Hypertension (Blood pressure ≥ 140/90 mmHg) is the modifiable risk factor responsible for a host of complications. Evidence based guidelines are important for prevention and control of hypertension. However, there is variation and inconsistencies among published guidelines concerning, diagnosis and treatment approach. Therefore, this review was conducted with intension to evaluatequality and comprehensiveness of published national adult hypertension treatment guideline, diagnosis and treatment approach in comparison with other national and international guidelines.
We selected national guidelines of five countries (USA of America, Canada, Europe, Australia and Ethiopia) and one international guideline.We used clinical guideline appraisal tool to evaluate the quality of guidelines, and comprehensiveness of the guidelines was evaluated by using a tool developed reach team.
We qualitatively synthesized the evidence by reviewing quality and comprehensiveness ofselected guidelines.
National adult hypertension treatment guideline of Ethiopia addressed only 22 (64.7%) of quality appraisal tool components. The guideline is least comprehensive 15 (51.7%). Major problems the guideline were; lack of diagnostic approach for masked, white-coat and resistant hypertension; failure to address child hood risk factors and secondary cases of hypertension. Similarly, management of hypertension in patients undergoing surgery, specific patient groups, access to medicine and social determinants of health are not addressed.
Quality and comprehensiveness of National hypertension guideline of Ethiopia is poor. Therefore, we recommend the guideline development committee and other relevant stakeholders to: update the blood pressure targets for elderly population, determine when to initiate and intensify antihypertensive drug therapy; address social determinants and socioeconomic status of population including maternal nutrition and Access of medicines.
Hypertension treatment guidelines, Management of hypertension in adults, Evidence based guideline, Ethiopia
ABPM: Ambulatory Blood Pressure Monitoring; ACC/AHA: American College of Cardiology/American Heart Association; AGREE: Appraisal of Guidelines for Research &Evaluation; ASCVD: Atherosclerotic Cardiovascular Diseases; CHD: Coronary Heart Disease; CKD: Chronic Kidney Disease; CVD: Cardiovascular Diseases; ESC/ESH: European Society of Cardiology/European Society of Hypertension; ESRD: End Stage Renal Disease; FGR: Fetal Growth Restriction; HBPM: Home Blood Pressure Monitoring; HF: Heart Failure; JNC: Joint National Committee guideline for management of raised blood pressure in adults; LDL-C: Low Density Lipoprotein- Cholesterol; MI: Myocardial Infarction; NCDs: Non-Communicable Diseases; PAD: Peripheral Arterial Disease; SPC: Single Pill Combination; SPRINT:Systolic Blood Pressure Intervention Trial; TIA: Transient Ischemic Attack
Hypertension (Blood pressure ≥ 140/90 mmHg) is the modifiable risk factor responsible for host of complications. Starting at a blood pressure of 115/75 mmHg, every increase of 20 mmHg in systolic blood pressure (SBP) and/or increase of 10 mmHg in diastolic blood pressure (DBP) is associated with a doubling of the risk of death from stroke, heart disease, or other vascular disease [1].
Despite availability of evidence based interventions success in blood pressure control is poor globally [2]. The average Blood pressure (BP) of global adult population is above normal and less than 20% of people with hypertension have controlled their blood pressure [2-4]. Hypertension prevention and control in SSA is the worst in kind, fewer than 5% of those with hypertension had achieved control of their condition in SSA [5].
Prevalence of hypertension among adults increased alarmingly from 9.3% in 2011 to 19.6% in 2015 in Ethiopia [6-8]. Only 28.4% of patients were on antihypertensive medication [7]. According to the WHOSTEPs survey, 97% of hypertensive patients in Ethiopia do not receive appropriate preventive care or treatment, with only 2.8% receiving treatment and 1.5% having their hypertension controlled [9,10].
Hypertension is the direct and indirect contributor of premature mortality in Ethiopia. For example; 39,571 stroke related deaths, 4,875 kidney disease related deaths, 46,943 coronary heart disease related deaths and 11,050 hypertension related deaths were reported in 2017 [11].
