Thromboembolic events contribute to the most serious outcomes in patients with nephrotic syndrome. We report a case of a young male patient with mesangial proliferative glomerulonephritis presenting with nephrotic syndrome, which rapidly progressed to mesenteric and portal veins thrombosis and septic shock, ultimately leading to death.
Mesangial proliferative glomerulonephritis, Nephrotic syndrome, Mesenteric and portal veins thrombosis, Septic shock
A 19-years-old, male patient was admitted due to bilateral lower extremity edema and abdominal distension. The abdominal distension appeared 2 months ago with accompanying bilateral lower extremity edema. In a local hospital, laboratory data showed: Serum albumin 15.4 g/L and 24 hr. urine protein 6.683 mg. The patient was diagnosed with nephrotic syndrome and renal biopsy revealed mesangial proliferative glomerulonephritis. The symptoms recovered after the patient received prednisone 60 mg/day for 12 days and steroid therapy was continued. 3 weeks ago, the patient suddenly felt nausea, vomiting and had watery stool. There was a relapse of bilateral lower extremity edema together with worsening of the abdominal distension. Paracentesis was performed in another local hospital which revealed hemorrhagic ascitic fluid and treatment with prednisone was stopped. Finally, the patient was admitted in our hospital with abdominal distension and bilateral lower extremity edema as chief complaints. The latter did not have any history of hepatitis B and without arthralgia, erythema or papules in the lower extremity. The past medical history and family history were not relevant.
Physical examination findings on admission: Temperature 37 °C, heart rate 88 beats/min, respiratory rate 22 breaths/min and blood pressure 110/70 mmHg. The patient looked emaciated and malnourished. On auscultation of the lungs, the breath sounds were coarse but without rales. There was rigidity of the abdominal muscles, tenderness in the epigastric region and left hypochondrium, lumbar and iliac regions. Blumberg's sign was positive. Shifting dullness was positive. The bowel sound was decreased and there was bilateral pitting edema at the ankles.
Routine blood test: WBC 20.00 × 109/L, RBC 4.02 × 1012/L, Hb 122.0 g/L, PLT 674 × 109/L and neutrophils 94.1%. Urinalysis: Proteinuria 2+ and Hematuria 2+. Renal function test: BUN 8.40 mmol/L and SCr 66 umol/L. Liver function test: Total protein 31 g/L and albumin 7 g/L. Electrolytes: K+ 4.44 mmol/L, Na+ 124 mmol/L and Cl- 93.5 mmol/L. Arterial blood gas analysis: pH 7.440, PaO2 111.0 mmHg, PaCO2 29.0 mmHg, HCO3 22.90 mmol/L, SPO2 99% and BE (ecf) -4.50 mmol/L. Immunologic panel: ANA and anti-dsDNA were negative. HBsAg was negative. Paracentesis was performed and showed a turbid ascitic fluid, with WBC > 50/HP and RBC 20-30/HP and culture revealed the presence of Gram-negative bacilli and Gram-positive cocci. Biochemistry of the ascitic fluid showed: Total protein 4 g/L, Albumin 1 g/L, LDH 303 U/L and ADA 17.7 U/L.
The patient was diagnosed with primary nephrotic syndrome, hyponatremia and acute peritonitis. After admission in our hospital, the patient received oxygen by mask. Levofloxacin, cefepime and metronidazole were at once given to prevent the spread of infection. Diuretics and other symptomatic treatment were given but the patient still had pain in the epigastric region, with sweating, low vitality and serious edema. The results of the coagulation profile showed: PT 67.1s, INR 5.79, APTT 90.8s, FBG 4.85 g/L and D-dimer 213.0 ul/L. Abdominal CTV was performed and showed thrombosis in the superior and inferior mesenteric veins (MVT) and portal vein (PVT) (Figure 1). Treatment with low molecular weight heparin was immediately started. 45 hrs after admission, the patient suffered from dyspnea and had a respiratory rate of 65 breaths/min and heart rate of 132 beats/min and the blood pressure was 65/30 mmHg. Dopamine and voluven were given to the patient and the blood pressure raised to 100/60 mmHg. The patient had to be transferred to the ICU for intubation but refused due to financial limitation. 3 hrs later, the patient felt irritated with blurred consciousness and had tremor of the head and both upper and lower limbs with a blood pressure of 110/65 mmHg, heart rate of 135 beats/min and respiratory rate of 40 breaths/min with shallow and rapid breathing. Ultimately, the patient died 2 days after admission in our hospital.
