Takotsubo Syndrome usually presents with normal coronary arteries and the typical pattern of apical ballooning on the left ventricle. This entity can recur but very infrequently it presents with a different pattern of left ventricle wall motion abnormality. We describe the case of a 58-year-old woman presenting with recurrent TTS, associated with two different wall motion patterns in a period of nine years, triggered by a similar stressor factor.
Cardiomyopathy, Acute coronary syndrome, Tako-Tsubo
Takotsubo Syndrome (TTS), also known asStress-induced Cardiomyopathy, is a transient left ventricle (LV) regional dysfunction without significant coronary obstruction or plaque rupture [1].
According to the modified Mayo Criteria, the diagnosis requires the presence of all four of the following: a) Transient hypokinesis, dyskinesis, or akinesis of the LV midsegments, with or without apical involvement; with wall-motion abnormalities that extend beyond a single epicardial vascular distribution; b) Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture; c) Signs of ischemia withnew ECG abnormalities (either ST-segment elevation and/or T-wave inversion) or modest elevation in the cardiac troponin level; d) Absence of pheochromocytoma or myocarditis.
Clinically, four major anatomic patterns of regional wall motion abnormality have been recognized: Apical ballooning is the more frequent presentation that is present in approximately 81% of cases. Other variants have been described such as mid-ventricular (14%), basal or inverted (2%) and focal (1%).
Recurrence of this entity is uncommon, and most cases present with similar wall motion abnormalities on relapse [2,3].
We present the case of a 58-year-old patient that presents with TTS with two different ballooning patterns in two separated events.
A 58-year-old woman with hypercholesterolemia, hyperuricemia and insulin resistance presented in the emergency room (ER) with 90 minutes of intense retrosternal chest pain, radiating to jaw and profuse sweating after a very stressful family event. She was hemodynamically stable without signs of heart failure on physical examination. ECG showed T wave inversion in V5 and V6 leads without changes on serial ECGs. Troponin T was 211 ng/L (normal value < 14 ng/L). Coronary angiography proved absence of significant stenosis, and ventriculography showed mid-ventricular hypokinesia with preserved ejection fraction (Figure 1). There was complete resolution of the wall motion abnormalities on follow up echocardiogramafter 21 days. TTS was diagnosed.
 Figure 1: A) Coronary Angiogram demonstrating absence of obstructive disease in the LAD; B) Diastolic and; C) Systolic phases of the ventriculogram showing mid cavitary hypokinesis. View Figure 1
Figure 1: A) Coronary Angiogram demonstrating absence of obstructive disease in the LAD; B) Diastolic and; C) Systolic phases of the ventriculogram showing mid cavitary hypokinesis. View Figure 1
Nine years later, after a stressful personal event, she presented again in the ER with 2 hours of chest pain. ECG showed no changes compared to her previous admission. Troponin T was 314 ng/L. Coronary angiography and optical coherence tomography (OCT) demonstrated nonobstructive coronary artery disease without signs of plaque rupture or erosion (Figure 2). Ventriculography showed apical akinesia and hypercontractility of the remaining segments, suggestive of classic apical TTS (Figure 2). Plasma metanephrine levels were normal. Cardiac magnetic resonance (CMR) was compatible with TTS. The patient was discharged with enalapril and bisoprolol. Echocardiographic follow up 21 days later revealed normal LV wall motion and preserved ejection fraction. To date the patient remains asymptomatic.