The world has started new movement to reduce premature mortality from non-communicable diseases. One of these movements is achieving 50% blood pressure control by 2030 from 2016 baseline (i.e. 14%) [12]. Movement towards this target will be probably ambitious unless something is done concerning management of hypertension at national level. Reviewing the existing chronic care policies and guidelines could be a good starting point. Studies indicated that adherence to evidence based guidelines, and improving access to basic medicines are important for prevention and control of hypertension [13]. Therefore, this review was conducted with intension to evaluate quality and comprehensiveness of national hypertension treatment guideline ofEthiopia to provide comprehensive care for adults with hypertension.
We included management of high blood pressure in adults (chapter four) of guidelines on clinical and programmatic management of major NCDs in Ethiopia, word heart health initiative guideline for management of CVDs, American college of cardiology guideline, Australia guideline for the diagnosis and management of hypertension in adults, hypertension Canada guideline and European society of hypertension guideline [12,14-18]. We used clinical guideline appraisal tool containing 34 questions to evaluate the quality of guidelines [19-22] and protocol of adapting guidelines for local context [23]. We developed seven guideline content evaluation tools (containing 29 sub-components) to assess the comprehensiveness of adult hypertension management guideline of Ethiopia.
• Availability of multidisciplinary guideline line development committee
• Availability of multidisciplinary guideline adaptation committee and experience of applying ADAPTE process when necessary
• Clear evidence generation process by involving methodologists for analysis and interpretation of findings
• Availability of the recent update in English language
• Universal acceptability of the guideline (i.e. world heart initiative guideline for management of hypertension).
We qualitatively synthesized the evidence by using the following approach. First we reviewed guideline development process, adaptation process, quality and comprehensiveness of guidelines. Secondly we presented the important recommendations concerning management of hypertension and related comorbidities. Finally, we discussed the major identified gaps of Ethiopian national NCD guideline for management of hypertension in adults.
Evidence based guidelines can be developed or adapted from other countries. Generally, guideline development process should involve:establishing guideline development group, setting thescope, formulating review questions, identifying evidence, creating recommendations, writing draft, and sending the draft to stakeholder review, revising draft based on comments, preparing final guideline and setting review period [24-26].
HEARTs package and National guideline for major non-communicable diseases [27] are adapted from other evidence based guidelines. Clinically sound evidence based guidelines being used in one setting may be adapted for use in another country. However, adaptation process should involve clearly defined process to contextualize the guideline to specific country interest. ADAPTE is commonly used process to facilitate efficient adaptation of high-quality guidelines [23]. The goal of ADAPTE is to establish a standard of transparency and replicability of adapted guideline, hence, to improve confidence to promote the recommendations of the adapted guideline [23] (Table 1).
Table 1: Clinical guideline Adaptation Process based on ADAPTE Process. View Table 1
National hypertension treatment guideline of Ethiopia, satisfies only 12 (50%) of adaptation process steps. Major problems areas were; there was no assigned multidisciplinary guideline adaptation committee, lack of end-user involvement, and guideline selection criteria.In addition to this, quality, content, consistency and acceptability of each guideline were not appropriately assessed. Finally, the draft document was not communicated to stakeholders, and the feedback acknowledgement was not done [27].
Quality of clinical guidelines is critical for provision of appropriate care for patients who need it with reasonable cost. Quality clinical guideline should have the following components: information retrieval process, evidence evaluation form different perspectives, developingevidence based and clear recommendations [19-22].
Based on quality appraisal tool, Ethiopian national guideline has addressed only 22 (64.7%) questions of the quality appraisal tool [27] (Table 2). In addition to this, the guideline is the least comprehensive among guidelines evaluated 15 (51.7%) [27] (Table 3). This could be the contributing factor for probably the poorest blood pressure control among hypertensive patients. According to the WHOSTEPs survey, 97% of hypertensive patients in Ethiopia do not receive appropriate preventive care or treatment, with only 2.8% receiving treatment and 1.5% having their hypertension controlled [9,10].
