Migration of intrauterine contraceptive device (IUCD) to adjacent organs is rare but the most serious complication. Withdrawal of any migrated IUCD is advisable even if asymptomatic and Laparoscopic removal remain the gold standard, however sometimes finding the device intra-operatively is challenging for the surgeon.
We report a case of laparoscopic removal of migrated IUCD to the sigmoid colon. Computed tomography (CT) precisely located the migrated device embedded in the sigmoid colon. After failure of endoscopic attempt to remove the device, laparoscopy was then performed. On initial laparoscopic examination no adhesions were found, the uterus, ovaries & tubes were normal in appearance, however a small bud was identified on the anterior surface of the descending branch of the sigmoid colon. This bud was related to one arm of the T shaped IUCD in fluoroscopy. During dissection around the bud fortunately one arm of the device was seen and then the IUCD was easily extracted, then separate stitches were done to suture the opening of the colon. Postoperative outcomes were uneventful.
Migrated IUCD can be removed safely by laparoscopy. Preoperative precise localization is accurate and Intraoperative fluoroscopy guidance is helpful to find the missed device.
Intrauterine contraceptive device, Perforation, Migration, Sigmoid, Laparoscopy
IUCD: Intrauterine Contraceptive Device; CT: Computed Tomography
Intrauterine contraceptive Device (IUCD) widely used since 1965 because of their safety and effectiveness [1]. However perforation, rare but most serious complication, occurs approximately 1 in 1000 insertions [2]. Migration to adjacent organs is also well-known. Retrieval in such situation depends on the location of the migrated intrauterine device and evolves endoscopy, laparoscopy or sometimes (if required) laparotomy. We present here a case of totally migrated IUCD into the sigmoid colon, successfully removed laparoscopically.
A 38-year-old woman have had a copper T IUCD placed easily 6 years ago, but the patient became pregnant few months later. The patient reported that ultrasound at this time was normal and the device was not visible. The pregnancy was conducted to term and she delivered vaginallay without any complications. Diagnosis of IUCD drop was considered, and the patient has never consulted. She had been completely asymptomatic until recently she developed an abdominal discomfort, slight left iliac fossa and back pain. Pelvic ultrasonography revealed a normal appearing uterus. Abdominal X-ray revealed that the IUCD is seen above the pelvis (Figure 1). The diagnosis of IUCD migration was suspected and computed tomography was ordered wish showed migration of the T copper device totally to the sigmoid colon (Figure 2). Colonoscopy was done to assess the possibility of endoscopic extraction of the device, but failed because of inflammatory stenosis and the T arms were invisible to the endoscopist witch suspected that the device is impacted in the rectosigmoid wall. Necessary consent was obtained for laparoscopy and possible laparotomy. Laparoscopy was then performed. On initial laparoscopic examination the uterus, ovaries & tubes were normal in appearance, no adhesions were observed due to inflammation around the device. However a small bud was identified on the anterior surface of the descending branch of the sigmoid colon (Figure 3a). This bud is related to one arm of the T shaped IUCD in fluoroscopy (Figure 4). During dissection around the bud fortunately one arm of the device was seen (Figure 3b) and then the IUCD was easily extracted, then separate stitches were done to suture the opening (Figure 3c). Postoperative outcome was uneventful and the patient was discharged on the second postoperative day. There was no recurrence of symptoms on subsequent follow-up.
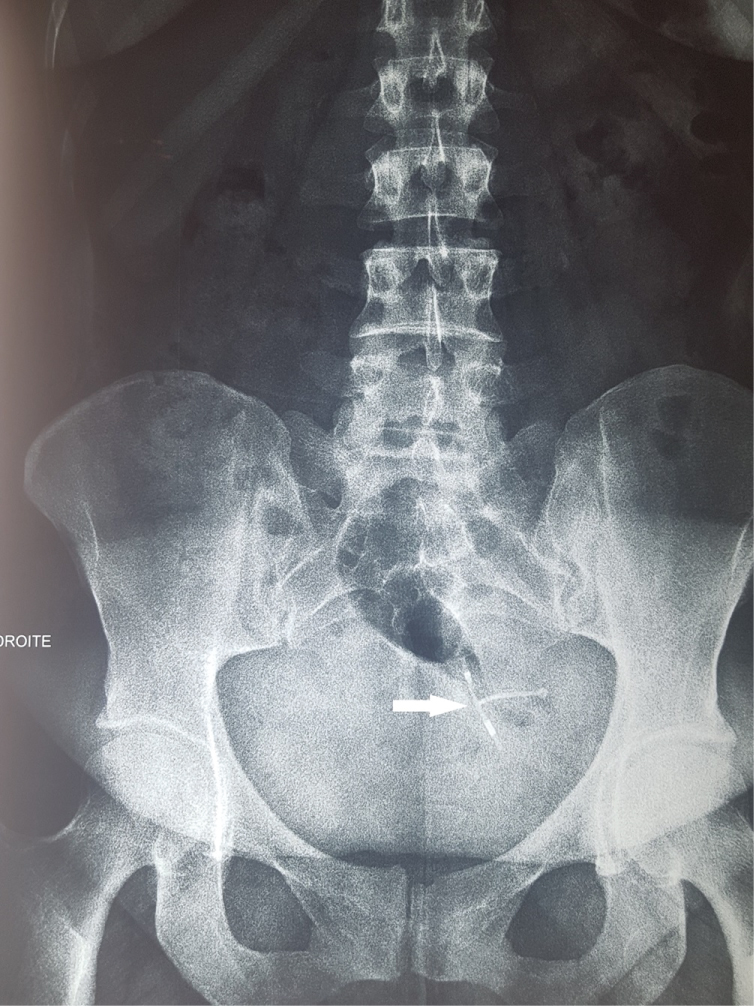 Figure 1: Migrated IUCD appearance in plain abdominal X-Ray: White arrow.