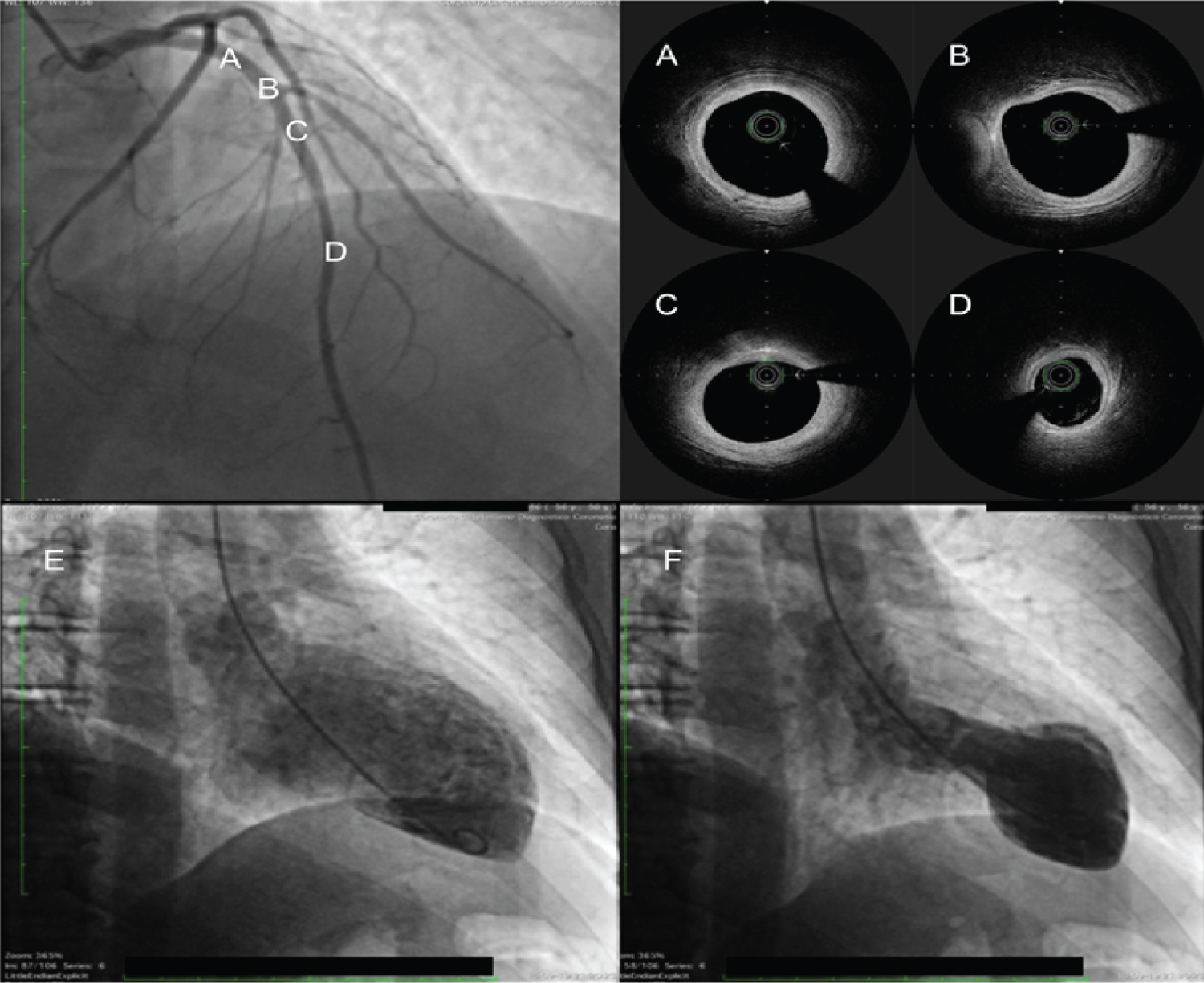 Figure 2: A-D) Coronary Angiogram demonstrating absence of obstructive disease in the LAD with OFDI of the corresponding segments of the vessel without signs of plaque rupture or erosion; E) Diastolic and; F) Systolic phase of the left ventriculogram with classical apical ballooning. View Figure 2
Figure 2: A-D) Coronary Angiogram demonstrating absence of obstructive disease in the LAD with OFDI of the corresponding segments of the vessel without signs of plaque rupture or erosion; E) Diastolic and; F) Systolic phase of the left ventriculogram with classical apical ballooning. View Figure 2
Takotsubo syndrome, was first described in Japan almost 30 years ago and was named after the similarity with an octopus trap, which has the shape comparable to the systolic apical ballooning appearance of the left ventricle characteristic in the classical variant [4]. The exact etiology is not known. A significant emotional or physical stressor factor typically precedes the development of TTS. Theories aim to overstimulation of hypothalamus pituitary adrenal axis that results in excessive release of catecholamines.Acute onset of TTS and its association with pheochromocytoma or paraganglioma have also supported this theory.
Catecholamine excess leads to subtle metabolic changes at cellular level. B2-adrenoreceptor mediated GS proteins signaling is converted to G1 protein signaling leading to reduced myocardial contractility and LV dysfunction [4].
Clinically, apical ballooning is present in approximately 80% of the cases but also mid-ventricular (16%), basal, and focal wall motion abnormalities can be found. Higher concentration and sensitivity of adrenergic receptors in the apex may explain the segmentary disfunction seen in the classic pattern but not the other variants [5].
The diagnosis should be based on Modified Mayo clinic criteria, an invasive coronary study must be performed to rule out coronary arterial obstructive disease. In this group of patients, there is a high prevalence of coronary artery disease. The use of intracoronary imaging can be helpful in ruling out the presence of plaque rupture and erosion that can be not evident on angiography. In an experience by Eitel, et al., where routine OCT of the left anterior descendant artery was performed in TTS patients, almost 70% of patients had stable atherosclerotic plaque in this territory without images of plaque rupture or erosion [6].
Cardiac magnetic resonance (CMR) can also be useful in the diagnosis of TTS. Data show that the etiopathogenic mechanism is not an ischemic or a fibrosis one, since late gadolinium enhancement is almost never found, but the presence of high signal intensity areas in the T2-weighted sequences reveals frequent myocardial oedema. It seems that a search for such an oedema should be systematically performed in patients with suspected TTS [7].
Recurrent TTS is infrequent with reported relapse rates of 0.6 to 6%. Most of the patients relapse with similar patterns. Recurrent TTS with different patterns is a very uncommon situation that has been described in scarce case reports [7].
TTS diagnosis is a challenging situation, specially in the presence of atypical clinical variants. The diagnosis should be based on Modified Mayo clinic criteria. Primary TTS commonly affects postmenopausal elderly women. Echocardiography, coronary angiography and cardiac MRI are useful tools in the diagnosis of TTS. Prognosis of TTS is generally good in over 90% patients.
Infrequently, patients can have recurrences with different variants pattern as we shown in this case and the physicians must be familiar with this situation.
The authors have no conflicts of interest to disclose.