Table 2: Quality dimensions and items for guideline appraisal. View Table 2
Table 3: Evaluation of hypertension guideline contents for providing comprehensive care for adult patients. View Table 3
Appropriate diagnosis of blood pressure is the first critical step in management of hypertension. Common errors that can occur during BP measurement include: Faulty BP apparatus (Cuff too smallor too large) and Patient Related [Pain or anxiety, Bladder distension, Acute smoking, caffeine, ethanol (< 2 hours)] and talking during BP reading) [1,28-30]. Generally, BP falls by 10-20% fromdaytime to nighttime, and this could be mainly explained by physical activity than a circadian rhythm [31].
A 24-hour ambulatory pressure monitoring is ideal method for hypertension diagnosis. This is because white-coat and masked hypertension can be identified, provide stronger prognostic evidence, and night-time readings can be recorded. However, it is expensive, less available, and not feasible in most countries [1].
Laboratory investigations are required as diagnostic aid or confirmatory. Common laboratory investigations include: measuring fasting blood glucose, complete blood count, lipid profile, serum creatinine with estimated glomerular filtration rate, serum electrolytes, thyroid-stimulating hormone, urinalysis and electrocardiogram, echocardiogram, uric acid and urinary albumin to creatinine ratio [1,18].
All guidelines agreed on importance of proper methods and timing of BP management for diagnosis of hypertension.However, Ethiopian national guideline did not address diagnostic work-up for white-coat and masked hypertension. It is important to know the prevalence of both white-coat and masked hypertension to provide appropriate care for patients with hypertension. Ignoring white-coat hypertension may lead over estimation of hypertension and unnecessary treatment. While, ignoring masked hypertension lead to under estimation of hypertension, delayed treatment initiation and associated complications.
There are two global guidelines for treatment and control of blood pressure in adults: Joint National Committee guideline for management of raised blood pressure in adults 7 and 8 (JNC 7 and 8) [32,33].
Global heart health (HEARTs) technical package [15] has similar hypertension diagnostic thresholds and targets of treatment with JNC 7 recommendations. National guidelineof Ethiopia adopted JNC 7 and 8 hypertension diagnosis thresholds and targets [27]. Concerning hypertension diagnosis thresholds, it included additional BP category (severe hypertension BP ≥ 180/110 mmHg). Similarly, it recommends BP targets of JNC 8 but increased age of targeting BP < 150/90 mmHg from ≥ 60 years to > 75 years [27] (Table 4).
Table 4: Comparison of Blood Pressure Targets and time to initiate pharmacologic treatment. View Table 4
Regarding Blood pressure targets, ACC and HEART's guidelines target BP < 130/80 mmHg for high risk and BP < 140/90 mmHg for others. Australia and Canada guidelines target BP < 120/80 for high risk, BP < 140/90 mmHg for others. Hypertension Canada targets BP < 130/80mmHg for diabetic patients. European cardiology and hypertension society targets < 140/90 mmHg in all patients, if treatment is tolerable < 130/80 mmHg, 120-129/< 80 mmHg for patients less than 65 years old and 130-139/< 80 mmHg in ≥ 65 years. Ethiopian guideline targets BP < 140/90 mmHg for adults 18-75 years and BP < 150/90 mmHg for patients above 75 years [1,12,14-18,34] (Table 4).
A Comprehensive treatment for hypertensive patients is believed to improve movement towards reduction of related morbidity and mortality. Comprehensive hypertension treatment approach should include due consideration to social determinants, non-pharmacologic and anti-hypertensive pharmacotherapy [35]. Despite this evidence there are inconsistencies and differences in treatment approach and when to treat hypertensive patients in published guidelines, because of which physicians sometimes have to individualize the therapy, based on specific patient characteristics and response to treatment [36].
Social determinants: Less attention is given to social determinants of health in the today's healthcare, despite their huge impact on health related patient outcomes. Findings from different literatures indicated that clinical care contributes only 10-20% to health outcomes of a person even in their best possible stand. Socioeconomic factors, health behavior and factors related to the physical environment are estimated to account for up to 80% of health outcomes [37].
Poverty cases difficulty for treatment recommendations (meal plan, medication, indoor pollution, etc.). Similarly, Populations living below the poverty level have higher prevalence of cigarette smoking and less likely to quit. Addressing poverty alone can improve life expectancy by (2-4-5.4 years) [38-42]. Spending on Education, with expanded coverage improves life expectancy on average by 1.19 years. Low level of education is associated risky behaviors like substance, unsafe sexual practice, and poor dietary management [43].
