A 52-year-old male was admitted for abdominal pain. He had a personal history of tobacco. The physical examination and laboratory tests were normal. A thoraco-abdominal computed tomography scan (CT) reveals a combination of a thin walled pulmonary cystic lesion, and an hepatic hypodense subcapsular lesion (Figure 1). No other abnormalities were showed. The liver magnetic resonance imaging (MRI) showed a normal sized liver with regular contours and multiple nodular lesions (Figure 2). We completed by liver biopsy, that shows infiltration of large cells with irregular nuclei that positively stained to CD1a and S100 (Figure 3).
Langerhans cell histiocytosis (LCH) is a rare clonal pathology characterized by infiltration of Langerhans cells. The pathology can occur with the involvement of only one organ, but can have multi-visceral involvement [1]. New evidence suggests that LCH occurs as a consequence of misguided differentiation of myeloid dendritic cell precursors [2]. The definitive diagnosis requires a biopsy of the most accessible lesion for confirmation through histological examination and immune histochemistry [3].
Adult pulmonary LH occurs almost exclusively in young smokers or ex-smokers (90 to 100% of cases), equally in both sexes [4]. Liver involvement is seen in 15% to 20% of cases and presents as tumor-like or cystic lesions or as hepatomegaly [2].
Treatment of patients with LCH depends on the extent of the disease. Steroids may help to slow or even stop the progression of lung LCH and cessation of smoking is essential to prevent disease recurrence or progression. Chemotherapeutic agents, such as vinblastine, methotrexate, cyclophosphamide, etoposide, and cladribine have been successful in patients with progressive disease unresponsive to corticosteroids and in those with multiorgan involvement [5].
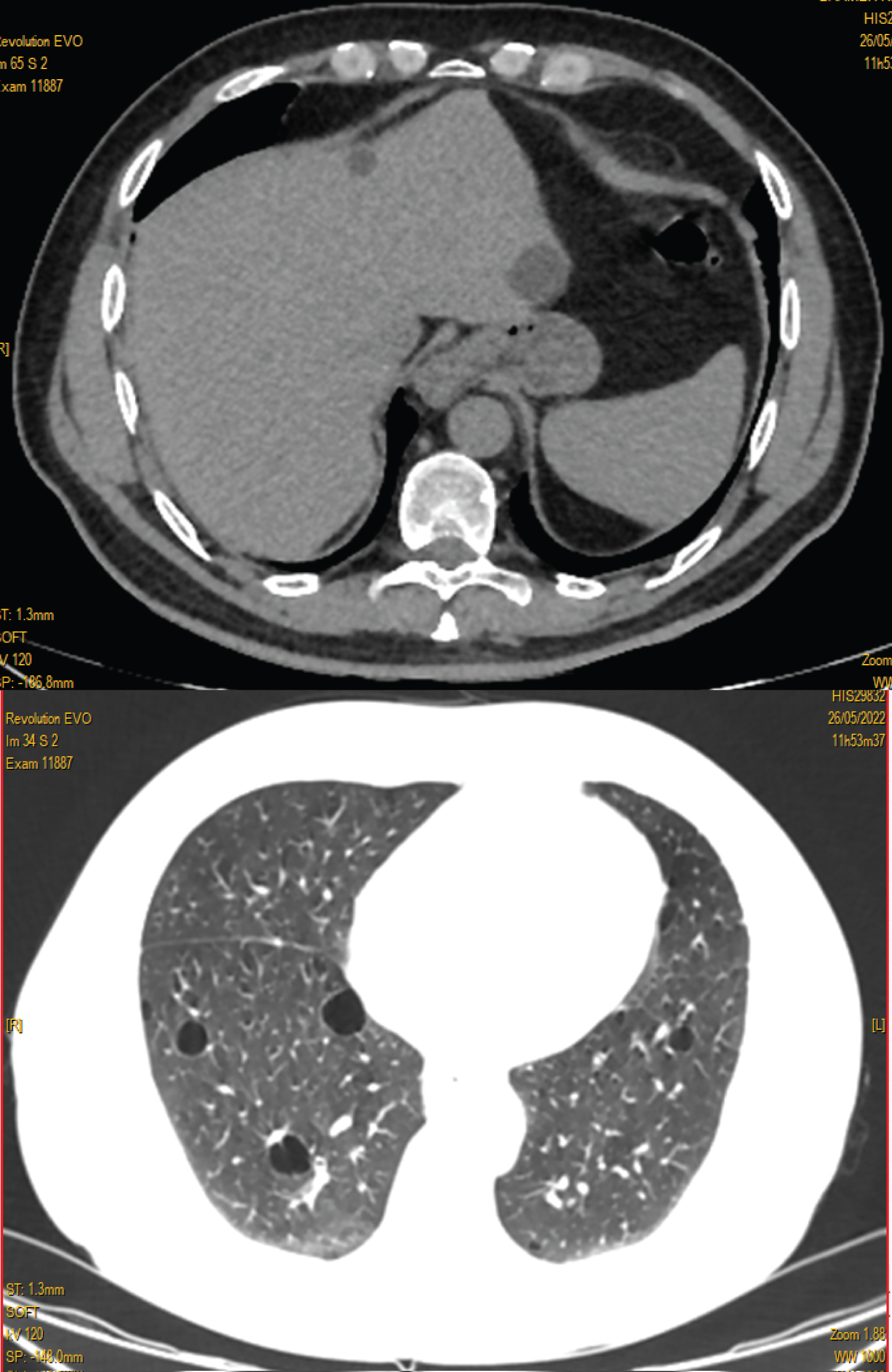
Figure 1: Thoraco-abdominal computed tomography scan (CT) showing an hepatic hypodense subcapsular lesion and multiple cysts in the lungs.
