Cutaneous Carcinomatous Lymphangitis (CCL) is one of the rare clinical forms of cutaneous metastasis that generally occurs late in the history of the cancer. It is generally misrecognized and wrongly treated as antibiotic-resistant erysipele. Clinically, lesions are polymorphic and mimicking different skin diseases, thus delaying the diagnosis and the treatment. We report a case of CCL with atypical lesions.
Skin metastases accounts for 2% of all metastases. During breast carcinoma, they occur in 23.9% of patients [1]. They can have polymorphic and confusing clinical features. Carcinomatous lymphangitis is one of the rare clinical forms that generally occur late in the history of the cancer. Furthermore, it can sometimes inaugurate the underlying malignancy as in the case of our patient. We report a case of Cutaneous Carcinomatous Lymphangitis (CCL) associated with keratosis and necrotic lesions that revealed invasive breast adenocarcinoma.
Skin metastases accounts for 2% of all metastases. During breast carcinoma, they occur in 23.9% of patients [1]. They can have polymorphic and confusing clinical features. Carcinomatous lymphangitis is one of the rare clinical forms that generally occur late in the history of the cancer. Furthermore, it can sometimes inaugurate the underlying malignancy as in the case of our patient.We report a case of Cutaneous Carcinomatous Lymphangitis (CCL) associated with keratosis and necrotic lesions that revealed invasive breast adenocarcinoma.
This is a 42-year-old woman, living in the countryside and without any particular antecedents, who presented 8 months before her admission a swelling of the right upper limb. She was treated several times as a bacterial hypodermatitis but without any favorable response. The symptomatology has recently been aggravated by the appearance of keratosisand necrotic plaques with extension of the edema to the right half of chest. On general examination, the patient was cachectic with respiratory dyspnea. Dermatological examination found an erythematosus, infiltrated and sclerotic plaque spread over the entire right chest and the right arm andulcerating and necrotic areas (Figure 1). Lymphedema was very important, extending up to the arm, forearm and hand (Figure 2). Examination of the right axillary lymph node area was difficult. Breast examination showed a nodule sitting in the inferior-internal lobe of the right breast, not well limited, with sclerotic and red skin in regard. A skin biopsy performed at the periphery of an ulcerating areas was in favor of a cutaneous localization of an invasive breast carcinoma with presence of lymphatic vascular emboli. Trans-cutaneous biopsy of the breast nodule confirmed invasive breast adenocarcinoma with an immune histochemical study showing a positivity for cytokeratin 7 (CK7+) and a negativity for cytokeratin 20 (CK20-). Hormone receptors were negative. The extension assessment showed a right pleural effusion with secondary lytic bone lesions. Chemotherapy has been recommended for our patient, but her condition deteriorated and she died in the month following.
The incidence of skin metastases in patients with metastatic cancer is by about 5% [1-4]. This skin damage may be secondary to a direct extension of the tumor (in 40% of cases) or metastases (60% of cases) which may be regional, in transit or distal [1]. During breast cancer, skin involvement can take different forms: nodular metastases, Paget's disease, breast carcinoma "en cuirasse", alopecia neoplastica, palpebral metastases or intravascular skin metastases. This last form is rare and in which we distinguish two types: the first related to the tumor invasion of dermal blood vessels "lymphangioma-like plaque". The second is cutaneous carcinomatous lymphangitis, related to the invasion of the dermal lymphatic pathways and leading to lymphatic blockage that is at the origin of the localized lymphedema and the "orange peel" appearance simulating a hypodermatitis process [3,4]. The cancers implicated are mainly breast carcinomas but also endometrial, pancreatic, rectal, pulmonary, ovarian and parotid ones [5]. Clinically, lesions are polymorphic and mimicking different skin diseases (erysipela, radio-induced dermatitis, eczema...), thus delaying the diagnosis and the treatment. Lesions can be located on the breast skin or remotely and are erythematous, hot, painful, erysipela-like (hence the term "erysipelatoid"). Their clinical appearance changes slowly after several weeks; the skin may acquire a yellow color and fibrous texture [6]. These clinical features, apyrexia and white blood cell normality should assist in the diagnosis of a non-infectious process [7].
Confirmation of the diagnosis of CCL is histologic; metastatic tumor cells are closely related to superficial and deep dilated lymphatic vessels with a slight perivascular infiltrate made of lymphocytes and plasma cells [1]. The treatment is that of primary cancer, which sometimes leads to clinical remission, but the prognosis of these patients is generally poor [2].
