Convulsive Syncope can be difficult to distinguish from seizures at times. We present a young adult with cardiogenic convulsive syncope that mimic seizures. Continuous cardiac monitoring revealed various arrythmias during seizure like activity. She had a viral prodrome. Cardiac MRI was diagnostic for myocarditis. More detailed studies for the role of a noninvasive cardiac testing such as Cardiac MRI (CMR) and newer treatment modalities such as anti-thymocyte immunoglobulin are required for the management of Viral Myocarditis.
A 32-year-old female was brought to the Emergency Department after a cardiac arrest at work. She was found to be pulseless, so three rounds of CPR were performed, and four shocks were delivered. While in hospital she had multiple episodes of arrythmias associated with pulselessness requiring transvenous pacing. She had a prodrome of viral illness and transferred to a tertiary care center for cardiac MRI and placement of an Implantable Cardioverter Defibrillator (ICD). Cardiac MRI revealed signs of early myocarditis.
Differentiating Cardiovascular Convulsive syncope from Seizure has always been a dilemma [1,2]. We describe a case of a previously healthy young woman presenting with a sudden onset of intractable Stokes Adam Attack. Vasovagal syncope is the most likely etiology of syncope in young women [1]. However detailed history taking in our patient revealed a prodrome of viral illness. Later found to have myocarditis on cardiac MRI. Myocarditis can have variable presentation [1,3]. This case depicts life threatening arrythmias that present as seizure like episodes. The arrythmias caused as a sequela of myocarditis.
A 32-year-old female was brought to Emergency Department after a cardiac arrest at work. As per coworkers she suddenly collapsed and had seizure like activity. She was found to be pulseless, so three rounds of CPR were performed, and four shocks were delivered. Return of spontaneous circulation was achieved. She reverted to full consciousness spontaneously within minutes without confusion or cognitive deficits. On further enquiry she admitted a one-week history of fever and cough. She was evaluated in an Urgent care center and sent home on Pseudoephedrine.
En route to the hospital she was noted to have a BP of 90/60 mmHg and the cardiac monitor revealed polymorphic Ventricular tachycardia (VT), (Figure 1). She then had an episode of myoclonus and became unresponsive, went into asystole briefly then polymorphic VT then monomorphic VT (Figure 2), and finally into sinus tachycardia (Figure 3). Per EMS this lasted for about 15 sec.
 Figure 1: Electrocardiogram recorded by Emergency Medical Services showing Polymorphic Ventricular Tachycardia.
View Figure 1
Figure 1: Electrocardiogram recorded by Emergency Medical Services showing Polymorphic Ventricular Tachycardia.
View Figure 1
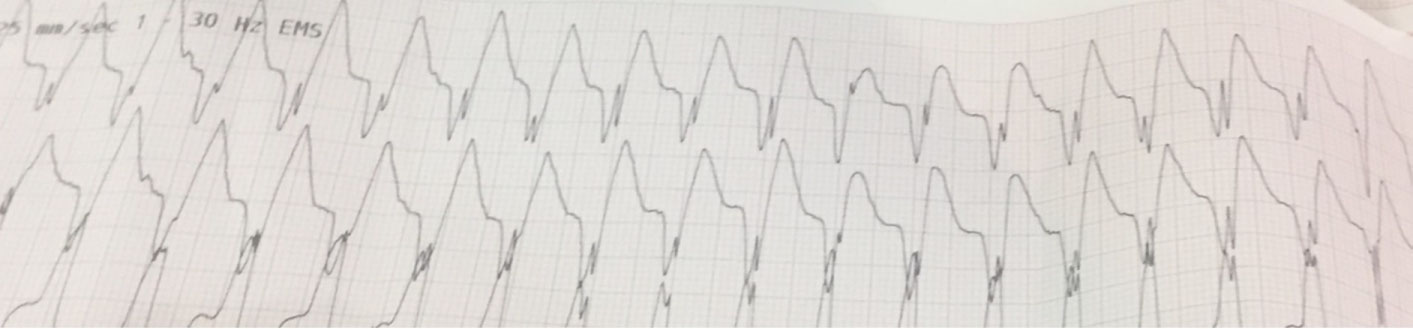 Figure 2: Electrocardiogram recorded by Emergency Medical Services showing Monomorphic Ventricular Tachycardia.