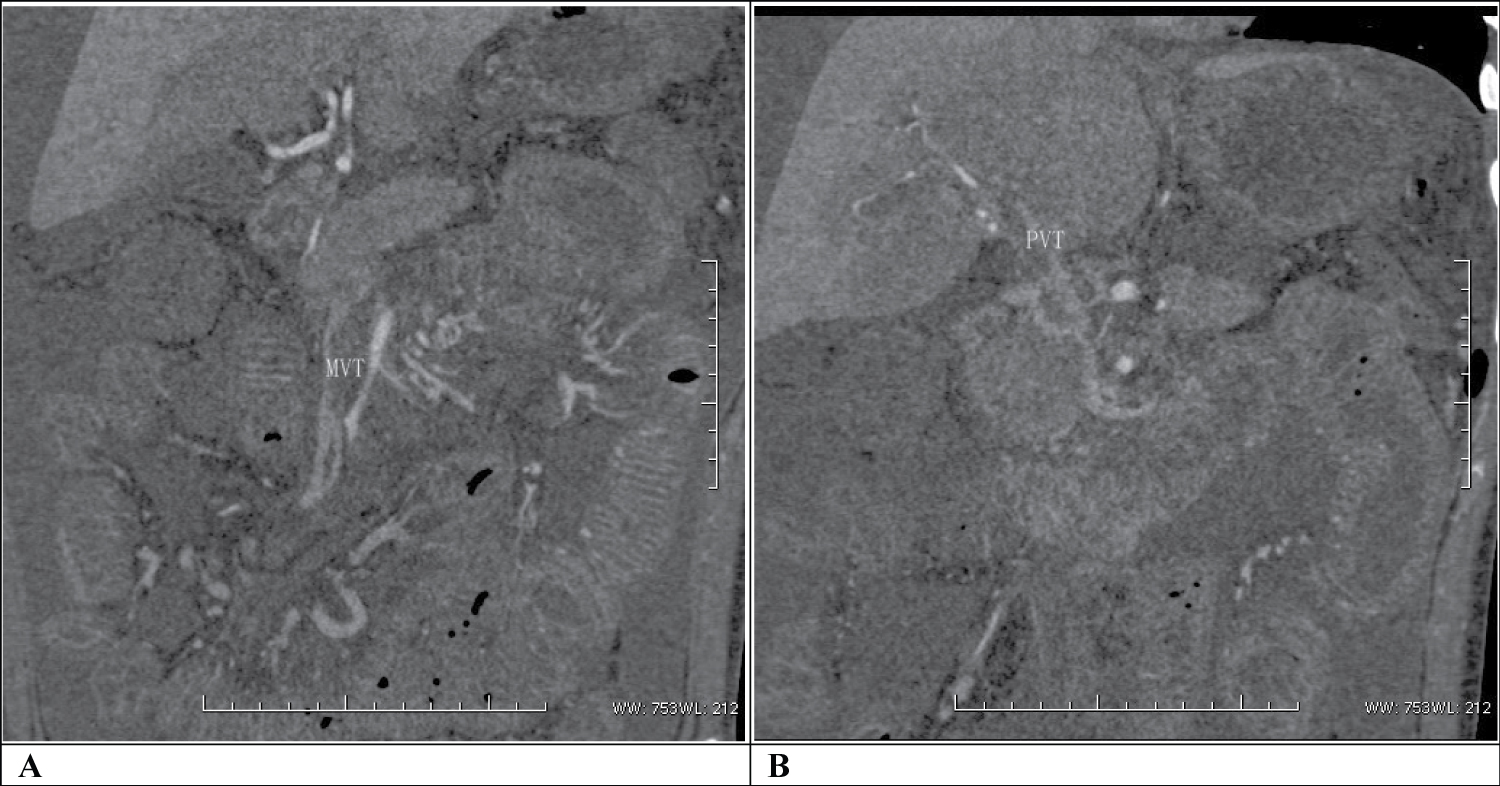 Figure 1: Thrombosis in (a) The superior and inferior mesenteric veins (MVT) and; (b) Portal vein (PVT) in the patient with mesangial proliferative glomerulonephritis. As shown by CTV, there was obvious occlusion in the superior and inferior mesenteric veins and portal vein.