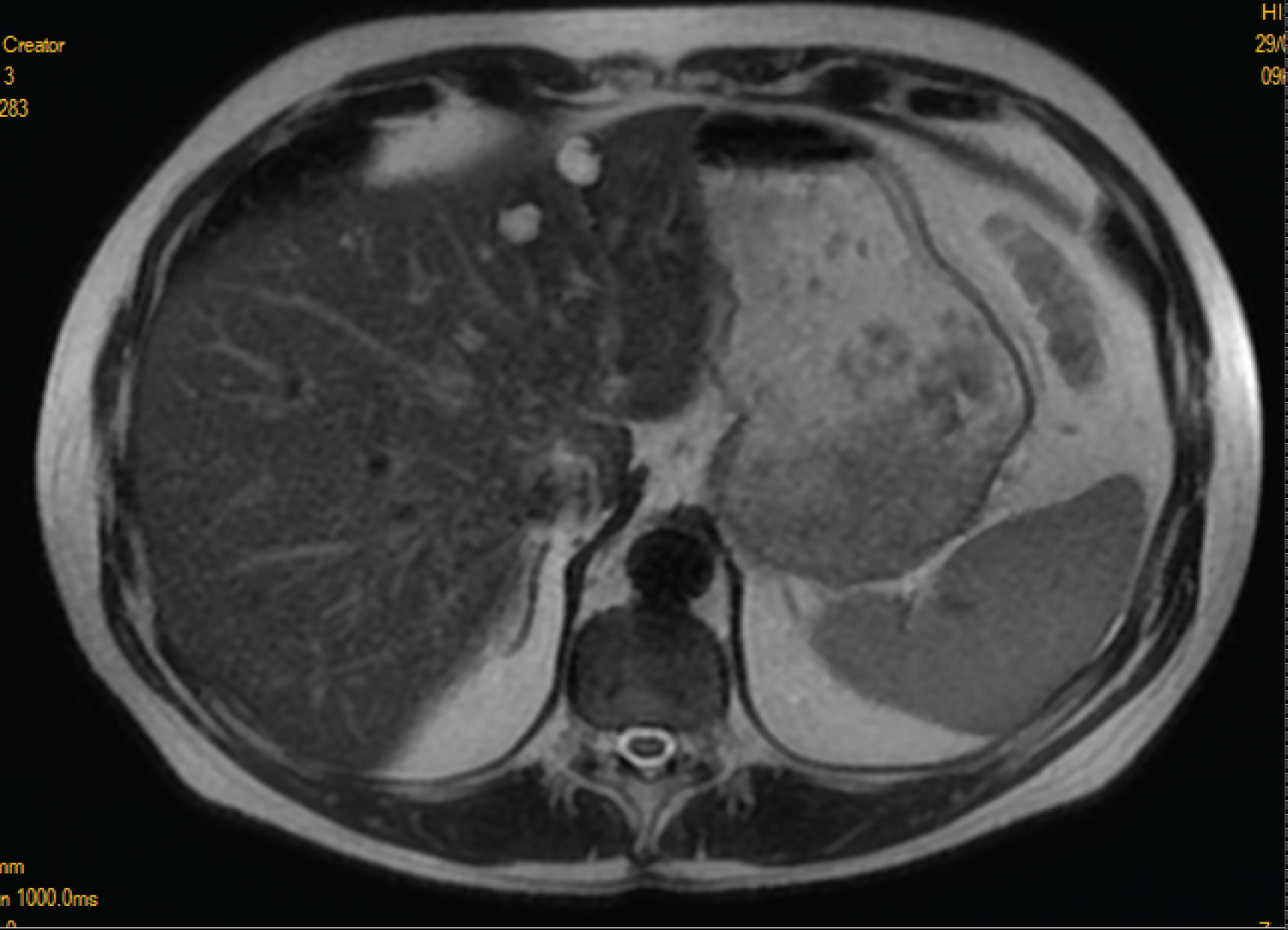
Figure 2: The liver magnetic resonance imaging (MRI) showing several nodular lesions.