View Figure 2
Figure 2: Electrocardiogram recorded by Emergency Medical Services showing Monomorphic Ventricular Tachycardia.
View Figure 2
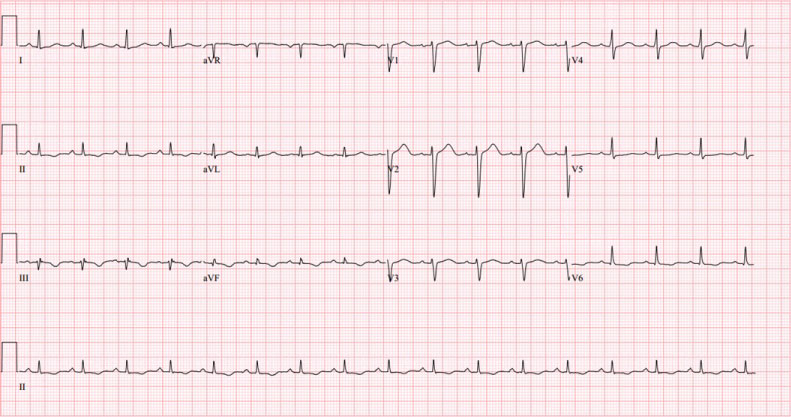 Figure 3: EKG showing Normal Sinus Rhythm.
View Figure 3
Figure 3: EKG showing Normal Sinus Rhythm.
View Figure 3
In the Emergency department, cardiac monitor showed non-sustained polymorphic ventricular tachycardia and then a sustained period of bigeminy quickly developing into polymorphic ventricular tachycardia with tonic movements of her arms and face and was pulseless. CPR and defibrillation were performed with resolution to sinus rhythm. She quickly regained consciousness. Total time of pulselessness was less than 30 seconds. Cardiac monitoring revealed frequent Premature Ventricular Contractions (PVC) (Figure 4). Point of care ultrasound was performed bedside, which showed mildly dilated left atrium and left ventricle with reduced left ventricular ejection fraction (Figure 5 and Figure 6).
 Figure 4: EKG recorded in the Emergency department showing Sinus Rhythm with frequent Premature ventricular contractions and prolonged QTc interval.
View Figure 4
Figure 4: EKG recorded in the Emergency department showing Sinus Rhythm with frequent Premature ventricular contractions and prolonged QTc interval.
View Figure 4
 Figure 5: Transthoracic Echocardiogram showing dilated Left atrium. LA Diameter: 2.6 cm.
View Figure 5
Figure 5: Transthoracic Echocardiogram showing dilated Left atrium. LA Diameter: 2.6 cm.
View Figure 5
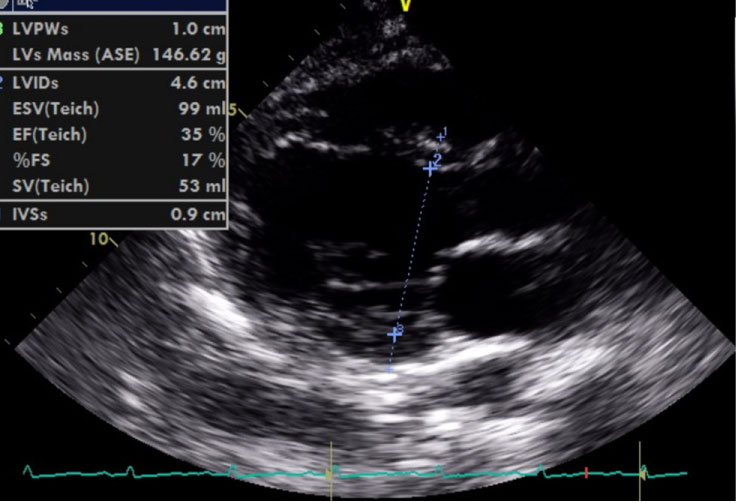 Figure 6: Transthoracic Echocardiogram showing Dilated Left Ventricle with reduced Ejection Fraction. Left Ventricular Ejection Fraction: 35 percent.
View Figure 6
Figure 6: Transthoracic Echocardiogram showing Dilated Left Ventricle with reduced Ejection Fraction. Left Ventricular Ejection Fraction: 35 percent.