Nonpharmacological Interventions: Behavior and life style factors account for 30% of health related patient outcomes. Their effect may be more pronounced in case of chronic illness like hypertension [37]. The following nonpharmacological interventions are recommended as first line management for hypertension individually or in combination with antihypertensive drugs. These include; weight loss for obese and overweight individuals, healthy diet, reducing dietary Sodium, enhancing dietary potassium intake, physical activity and reducing harmful use of alcohol. [18,44-51]. Perfect adherence nonpharmacological therapy can reduce systolic blood pressure (SBP) on average by 36 mmHg for hypertensive patients.
Pharmacological treatment: Concerning when to initiate pharmacologic therapy for hypertension guidelines have slight variation. For example, Australia hypertension treatment guideline recommends initiating antihypertensive pharmacologic therapy at BP ≥ 120/80 mmHg for high-risk patients, ≥ 140/90 mmHg for moderate risk and ≥ 160 mmHg for low risk patients [16]. European Cardiology society guideline recommends initiation antihypertensive therapy if BP 130-139/80-89 mmHg for very high risk, after 3-6 months trial of lifestyle intervention if BP 140-159/90-99 mmHg and immediately for all patients if BP ≥ 160/100 mmHg [18].
Canada hypertension guideline has similar recommendation except that, initiating antihypertensive pharmacologic therapy for diabetic patients is at BP ≥ 130/80mmHg [17]. American Heart association guideline [1] and WHO HEART's package guideline [15] recommend initiating antihypertensive pharmacologic therapy at BP ≥ 130/80 mmHg for high risk patients and BP ≥140/90 mmHg for others. Ethiopian NCD guideline for major diseases recommends antihypertensive pharmacologic therapy for patients with BP ≥ 160/100 mmHg and BP ≥ 140/90 mmHg for high risk (i.e.10 year CVD risk 20-20%), patients with BP ≥ 140/90 mmHg for high risk and 10-year CVD risk below 20% should continue lifestyle management [27] (Table 4).
All guidelines agreed on use of angiotensin converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), beta-blockers, calcium channel blockers (CCBs), and diuretics (thiazides and thiazide-like drugs) as the basis of antihypertensive treatment strategies. Similarly, all guidelines recommended Combination treatment is recommended for most hypertensive patients as initial therapy. Preferred combinations should comprise ACEI or an ARB with a CCBs or diuretics (thiazides and thiazide-like drugs). If BP is not controlled with a two-drug combination, treatment should be increased to a three-drug combination, usually ACEI/ARB + CCB + thiazide, preferably as a single pill combination (SPC) [12,14-18].
Treatment algorithm and dose intensification: One of the important components of quality guidelines is providing simplified management protocol or algorithms in the form of tables, charts or graphs. We selected WHO HEART's technical package guideline as reference concerning treatment algorithm and antihypertensive drug dose intensification (Figure 1 and Figure 2). Providing guide when and how to intensify to drug treatment is important to improve BP control. However, this approach was not addressed in Ethiopian national hypertension guideline.