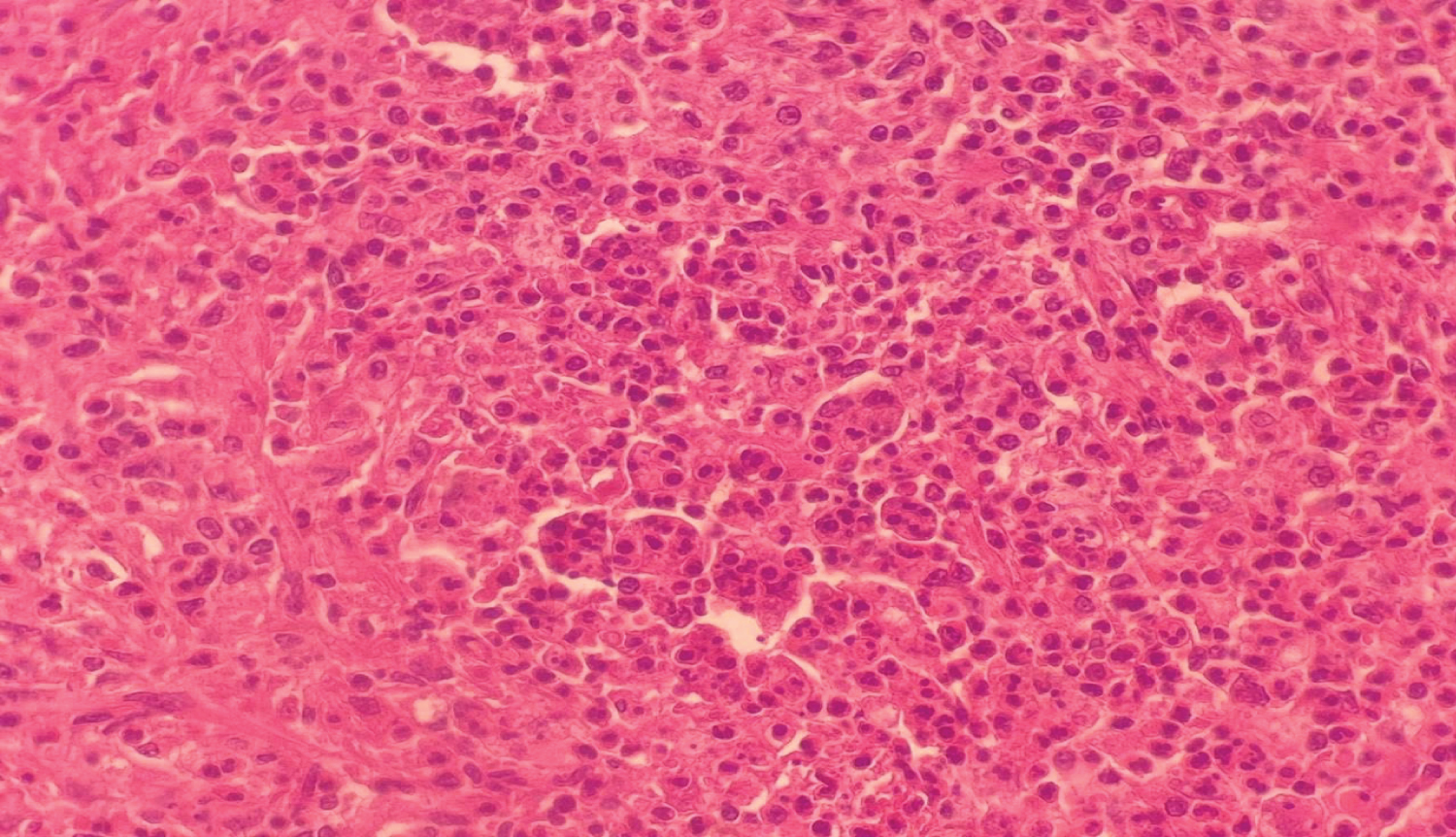
Figure 3: Histologic examination of a liver biopsy specimen.