IgD multiple myeloma (MM) is a rare plasma cell neoplasm, considered to have a poor prognosis compared to the other isotypes. Many studies reported an advanced stage at the presentation. In contrast to these studies, we report a case of rare IgD-Lambda MM at the early stage. The laboratory data showed no hypercalcemia, without any renal impairment, or monoclonal spike (M-spike or paraprotein) at the Serum protein electrophoresis (SEP) but only a hypogammaglobulinemia. IF is performed with antisera to IgG, IgA, IgM, total kappa and total lambda (anti-γ, anti-α and anti-μ heavy chains, and anti-κ and anti-λ total light chains) showed a lambda total light chains without corresponding heavy chain. The first IF of the most frequent isotypes was completed with the second serum IF for the screening of the rare isotypes, with anti-sera to IgD, IgE (anti-δ and anti-ξ) and to total kappa and total lambdaheavy chains showed an IgG-Lambda isotype with no free light chains. Hypogammaglobulinemia was associated to more than 80% of IgD MM. So, hypogammaglobulinemia can be used as an indicator of IgD MM isotype. Finally, bone pain, anemia and renal failure are the most frequent inaugural symptoms.
IgD, Multiple myeloma, M-spike, Back pain
Multiple myeloma (MM) is characterized by the clonal proliferation of malignant plasma cells, which secrete monoclonal immunoglobulin in the bone marrow. Immunoglobulin D(IgD) MM is a rare subtype associated with poorer prognosis, and accounting for about 2% of MM cases worldwide [1,2]. Moreover, IgD MM is often misdiagnosed because of the small amount of the monoclonal protein, or mistaken as light chain type MM. It is characterized by the high preponderance of lambda light chains over kappa light chains [3].
Patients with IgD myeloma presented more often with features of high-risk disease, that is, with advanced ISS (International staging system), high LDH (lactate dehydrogenase), significant renal dysfunction, and large amounts of Bence jones proteinuria [1,3]. Response to primary therapy was similar to other patients, although there was a trend for better quality of responses in patients with IgD myeloma [3].
First of all, we report a challenging case in the diagnosing of a rare immunoglobulin D-Lambda (IgD) MM, that is often of advanced stage at the diagnosis. Nevertheless, our patient was at an early stage, with no hypercalcemia, normal kidney function, Serum protein electrophoresis (SPE) with no M-spike (Monoclonal protein-spike) and normal urinary proteinuria excretion. In addition, we want to emphasize that not all the CRAB (hypercalcemia, renal failure, anemia and bone disease) criteria are needed for a diagnostic of multiple myeloma, and SPE is not a specific test for the diagnosis of IgD MM.
