A 24-year-old male with no clinical history, presents with jaundice. There was no abdominal pain.
Ultra sound shows a huge right sided, well bordered, globally hyperechoic retroperitoneum, solid mass, with calcifications (Figure 1), in the peri renal space. CT scan (Figure 2) shows an encapsulated soft tissue mass, with net border, anterior to the right kidney, responsible of mass effect on the right liver and inferior veina cava, with heterogeneous density associating multiple fatty containing zones, an enhanced solid component and calcifications. This lesion measures approximately 20 × 13 cm in longitudinal and anterior-posterior dimensions. No aggressive features were noted especially the absence of extension to the adjacent organs.
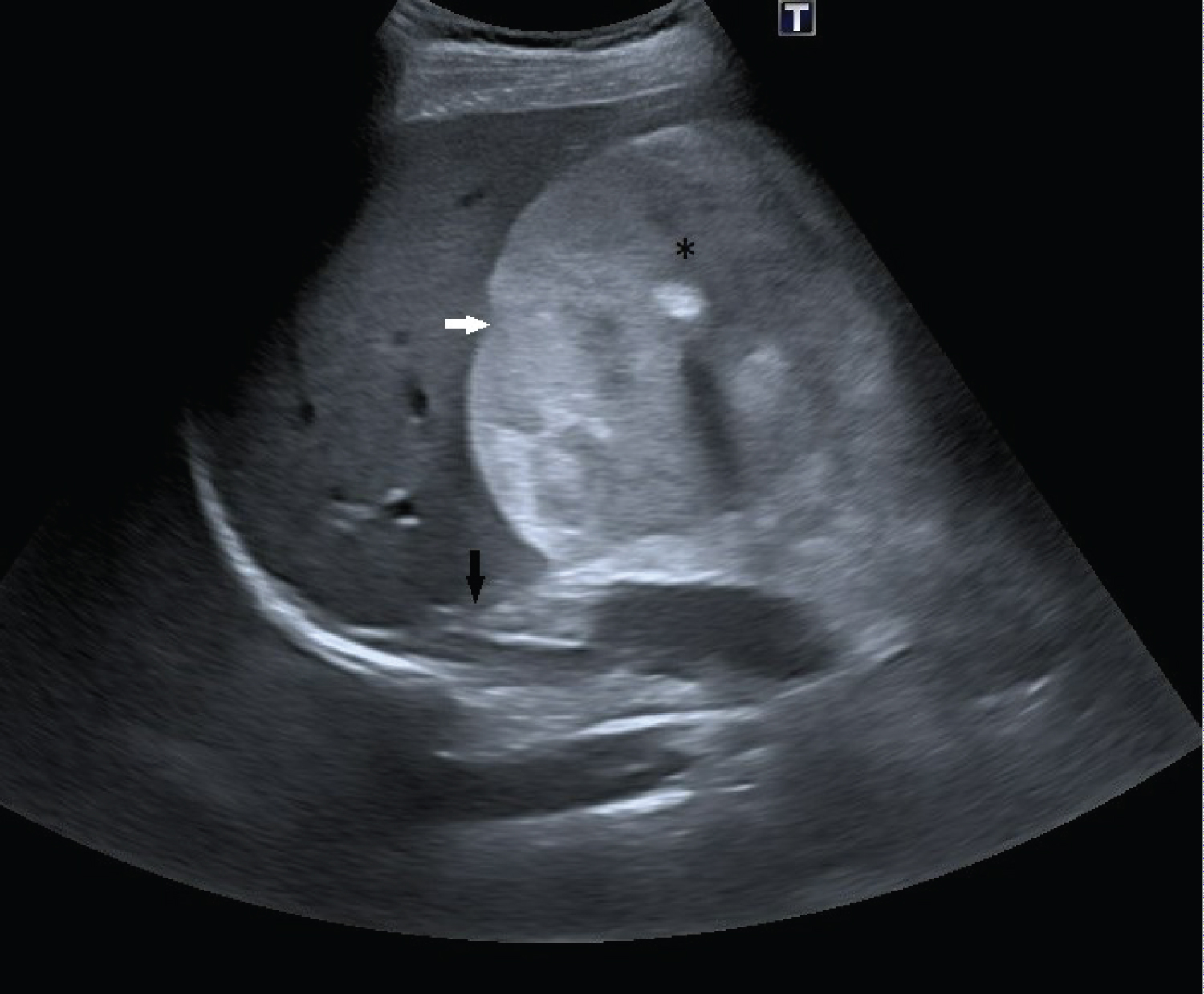 Figure 1: Sagittal sonography imaging, shows a globally hyper echoic well bordered retroperitoneum mass, with calcification (asterisk). Not the mass effect on the liver (white arrow) and the right kidney (black arrow).