View Figure 1
Figure 1: Migrated IUCD appearance in plain abdominal X-Ray: White arrow.
View Figure 1
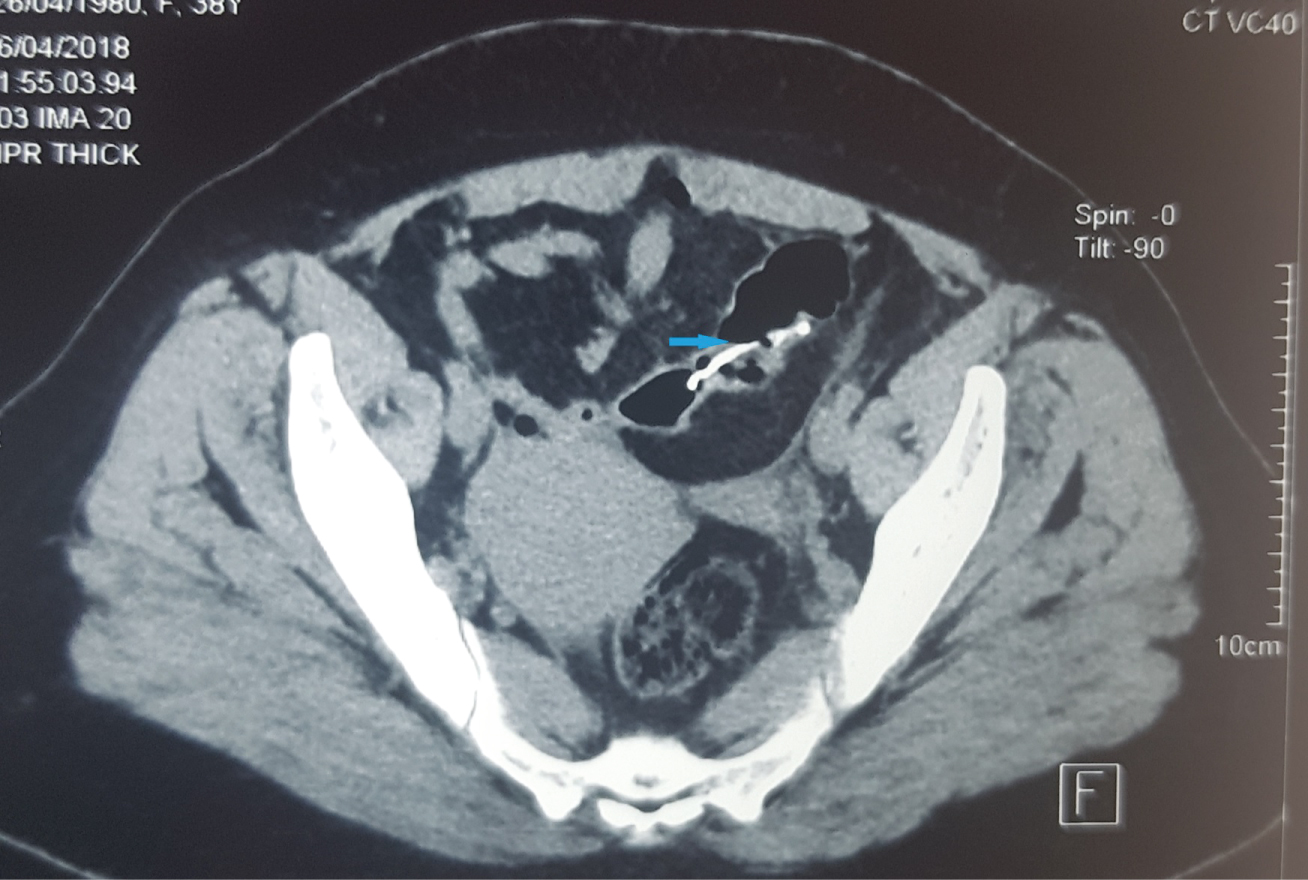 Figure 2: CT scan showing the IUCD in the sigmoid colon: Blue arrow.
View Figure 2
Figure 2: CT scan showing the IUCD in the sigmoid colon: Blue arrow.
View Figure 2
 Figure 3: Intraoperative view: a) A small bud seen in the anterior surface of the sigmoid colon (white arrow); b) Removal of the migrated IUCD from the colon; c) Colon appearance after suture.
