There are multiple diagnostic methods for the detection of H. pylori; however, because most are not cost-effective and have low sensibility and specificity, gastric biopsy remains the gold standard for diagnosis. H. pylori's patchy distribution in the gastric mucosa requires multiple biopsy samples to accurately diagnose infection. This study's objective is to identify the diagnostic value of using BLI-Bright with magnification endoscopy as a tool for guided biopsy sampling in patients with suspected H. pylori infection.
This study was conducted by retrospective analysis of 200 case files of patients who underwent upper endoscopy at Christus Muguerza Hospital Sur in Monterrey, Mexico between August 2016 and June 2018. One hundred ninety-three patient files met the selection criteria. To establish the diagnostic significance of occupied/unoccupied gastric pits, sensibility, specificity, and positive and negative predictive values were calculated based on histological findings.
Predicting H. pylori infection in occupied/unoccupied pits has a sensitivity of 66.00%, specificity of 95.10%, a positive predictive value of 85.50%, and a negative predictive value of 88.89%. Analysis of gastric pits using BLI-Bright with magnification endoscopy is more sensitive and specific than rapid urease testing for the diagnosis of H. pylori.
Given its relatively high negative predictive value, finding empty gastric pits suggests a low probability of finding H. pylori. Blue Laser Imaging (BLI)-Bright with magnification endoscopy is not a replacement for histologic examination, but rather a tool to help select potentially infected areas of the stomach based on the appearance of gastric pits.
Magnification endoscopy, BLI-Bright, H. pylori diagnosis, Gastritis
In endemic areas, Helicobacter pylori (H. pylori) infection is typically acquired during the first years of life and is considered one of the most common causes of chronic infection worldwide. Most patients remain asymptomatic for long periods, generally presenting symptoms and complications until adulthood [1,2]. The most common complications associated with H. pylori infection include gastric and duodenal ulceration, adenocarcinoma, and lymphoma [1].
Testing for H. pylori is generally indicated in adults with dyspepsia, peptic ulcer disease, gastric mucosa associated lymphoid tissue (MALT) lymphoma, and early gastric cancer. Testing may also be recommended before starting long-term treatment with NSAIDs or aspirin, in some cases of unexplained iron deficiency, and adults with immune thrombocytopenia [3].
There is currently a wide variety of methods available to diagnose H. pylori infection. Non-invasive methods include H. pylori antigen detection in stool, IgA and IgG antibody detection in serum, urine, and oral samples, as well as the 13C-urea breath test [3]. Invasive tests detect the organism in gastric tissue samples obtained via upper endoscopy and include histopathology, rapid urease test (RUT) (Hp FastTM GI Supply Inc. Camp Hill, PA USA), culture, polymerase chain reaction (PCR), and fluorescence in situ hybridization (FISH) [4].
In adult patients, invasive methods of diagnosis such as gastric biopsy sampling for histologic or rapid urease testing are usually reserved for those with indications for an upper endoscopy. In contrast, non-invasive methods including the urea breath test and stool antigen test are preferred when upper endoscopy is not otherwise required, because this procedure is not routinely indicated for the sole purpose of H. pylori diagnosis [5].
Despite their widespread availability, these diagnostic methods are not particularly cost-effective and have lower sensitivity and specificity than gastric biopsy, which is why the latter remains the gold standard for diagnosis [5]. Given H. pylori's patchy distribution in the gastric mucosa, multiple biopsy samples are required to accurately diagnose infection [1,5]. To reduce the probability of sampling areas of non-infected mucosa, the current recommendation is to obtain 6 gastric biopsies for histopathologic examination, urease testing, and culture from both the antrum and corpus of the stomach [4].
This study proposes the use of Blue Laser Imaging (BLI) and BLI-Bright with Magnification Endoscopy as a tool for taking guided biopsies based on the mucosal appearance to detect H. pylori infection with greater accuracy and precision. This endoscopic technique allows for the identification of gastric mucosal patterns such as pit width and characteristics, vascular pattern, and arrangement. Mucosal areas infected with H. pylori appear altered due to the underlying inflammatory process; the width of gastric pits changes in comparison to normal gastric mucosa, space between pits increases, and in some cases, the blood vessels become less evident. Recognizing altered mucosal patterns may increase the probability of accurately sampling mucosa that is truly infected, thereby markedly reducing the total number of samples needed to make an accurate histological diagnosis.