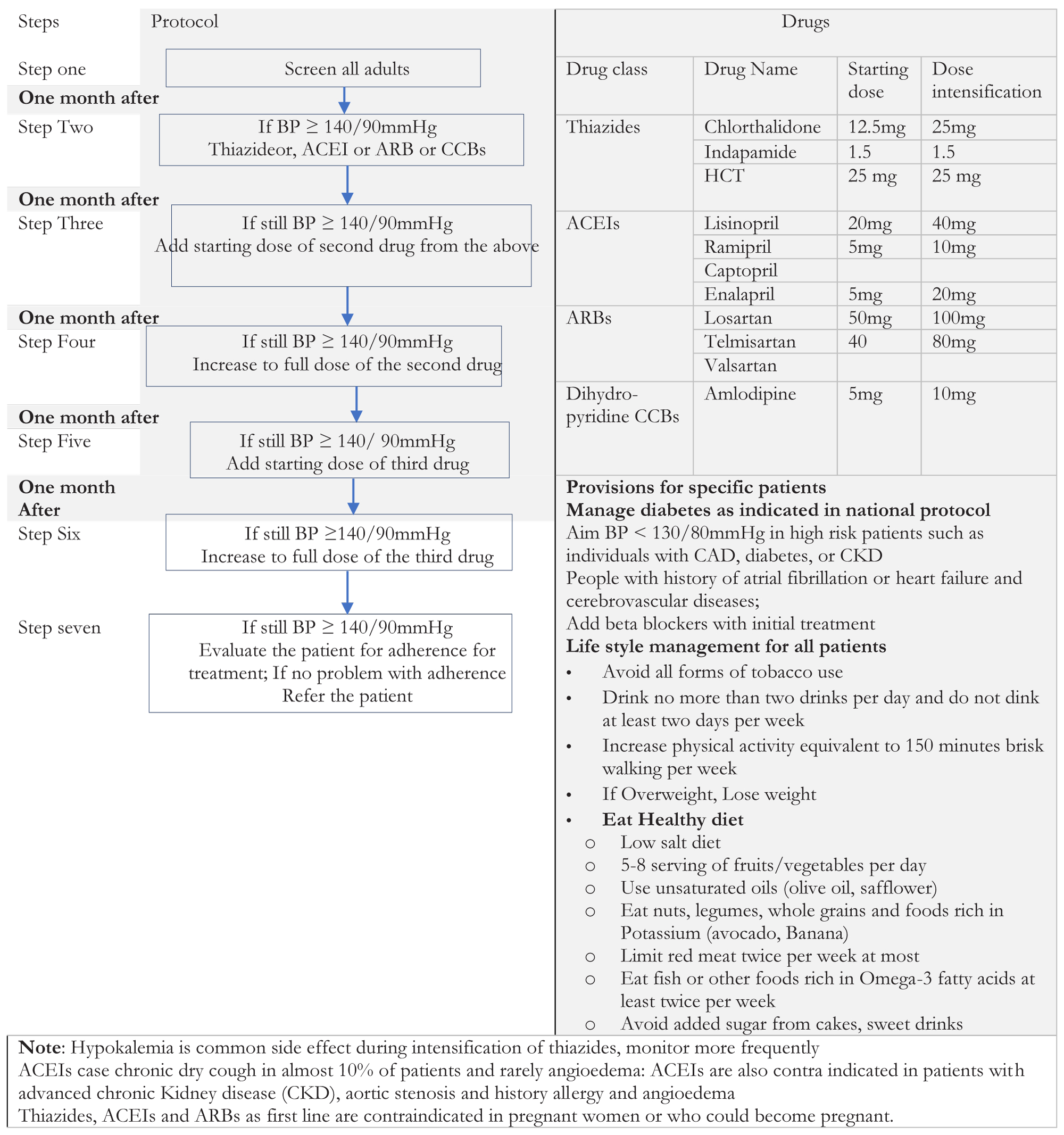 Figure 1: World Hypertension League and the International Society of Hypertension: Hypertension treatment Protocol by using single first line agent.
View Figure 1
Figure 1: World Hypertension League and the International Society of Hypertension: Hypertension treatment Protocol by using single first line agent.