View Figure 1
Figure 1: Sagittal sonography imaging, shows a globally hyper echoic well bordered retroperitoneum mass, with calcification (asterisk). Not the mass effect on the liver (white arrow) and the right kidney (black arrow).
View Figure 1
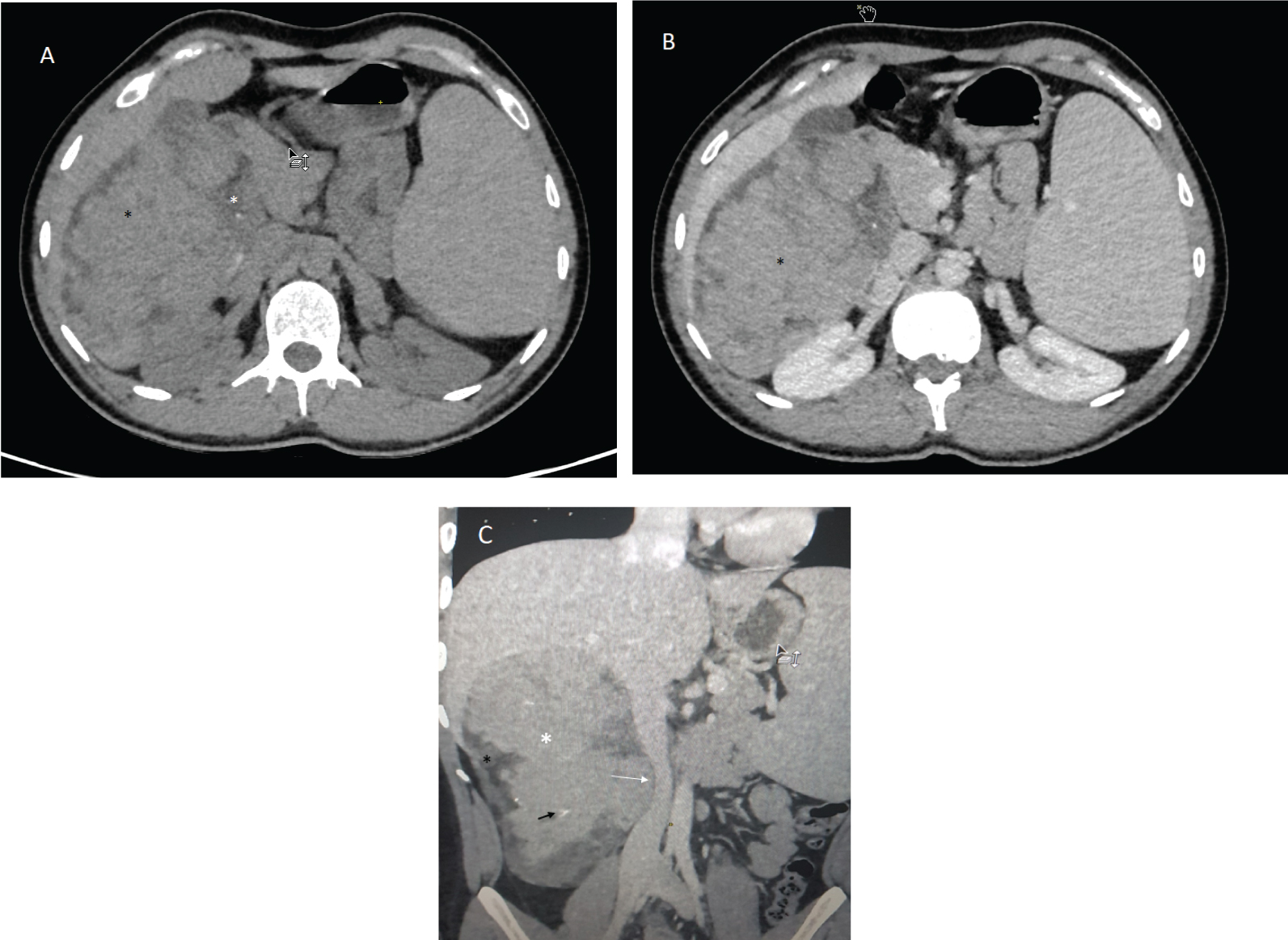 Figure 2: Axial CT scan before (a) and after (b) IV administration of contrast, contrast enhanced coronal CT (c): Right sided, retro peritoneum, extra renal and extra adrenal, encapsulated, solid mass with predominant enhancing soft tissue component (black asterisk), peripheral fatty (white asterisk) containing areas, macro calcification (black arrow). Note the mass effect on the inferior veina cava (white arrow).