Our case illustrates the importance of recognizing this entity in the absence of improvement of erysipela-like lesions, and thus avoiding anti-inflammatory treatment or prolonged empirical antimicrobial therapy that would delay correct diagnosis.
The authors declare that they have no competing interests.
All the co-authors contributed to the realization of this work, read and approved the final manuscript.
Written consent for publication of this article has been obtained from our patient.
Nil.
None.

Figure 1: Polymorphic lesions: ulcerous, keratotic and necrotic areas.
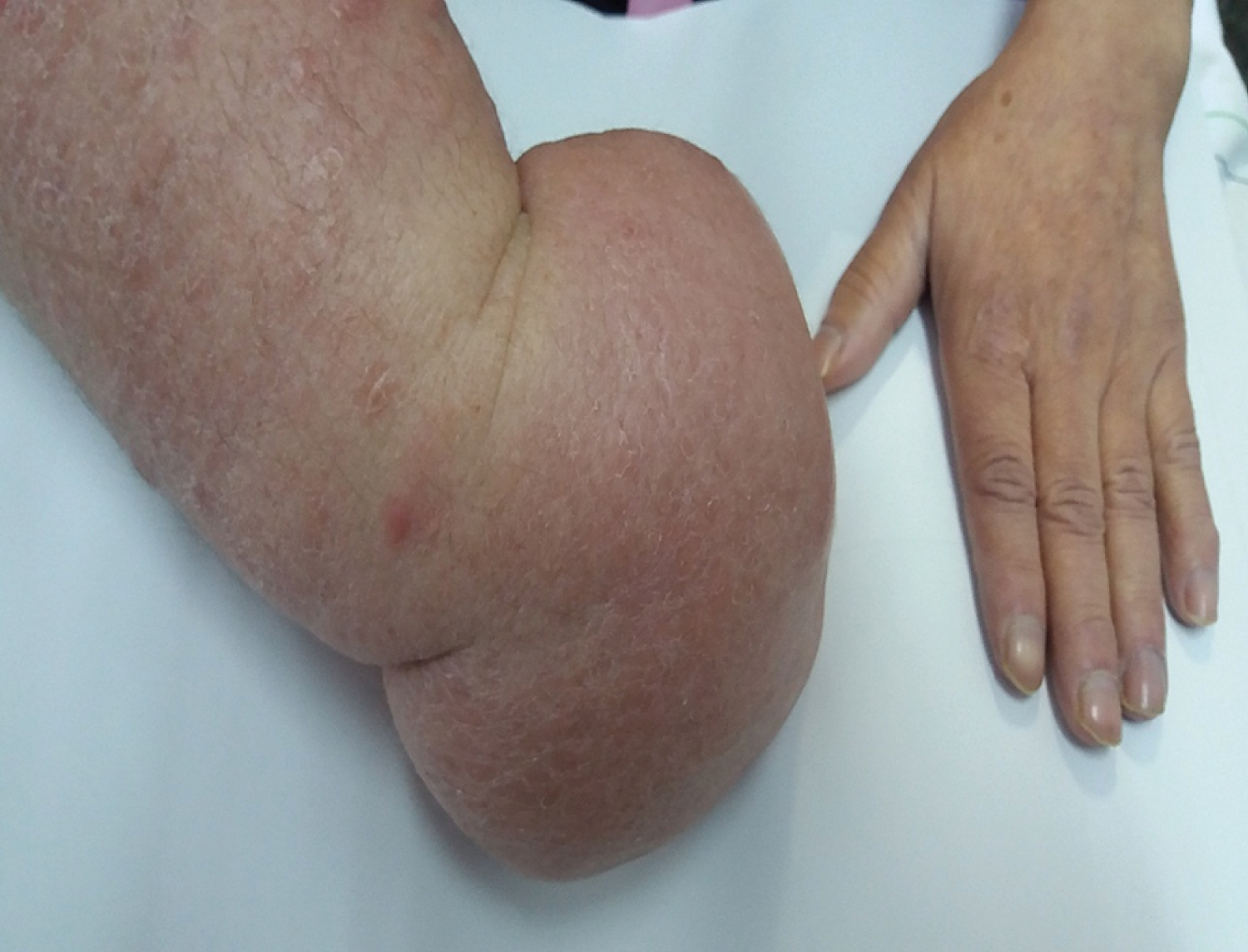
Figure 2: Significant lymphedema of the entire upper limb.