View Figure 1
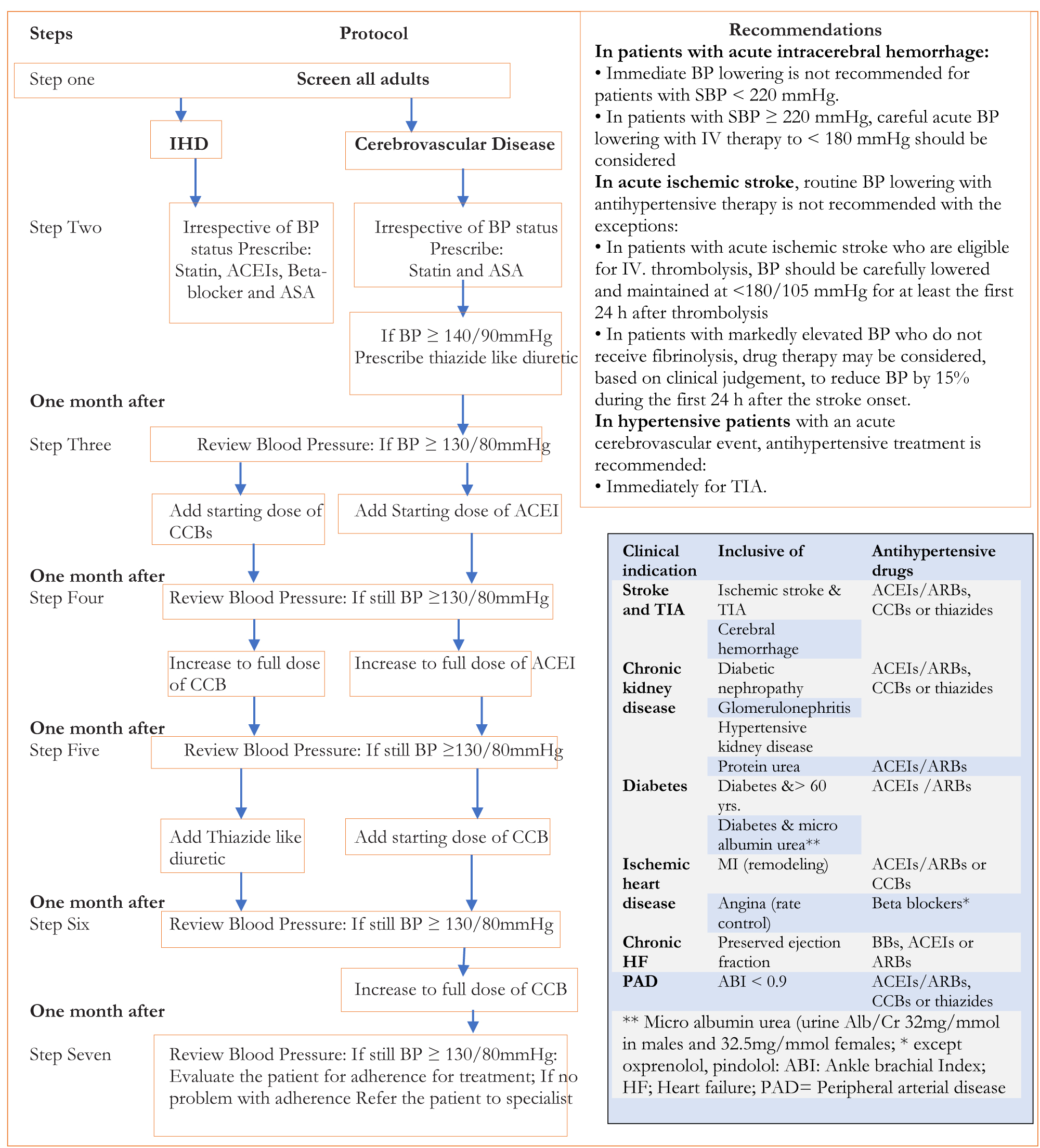 Figure 2: Protocol for treating patients with Ischemic heart disease by using of anti-hypertensive drugs.
View Figure 2
Figure 2: Protocol for treating patients with Ischemic heart disease by using of anti-hypertensive drugs.
View Figure 2
One of global voluntary targets NCD control is ensuring 80% availability of affordable and quality essential drugs for treatment of NCDs in both public and private facilities. However, According to the third national pharmaceutical sector survey median percentage availability of medicines used for chronic illnesswas 54.55% and none of essential medicines for NCDs are affordable [52]. This unaffordability of medicine is contributing poor adherence of hypertensive patients as evidenced by only 28.4% of hypertensive patients were taking medications prescribed by professionals. In addition to this, 15.6% individuals with raised BP (SBP ≥ 140 and/or DBP ≥ 90 mmHg) were not currently not on antihypertensive medication [7].
It is recommended to decrease out of pocket payment (OPP) to 15-20% of total health expenditure to make financial limitation to healthcare access. Out of pocket payment (OPP) expense was 33.8% in 2017 [50,53,54]. Given the poverty level of nearly one-quarter of the population in Ethiopia, it is likely that households who decide to use health services could easily slip into poverty. Thus, the government should improve coverage of community health insurance schemes which is under pilot in some regions. It should also start social health insurance for the formal sectors.