View Figure 6
She was overdrive paced for a day (Figure 7). On telemonitoring, Rhythm was sinus rhythm with PVC. IV Amiodarone was also given to control ventricular arrythmias.
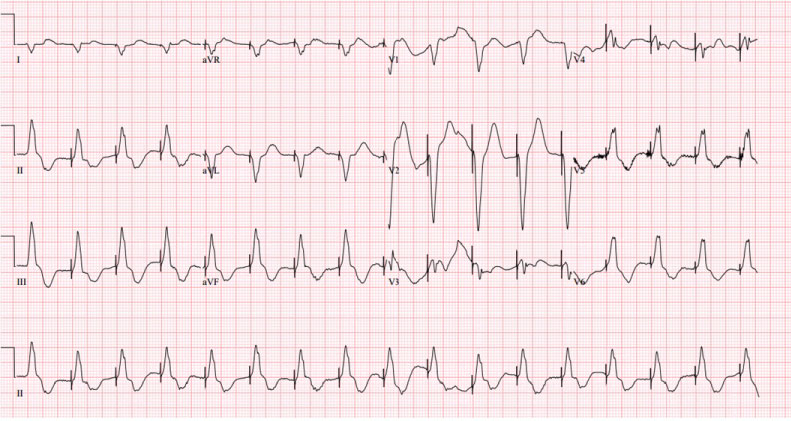 Figure 7: EKG showing Ventricular paced rhythm.
View Figure 7
Figure 7: EKG showing Ventricular paced rhythm.
View Figure 7
On day 2, TVP was removed and patient was transferred to a tertiary care center for a cardiac MRI. Cardiac MRI revealed Global myocardial SI increase in T2-weighted images and Increased global myocardial early gadolinium enhancement ratio between myocardium and skeletal muscle in gadolinium-enhanced T1-weighted image. A Subcutaneous Implantable Cardioverter Defibrillator (ICD) was placed for secondary prevention of arrythmias. Patient was discharged with close follow up.
This case describes a patient with classic Stokes Adam attack associated with a myriad of ventricular arrythmias in the setting of viral myocarditis.
Differentiating syncope from seizures can be difficult at times [1,2]. The Stokes-Adams attack, a form of cardiovascular syncope, classically described as an abrupt, transient loss of consciousness due to a sudden but pronounced decrease in the cardiac output, which is caused by a paroxysmal shift in the mechanism of the heart beat [4].
Our patient exhibited generalized jerking and myoclonic movements on presentation. The loss of muscle tone (atonia) resulting in sudden collapse, the absence of post ictal phase, prompt return of consciousness favors syncope over seizure in our patient [1,2].
Treatment of myocarditis consists of both specific therapy aimed at the cause of the myocarditis and supportive treatment to control Heart failure and arrhythmias [3,5,6]. The Heart Failure Society of America 2010 comprehensive heart failure practice guideline recommends considering endomyocardial biopsy for patients with acute deterioration of heart function of unknown origin that is not responding to medical treatment [6].
It is a common case scenario where patients are dismissed from urgent care centers with common cold remedies to have to return with life threatening Myocarditis/Bacterial superinfections [3]. Unfortunately, we do not have any predictive methods to triage these patients on initial presentation at urgent care centers.
Literature reveals various presentations of Stokes Adam Attack. A myriad of arrythmias are associated with it. AV blocks are more commonly associated than Ventricular arrythmias [4,7]. This case emphasizes the importance of thorough history from multiple available sources because intractable Stokes Adams can mask an underlying heart conditions such as infection.
Cardiovascular magnetic resonance (CMR) has become the primary tool for noninvasive assessment of myocardial inflammation in patients with suspected myocarditis. The International Consensus Group on CMR Diagnosis of Myocarditis provides CMR protocol standards, terminology for reporting CMR findings, and diagnostic CMR criteria for myocarditis (i.e., "Lake Louise Criteria") [8].
Current standard treatment of viral myocarditis is supportive care, although immunomodulatory therapies, such as steroids and intravenous immunoglobulin, are often used [6,9]. A systematic review concluded that there are insufficient data from methodologically strong studies to recommend routine IVIG therapy in patients with acute myocarditis. However, there are no controlled randomized data on IVIG in pediatric or adult patients with acute or chronic myocarditis or Dilated cardiomyopathy with biopsy-proven viral or autoreactive myocardial inflammation [9].
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.