View Figure 2
Figure 2: Axial CT scan before (a) and after (b) IV administration of contrast, contrast enhanced coronal CT (c): Right sided, retro peritoneum, extra renal and extra adrenal, encapsulated, solid mass with predominant enhancing soft tissue component (black asterisk), peripheral fatty (white asterisk) containing areas, macro calcification (black arrow). Note the mass effect on the inferior veina cava (white arrow).
View Figure 2
Extra-adrenal myelolipomas are a group of mesenchymal tumors which consist of a mixture of mature adipose tissue with hematopoietic cells. This intriguing tumor most commonly occurs within the adrenal gland; however, it has been occasionally found within the pelvis, thorax, retroperitoneal space, and various other sites throughout the body [1,2]. The physiopathology is not yet clearly explained, Amin, et al. [3] suggest that there may be a relationship between the re-activation of primitive peritoneal foci of extramedullary hematopoiesis under pathological stresses (severe anemia, sepsis, myeloproliferative disease ...) and the origin and progression of extra-adrenal myelolipomas.
A review of the literature shows that extra-adrenal myelolipomas exhibit a slight female predominance and are typically discovered incidentally between the ages of 50 and 70-years-old [4,5]. The limb did not cause abdominal pain but only a jaundice.
The well-defined fatty masses in myelolipomas appear echogenic in ultrasound. Myeloid tissue is heterogeneous in appearance. Hemorrhage and calcification change the sonographic pattern. Hemorrhage appears usually as low echo areas compared to fat, and calcification appears as hyperechoic areas with acoustic shadowing [3]. On CT scans, myelolipomas are well-circumscribed, round or elliptical, hypodense and heterogenous masses. Attenuation values of -120 to -90 HU are characteristic of the adipose tissue, and the presence of fat density is useful and pivotal in diagnosing the mass as a myelolipoma [6]. On MRI, the lesion has high signal intensity on T1WI and intermediate signal intensity on T2WI corresponding to areas of fat. Chemical shift sequences do not objectively quantify any reduction in the opposed-phase images unlike adrenal adenomas which are composed of non-adipocyte cells and are rich in intracellular fat content. However, pixels containing both fat and water may show drop in signal on opposed-phase images [7]. MRI was not done in our case.
We opted for the surgical treatment of the limb because of its size and the local mechanical compression. The final pathology exam confirmed the diagnosis of retroperitoneal myelolipoma without malignancy features. We present the macroscopic aspect of the tumor (Figure 3), we do not dispose of the microscopic pathology.