The study was done by retrospective chart review of 200 patients between 19 and 86 years of age, who underwent upper GI endoscopy at Christus Muguerza Sur Hospital in Monterrey, Mexico between August 2016 and June 2018. Informed consent was obtained for all endoscopic procedures, and approval from the Hospital Ethics Committee was obtained to analyze existing medical records for research purposes. All selected patients presented with one or more of the following symptoms: pyrosis, regurgitation, nocturnal cough, dysphonia, dysphagia, retrosternal chest pain, hemoptysis, and/or unintentional weight loss. Patients who required upper GI endoscopy for any other reason were not included in the study. After meeting inclusion criteria, 7 patients were excluded from the study for having received medical treatment for GI symptoms with drugs such as proton pump inhibitors (PPIs), histamine H2 receptor antagonists, nonsteroidal anti- inflammatory drugs (NSAIDs), mucosal protective agents, and antibiotics within 3 weeks of undergoing EGD.
The endoscopic examination was performed using an optical magnification endoscope (EG-L590ZW) with the FUJIFILM EPX-4450HD LASEREO system. The laser in BLI-Bright, which captures images via high contrast signals (410 nm and 450 nm wavelength) combined with magnification allows for enhancement of the vascular pattern and better visualization of the superficial mucous membrane on the 24-inch LCD monitor. This feature assists the endoscopist in identifying certain mucosal patterns or color changes, thus replacing blind biopsy sampling with guided biopsy sampling.
During each endoscopic procedure, images of the stomach were taken using the BLI-Bright mode before obtaining biopsy samples. The mucosa of the gastric body was first classified as having type 1, 2, 3, or 4 gastritis based on the description proposed by Anagnostopoulos, et al. in which type 1 pattern of gastritis is identified when there is a honeycomb-type subepithelial capillary network (SECN) with a regular arrangement of collecting venules and round pits [6]. Within this same classification, type 2 gastritis refers to a honeycomb-type SECN with loss of collecting venules, and the type 3 pattern is characterized by the loss of normal SECN and collecting venules, with white enlarged pits surrounded by erythema [6]. Finally, type 4 gastritis is characterized by the loss of normal SECN and round pits, with an irregular arrangement of collecting venules [6].
After identification and classification of gastritis, the gastric body's pits were then classified as being occupied or unoccupied based on their appearance. Unoccupied (empty) pits were identified for having a dark, round, central umbilication (Figure 1A and Figure 1B), whereas occupied pits lacked the dark central umbilication seen in unoccupied pits (Figure 1C and Figure 1D) [6,7]. Occupied pits seen with BLI-Bright are characteristic of H. pylori infection and suggest an ideal place for biopsy sampling. Therefore, the goal was to target biopsy sampling to regions of gastric body's mucosa with pit patterns suggestive of H. pylori infection [6,7]. Whenever BLI revealed occupied crypts in the gastric body, 2 samples were taken specifically from that and an additional 4 samples were then taken from random mucosa of the gastric antrum. When only unoccupied pits were identified in the gastric body, samples were taken from randomly selected mucosa of the antrum and corpus of the stomach, as has been done before the introduction of BLI-Bright and magnification endoscopy.