Healthcare service delivery system availability and readiness survey indicated that thegeneral service readiness index was 54%. Only 9% of facilities had guidelines for CVD diagnosis and management. The percentage availability trained staff for CVD diagnosis and management was 7%. Availability of Aspirin (53%), hydrochlorothiazide (37%), ACEIs (25%), calcium channel blockers (20%), metformin (19%) and beta blockers (15%). The percent of facilities with all of these items needed to provide CVD care was (1%) [9,55].
Another important factor that could affect blood pressure control in Ethiopia is Health worker density and distribution (per 10, 000 population) (2.7 in 2010 and 4.93 in 2016). This is 4.6 times less than the required global target recommended to effectively provide essential health services, meet the universal health coverage and health-related SDGs (i.e. 22.8/10,000) [56-58]. The effect this gap is clearly visible by showing that about 97% of hypertensive patients were not receiving appropriate preventive care [9,10].
In this review we evaluated five national guidelines and one international guideline used for management of high blood pressure in adults. The quality and comprehensiveness of National guideline for major NCDs of Ethiopia were evaluated based on clinical guideline appraisal tool [19-22] and comprehensiveness evaluation tool developed by the research team.
Only 12 (50%) of ADAPTE process steps were addressed in National adult hypertension treatment guideline of Ethiopia [27]. The guidelines used for adaptation were not clearly mentioned, there quality is not assessed by validated instruments Like AGREE [59]. Generally, the guideline lacks engagement of all relevant stakeholders. Involving end-users is important to; address questions relevant to consumers, prioritize focus areas and improve acceptance [25].
Ethiopian national adult hypertension treatment guideline metonly 22 (64.7%) of guideline quality standards [27]. Major problems of the guideline include; lack ofevidences evaluation to contextualization, incomplete adaptation of evidences and poor involvement of relevant stakeholders including end-users. This might be reason for poor dissemination of the guideline as evidenced by only 9% of health facilities have guidelines for CVD prevention and control [9].
Similarly, the guideline was the least comprehensive 15 (51.7%) [27]. Major content problem werelack of diagnostic approach for masked, white-coat and resistant hypertension. The guideline did not address the genetic predisposition, child hood risk factors and secondary cases of hypertension. Similarly,management of hypertension in patients undergoing surgery, specific patient groups, Access to medicine and social determinants of health are not included in the guideline [27].
Regarding Blood pressure targets, ACC/AHA and HEART's target BP < 130/80 mmHg for high risk and BP < 140/90 mmHg for others. Australian and Canadian guidelines targets BP < 120/80 for high risk, BP < 140/90 mmHg for others. European hypertension society guideline targets BP < 140/90 mmHg in all patients and if treatment is tolerable < 130/80 mmHg, 120-129/< 80 mmHg for patients less than 65 years old and 130-139/< 80 mmHg in ≥ 65 years [1,12,14-18,34]. Blood Pressure goal all these guidelines is based on SPRINT trial [60] and meta-analysis of 19 global blood pressure trials [61].
Ethiopian guideline for major NCDs targets BP < 140/90 mmHg for adults 18-75 years and BP < 150/90 mmHg for patients above 75 years of age [27]. However, mortality from NCDs in developing countries including Ethiopia is Premature (i.e. below 70 years) [9]. Therefore targeting population above 75 years in country where life expectancy is 65 years requires reconsideration of this recommendation and it is not supported by evidence.
HEART's technical package [15] and major NCDs guideline of Ethiopia [27] have similar BP targets. This is in line with the recent Cochrane review evidence which indicated no change in mortality or no differences in serious adverse events intargeting blood pressure targets (≤ 135/85 mmHg) when compared with 'standard' blood pressure targets (≤ 140 to 160/90 to 100 mmHg). There is insufficient evidence to justify lower blood pressure targets (≤ 135/85 mmHg) in people with hypertension and established CVD [62].