View Figure 1
Figure 1: Thrombosis in (a) The superior and inferior mesenteric veins (MVT) and; (b) Portal vein (PVT) in the patient with mesangial proliferative glomerulonephritis. As shown by CTV, there was obvious occlusion in the superior and inferior mesenteric veins and portal vein.
View Figure 1
Nephrotic syndrome is always complicated with acute kidney injury, infection and thrombosis and a serious complication may affect the prognosis of the patient [1]. In this case, the patient was initially diagnosed with primary nephrotic syndrome because of edema, hypoalbuminemia and proteinuria; with exclusion of systemic lupus erythematosus, HBV-associated nephritis and papular nephritis, and the histopathological change was mesangial proliferative glomerulonephritis. Even the edema was temporarily relieved after treatment with prednisone but unfortunately, the patient died of a sudden onset of complications; that is thrombosis (MVT and PVT), secondary peritonitis, septic shock and acute respiratory distress syndrome (ARDS).
Thrombosis is a common complication of the nephrotic syndrome. Several factors are responsible for the development of thromboembolic events including a hypercoagulable state and steroid therapy. However, the most common thrombosis in the nephrotic syndrome is that of the renal vein and deep veins of the lower extremity; the prevalence of renal vein thrombosis being highest in patients with membranous glomerulonephritis at 37% followed by membranoproliferative glomerulonephritis at 26.2% and minimal change disease at 24.1% [2]. MVT alone or concomitant with PVT, on the other hand, is rare [3-7]. The cases that have been reported so far include only patients with minimal change disease as primary cause for the nephrotic syndrome [3-7]. To our knowledge, this is the first case reported of MVT and PVT with septic shock and ARDS in a patient with mesangial proliferative glomerulonephritis.
MVT is a rare acute abdominal disease. A diagnosis for MVT with PVT is usually delayed because of its nonspecific presentations [7]. The early clinical findings in MVT are epigastric pain, nausea and vomiting. In advanced cases of MVT, there is hemorrhagic ascitic fluid due to infarct of the intestines leading to peritonitis. Hence, mortality is very high among these cases. The clinical findings in PVT are abdominal pain or distension with large ascites [8,9]. In this patient with nephrotic syndrome, a sudden onset of the aforementioned symptoms, especially the presence of hemorrhagic ascitic fluid, should raise a high suspicion of MVT and not just a relapse of the nephrotic syndrome. D-dimer evaluation and abdominal CTV should then be considered to immediately confirm the diagnosis of MVT and PVT.
Treatment and prevention of thrombosis in the nephrotic syndrome are essential and consist of the use of anticoagulants such as low molecular weight heparin and coumarins. Urokinase is the most commonly used thrombolytic agent for venous thrombosis. Advanced cases of MVT with infarct of the intestines require excision; this may be an effective treatment to prevent secondary infection, sepsis and shock and thus improve prognosis [10].
Although MVT concomitant with PVT has a relatively low incidence in patients with nephrotic syndrome, an early suspicion and timely management are crucial to prevent septic shock and decrease mortality.