View Figure 3
Figure 3: Intraoperative view: a) A small bud seen in the anterior surface of the sigmoid colon (white arrow); b) Removal of the migrated IUCD from the colon; c) Colon appearance after suture.
View Figure 3
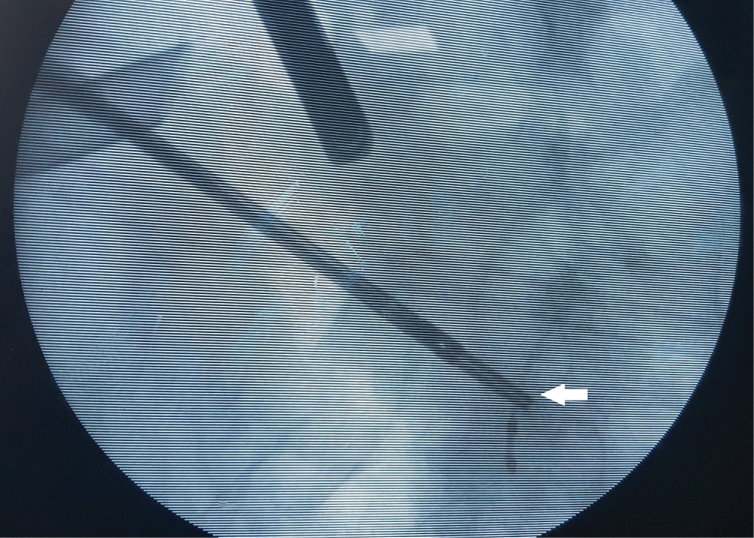 Figure 4: Fluoroscopy: The grasper holds one of the arms of the IUCD (white arrow).
View Figure 4
Figure 4: Fluoroscopy: The grasper holds one of the arms of the IUCD (white arrow).
View Figure 4
IUCD is a popular and safe reversible contraceptive method, but complications such as bleeding, infection, ectopic pregnancy and perforation and migration can occur. Uterus perforation and migration of the IUCD is uncommon but serious complication [3].
Although in 90% of cases misplaced IUCD is recognized in the first year after insertion [4], it can remain totally asymptomatic for a long period such in the present case witch remained asymptomatic for 6 years, after that the patient developed pain. Symptoms depend on the location of the IUCD. Patients in whom the device has migrated to rectum or sigmoid colon frequently develop abdominal pain [5].
The mechanism of migration still unclear, but the incidence seems to be influenced by several factors such as timing of the insertion, the parity, a history of previous abortions, the type of and the experience of the operator [6].
Uterine ultrasound coupled to abdominopelvic radiography is enough to carry the diagnosis of misplaced IUCD. Indeed an IUCD which is not "in place" on ultrasound and seen on radiography is misplaced until proven otherwise. Computed tomography helps in locating precisely IUCD that has migrated outside the uterus [7]. It is widely recommended to withdraw any displaced or migrated IUCD even if asymptomatic because of the risk of complications such as fistula formation and perforation of adjacent organs [8]. There are many ways to retrieve a displaced IUCD depending on its location. This can be achieved endoscopically, laparoscopically, laparotomy or combination of two techniques [9-10]. Endoscopic retrieval is feasible and safe [1,2,11] and it was attempted in our case but failed because the device was not visible at endoscopy, probably covered by colonic mucosa and inflammatory changes. There are no complications related to endoscopic retrieval that have been reported in the literature, this is probably due to the fact that the perforation is clogged by inflammatory changes. In laparoscopy, sometimes it is difficult to find the migrated IUCD, especially when the device has already passed the wall of a hollow organ, therefore accurate preoperative localization is advised. Precise preoperative localization is also helpful for the surgeon for the choice of patient position on table and trocars placement. For the present case, the device was localized preoperatively in the sigmoid colon, that's why we have chosen to put the patient in position as for sigmoid colon resection. Gill, et al. reported a conversion rate to laparotomy of 34.6% in a systematic review and adhesions were reported to be present in the majority of cases requiring laparotomy [4]. Often the device can be seen easily in the first laparoscopic view, but sometimes the first laparoscopic view is totally normal. In such situation fluoroscopy may be very helpful to the surgeon. In our case the only abnormality found in the laparoscopic view was a small bud on the anterior surface of the sigmoid colon; this was effectively related to the migrated IUCD as shown by Intraoperative fluoroscopy.
Perforation and migration is a rare but serious complication related to IUCD insertion. This prompts us to check carefully every time after device insertion and annual monitoring. Precise preoperative localization is accurate, better with computed tomography. Laparoscopic removal is feasible and safe. Surgeon should not hesitate to use helpful tools such as fluoroscopy guidance if available.
Not applicable.
Written informed consent was obtained from the patient for the publication of this case report and related images.
The dataset supporting the conclusions of this article is included within the article.
Not applicable.
AY and HZ performed the operation. AY, NH and HB drafted the manuscript. SR, CM and HO participated in the conception, design, and analysis of this case report. AZ was the chief supervisor and gave the final approval of the article. All authors read and approved the final manuscript.
Not applicable.
The authors declare that they have no competing interests.