A 57-year-old man from Souss-Massa region, in Morocco. The patient is a worker in a factory; he has no family history of malignancy or blood disorders. Our patient's medical history includes an operation for an inguinal hernia two years ago, followed by an appendectomy in 1990; also, he had glaucoma of the left eye under treatment since 2015.
He experienced a back pain, and a weight loss with an average of 20 kg in two months and a fast worsening of the general state. His conjunctivae are discolored. Skeletal X-ray examination detected osteolytic lesions in the skull (Figure 1).
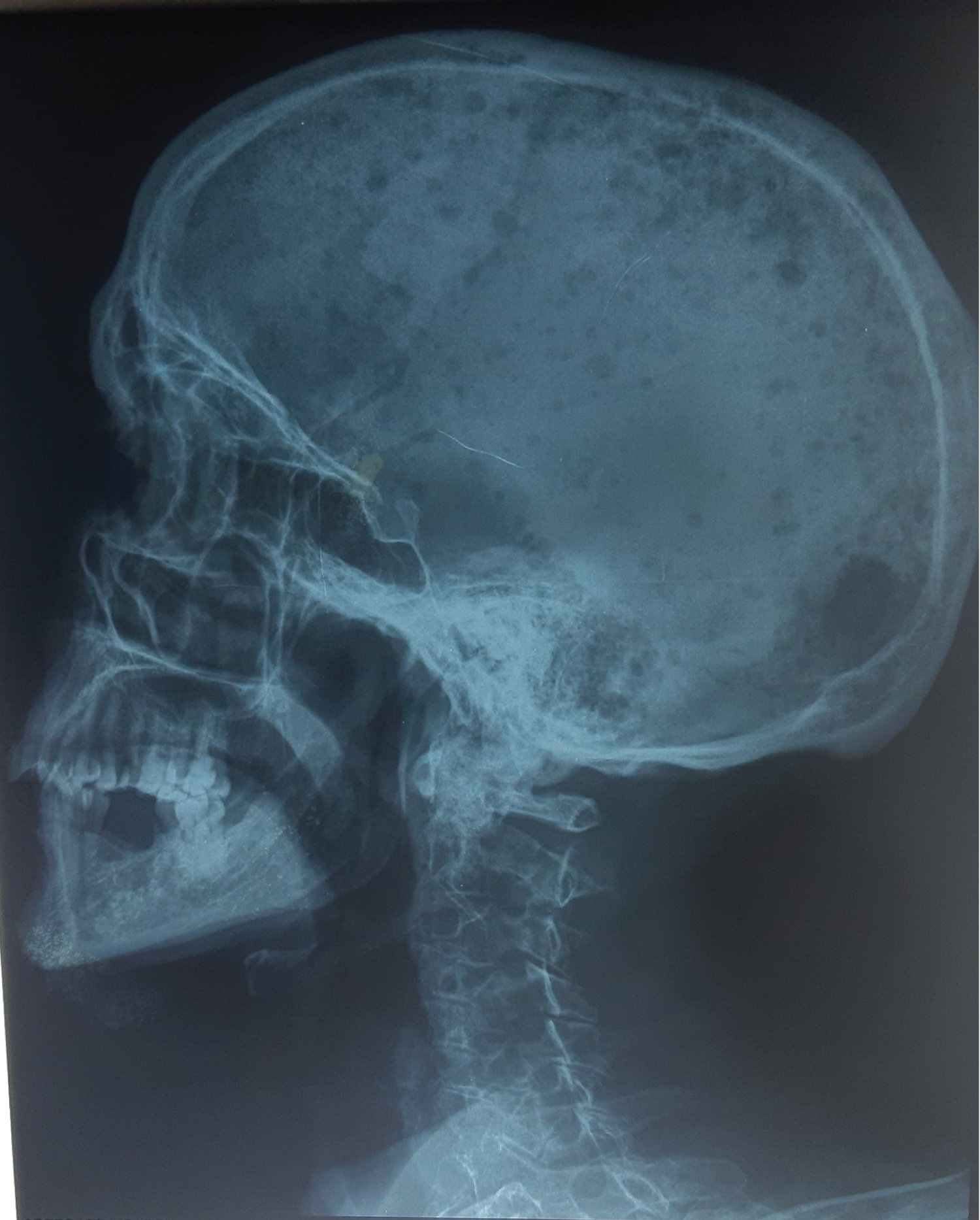 Figure 1: Skull X-Ray. View Figure 1
Figure 1: Skull X-Ray. View Figure 1
In contrast, laboratory data showed no hypercalcemia, without any renal impairment, or M-spike at the Serum protein electrophoresis SPE). Subsequent laboratory studies showed a β2-microglobulin of 2.88 mg/l (0.7-1.8 mg/l), total protein of 54 g/l (64-83 g/l), Albumin of 32.9 g/l (40-50 g/l), calcium 2.1 mmol/L (2.2 to 2.7 mmol/L), AST of 5 UI/L (0-40 U/L), ALT of 16 U/L (15-40 U/L), blood glucose of 4.73 mmol/l (4.4-6.1 mmol/l), urea of 3.7 mmol/l (2.5-10.7 mmol/l), creatinine of 82 μmol/l (62-106 μmol/l), GFR of 91 ml/min/1.73 m2, erythrocyte sedimentation rate (ESR) of 43 mm/h (< 30 mm/h), urinary protein of 0.06 g/24 h (< 0.15 g/24 h) and lactate dehydrogenase of 364 U/l (125-220 UI/l) (Table 1). Complete blood counts were measured during all the course of the treatment, on admission the patient presented with a normocytic normochromic anemia of 73 g/l (hemoglobin < 120 g/l) and a leukopenia, the platelet count was normal. Bone marrow aspiration revealed 55% dystrophic plasma cell infiltration with several abnormal plasma cells, and immature plasma cells (plasma blasts) (Table 1). Serum protein electrophoresis revealed a mild hypogammaglobulinemia and no M-spike (Capillarys 2-Sebia®) (Figure 2). Therefore, immunofixation (IF) is the gold standard method to confirm the presence of a monoclonal protein. IF is performed with antisera to IgG, IgA, IgM, total kappa and total lambda (anti-γ, anti-α and anti-μ heavy chains, and anti-κ and anti-λ total light chains) showed a lambda total light chains without corresponding heavy chain. Also, Urine immunofixation was negative for a monoclonal protein. An additional IF is performed, for the screening of the rare isotypes, with anti-sera to IgD, IgE (anti-δ and anti-ξ) heavy chains, and total kappa, total lambda, free kappa and free lambda light chains showed an IgG-Lambda isotype with no free light chains.