Race and ethnicity are becoming important for hypertension treatment and control. This is because of genetic variation and differences in social determinants of health. For example, Hypertension in black patients as compared with white patients tends to be more common, to present earlier in life, to be more severe and rapidly progressive [63]. Black patients are at significantly greater risk for stroke than white patients, especially at younger ages, due in part to the earlier onset and greater severity of hypertension. The adjusted relative risk of stroke, for example, is more than twice as high in hypertensive black patients aged 45-64 years as compared with similarly aged hypertensive white patients [64].
The Important risk factors for hypertension among black patients include: Lower socioeconomic status, Ingestion of a high-sodium/low-potassium diet, is poor maternal nutrition leading to low birth weight in the infant [65]. Use of CCBs and thiazides as first line therapy over ACEIs for uncomplicated hypertension in blacks is recommended [1]. This may be associated with the maternal nutritional problems and low birth weight which could contribute development of few functional nephrons [65].
A Patient follow-up, monitoring BP targets and dose intensification of drugs or introduction of combination modalities are important for controlling blood pressure. The HEARTs technical Package [15] clearly described the duration of BP monitoring and dose intensification or addition of another drug if BP is not controlled. Ethiopian NCD guideline states starting at low doses and increasing dose step by step to maximum tolerated dose. But it did not describe when and how to intensify drug therapy [27]. This could contribute to under treatment of patients that could have benefited from appropriate intensification of drug therapy.
Access to medicines and basic technologies for hypertension prevention and control was not addressed in Ethiopian NCD guideline [27]. About 80% of deaths due to chronic illnesses in low and middle income countries (LMICs) are due to poor access to basic services in primary health care; lack of affordable laboratory tests and medicines and poor adherence to treatment [10,66,67]. According to the third national pharmaceutical sector survey percentage availability of medicines used for chronic illnesswas 54.55% which is below WHO target (i.e. 80%). In addition this none of essential medicines for NCDs were affordable [52].
Healthcare service delivery system availability and Readiness survey indicated that thegeneral service readiness index was 54%. Concerning readiness and availability of CVD care, the availability of diagnosis and/or management of CVD service was 41%. Only 9% of facilities had Guidelines for CVD diagnosis and management [9,55]. Improving health system capacity to provide comprehensive CVD care is important.
Health Literacy is not well addressed as component of care in National NCD guideline of Ethiopia.Enhancing the health literacy of individuals and communities is an important measure to improve acceptability of NCD interventions [12,68]. Different studies indicated association between low literacy, with uncontrolled BP, low medication adherence [69,70].
Another important but ignored component of care in Ethiopian guideline was social determinants of health.Findings from different literatures indicated that clinical care contributes only 10-20% to health outcomes of a person even in their best possible stand. Socioeconomic factors, health behavior and factors related to the physical environment are estimated to account for up to 80% of health outcomes [37]. Therefore creating local social support system for economically disadvantage groups may give opportunity to achieve treatment goals.
In conclusion, quality and comprehensiveness of Hypertension treatment guideline of Ethiopia is suboptimal. Major quality problems include lack of literature evaluation for contextualizationof evidences and lack of consideration to specific patient populations. Major comprehensiveness problemswerelack of diagnostic approach for masked, white-coat and resistant hypertension. Similarly, Access to medicine and social determinants of health are not addressed in the guideline.
Therefore, we recommend the guideline development committee and other relevant stakeholders to: update the blood pressure targets and age classification of elderly population, determine when to initiateand intensify antihypertensive drug therapy; address social determinants and socioeconomic status of population including maternal nutrition and Access of medicines. It is also important to enhance dissemination of guideline to all health facilities to provide standardized care to all patients with hypertension.
Not applicable.
Not applicable.
Not Applicable. This is systematic review and we have used only published articles.
The authors declare that they have no competing interests.
There is no funding source for the study.
All Authors read and approved the manuscript. MM: has framed the format design conducted the review and developed the manuscript for publication; MD: has conceived the review project; AA: participated in literature review and format design, participated in literature review and polished the language of the manuscript.
We would like to thank all Tehran University medical sciences, department of pharmacoeconomics and Pharmaceutical Administration staffs for their technical and material support during our review including access to Internet.