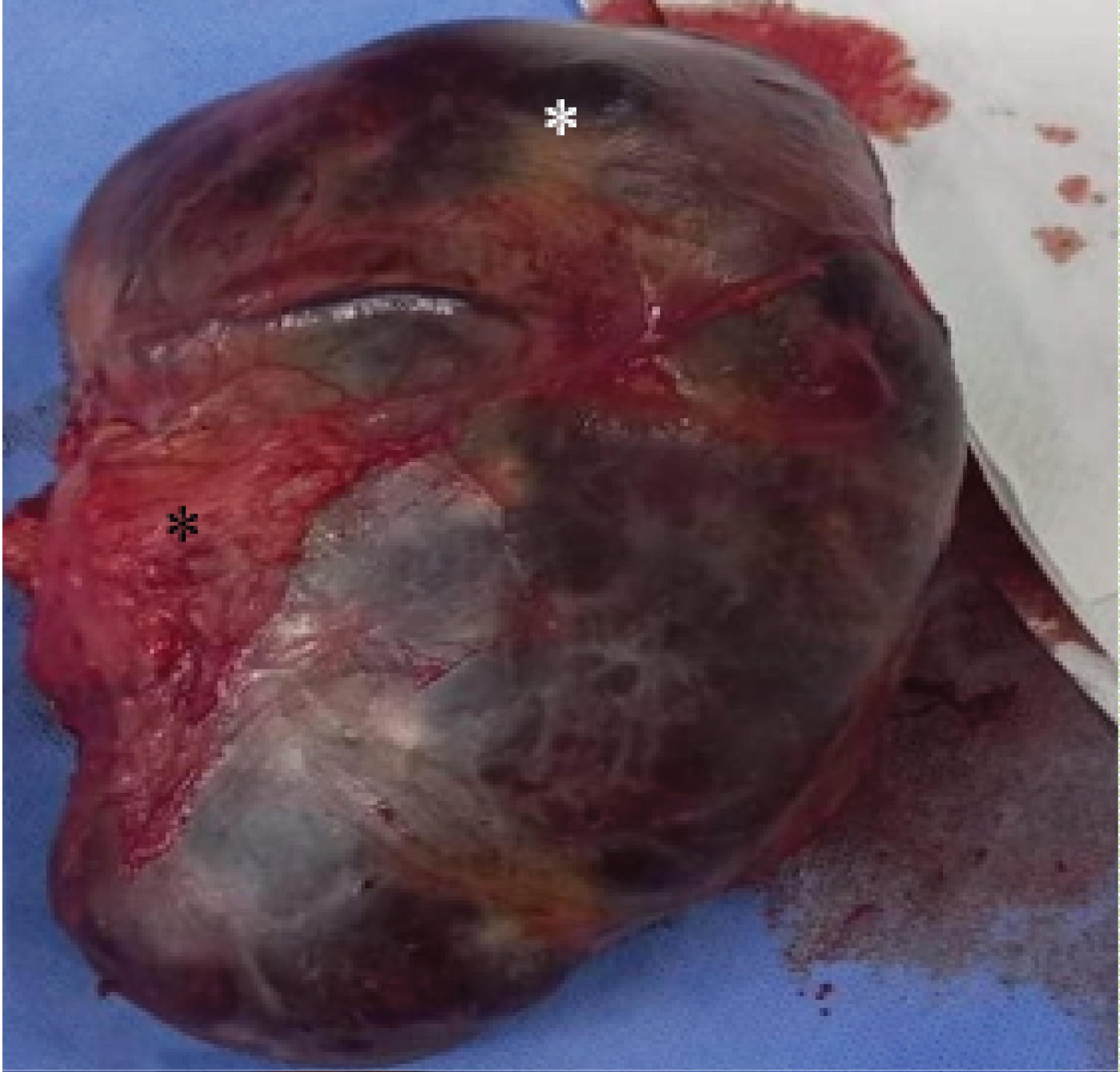 Figure 3: Macroscopic pathology: Huge encapsulated soft tissue measuring 17 × 15 × 5 cm in dimensions and 750 g in weight. Note the red hemorrhagic (black asterisk) areas and the yellow peripheral fatty component (white asterisk).
View Figure 3
Figure 3: Macroscopic pathology: Huge encapsulated soft tissue measuring 17 × 15 × 5 cm in dimensions and 750 g in weight. Note the red hemorrhagic (black asterisk) areas and the yellow peripheral fatty component (white asterisk).
View Figure 3
Although being extremely rare limbs, extra-adrenal myelolipoma, are still to consider in the case of a huge primary retroperitoneum mass with a fatty component and no aggressive features. The final diagnosis is usually based on pathology.
Extra-adrenal retroperitoneal myelolipoma.
• Mature teratoma
• Liposarcoma
• Extramedullary hematopoiesis