 Figure 2: Serum protein electrophoresis. View Figure 2
Figure 2: Serum protein electrophoresis. View Figure 2
Table 1: Bone marrow aspirate differential count. View Table 1
Our patient has had a normal kidney function; therefore, he was classified at the stage II of the revised international staging system (RISS).
Criteria for the diagnosis of multiple myeloma were fulfilled, and the patient was treated with a combination of cyclophosphamide, monthly pulsed dexamethasone, low-dose Thalidomide (CDT) and zoledronic acid. He underwent autologous hematopoietic stem cell transplant and was subsequently started on lenalidomide maintenance.
Firstly, IgD MM is rare. In fact, in a cohort of the Mayo Clinic in Rochester, recording all the patients whom multiple myeloma was diagnosed from 1985 to 1998, only 2% of all the record were with an Ig D MM, and the most frequent isotypes were Ig G, IgA and Free light chain with 52%, 21% and 16% respectively [1]. Also, Zagouri, et al. in a retrospective study among 1239 patients with symptomatic myeloma, only 2.5% were diagnosed with IgD MM [3]. We found the same results in a retrospective study (not yet published), through ten years, in our oncology department of Agadir regional hospital, we diagnosed only, two patients with IgD-lambda MM of 117 patients with monoclonal gammopathies, so, 1.7% of all the monoclonal gammopathies and 2.2% of patients diagnosed with MM.
Gender is one of the risks factors associated with MM in general, in fact, all cohort studies have noticed a male predominance of IgD MM [4,5]. Also, in our retrospective study, two male cases were indeed collected. Moreover, the most significant risk factor is age; our patient has 57-year-old, even though the two thirds of patients with MM in general are older than 65 years [6]. For the patients with IgD MM, and in the study of Bladé, et al. [4], the median age of the 53 patients with IgD MM, was 60 years (Range, 19 to 86), also Jancelewics, et al. [5], reported a median of 59 years and in the study of Shimamoto, et al. [7], the median age of 55.7 years. Thus, Ig D myeloma is diagnosed at an early age compared to other MM isotypes.
ESR was not so elevated, as one of the classic presentations of MM, because of the low concentration of the monoclonal immunoglobulin.
The inaugurals symptoms in our case were the back pain and weight loss, in fact, several international studies found that the main clinical symptom is represented by bone pain in more than 72% of patients [5,8]. Our patient has a normal kidney function with no proteinuria. Nevertheless, according to literature, the second most important inaugural clinical manifestation in patients with IgD MM, was the renal impairment, more than one third of the patients [9]. Moreover, the third most important symptom in this case was the normocytic normochromic anemia, the frequency of normocytic normochromic anemia exceeds 70% in most international series and can even reach 90% others [5,10]. SEP revealed hypogammaglobulinemia with no monoclonal spike. Interestingly, Serum protein electrophoresis was associated with hypogammaglobulinemia in 84% in the cohort of Bladé, et al. 100% in the cohort of Djidjik, et al. [10]. So, hypogammaglobulinemia can be used as an indicator of IgD MM. Serum immunofixation electrophoresis (SIE) revealed IgD-lambda MM, furthermore IgD-lambda was the most diagnosed isotype in all reported studies. In fact, 60% in the cohort of Bladé, et al. 80% in the cohort of Zagouri, et al. [3] and 90% in the cohort of Jancelewicz, et al. [5]. Thus, most frequent IgD myelomas are of the lambda variety.
In IgD MM, the whole skeleton (Spine, Skull, pelvis, ribs...) can be affected by multiple lyric lesions at the diagnosis. Shimamoto, et al. found osteolytic lesions in 42% of patients in their cohort [7], 77% in the cohort of Bladé, et al. and 80% in the cohort of Djidjik, et al. [10].
At last, IgD MM is rare subtype of MM and affect people with the median age of 60-year-old. SEP didn't show any M-spike in this case, but a hypogammaglobulinemia. Therefore, Hypogammaglobulinemia can be an indicator of the IgD MM. Also, the most frequent isotype is the IgD lambda. Another point is that, bone pain, anemia and renal failure are the most frequent inaugural symptoms. Finally, lytic lesions at the skeleton radiography are frequent in IgD MM.