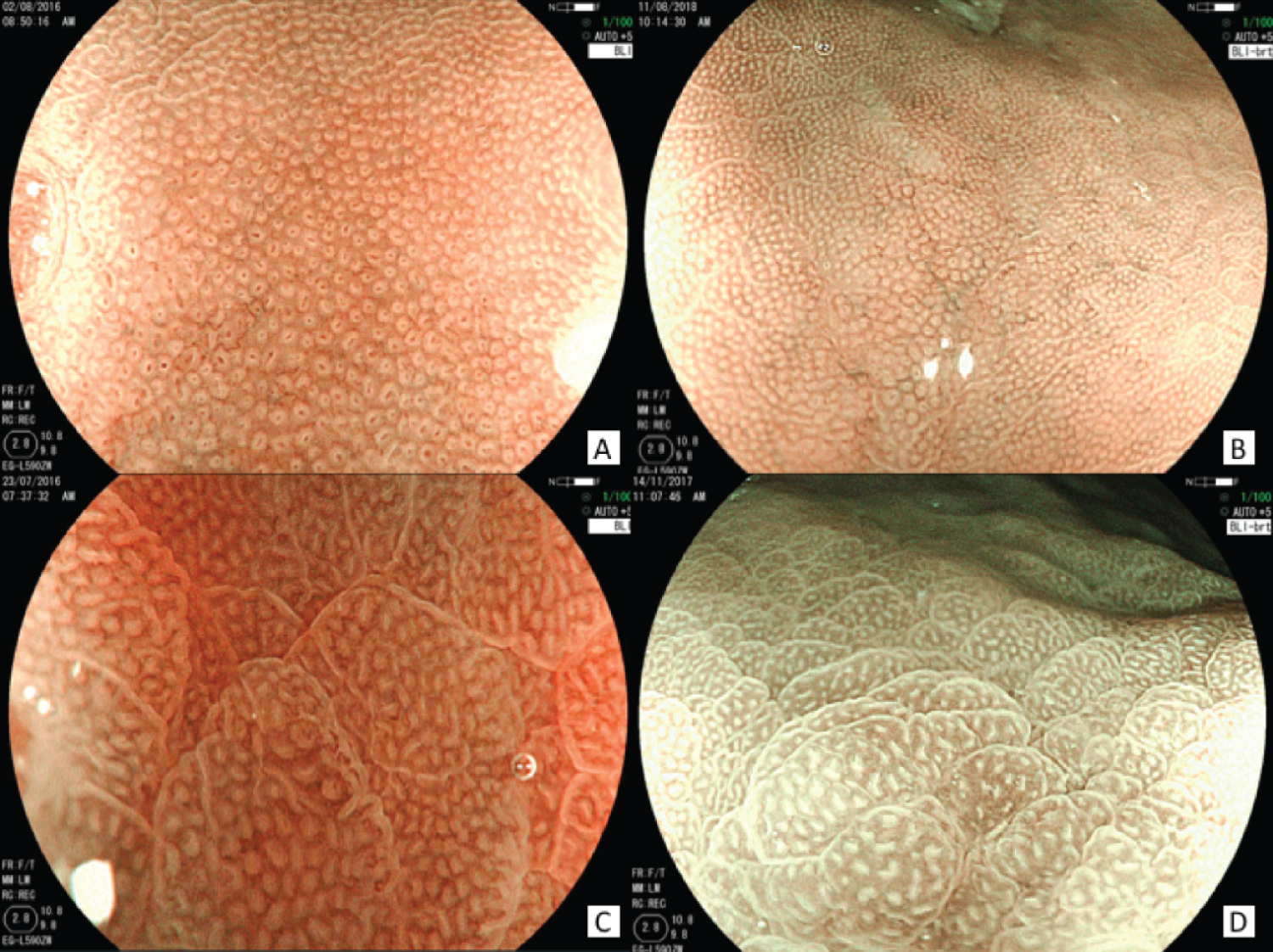 Figure 1: Empty pits visualized in BLI mode (A) and BLI-Bright mode (B), showing a dark round central umbilication. Occupied (filled) pits in BLI mode (C) and BLI-Bright mode (D), showing enlarged white pits that lack a central umbilication, surrounded by erythema.
View Figure 1
Figure 1: Empty pits visualized in BLI mode (A) and BLI-Bright mode (B), showing a dark round central umbilication. Occupied (filled) pits in BLI mode (C) and BLI-Bright mode (D), showing enlarged white pits that lack a central umbilication, surrounded by erythema.
View Figure 1
Therefore, 6 samples were taken from each patient; 2 stomach antrum samples for RUT, plus 2 antrum and 2 corpus samples for Modified Giemsa staining (Diff-Quik). The Modified Giemsa staining process consists of fixing the biopsy specimen with 10% formalin and immersing it in basophilic and eosinophilic solutions to visually identify the bacteria. This is considered the gold standard for diagnosis and thus, a finding H. pylori on a biopsy sample stained with Modified Giemsa defines infection.
Descriptive statistics of the sample were examined using frequencies and proportions for qualitative variables, and mean and standard deviation or median and minimum and maximum values for quantitative variables. Categorical variables were compared using the Chi-Square test, and quantitative variables were compared using the T-Test or Mann-Whitney U test according to normality. Statistical analysis was performed using SPSS v23.0 (Chicago, IL, USA). Sensitivity, specificity, positive and negative predictive value, positive and negative likelihood ratio were calculated using Med Calc Software Ltd. Diagnostic test evaluation calculator (https://www.medcalc.org/calc/diagnostic_test.php), Version 20.015; accessed November.
Two hundred and four patient files met the inclusion criteria and a total of 193 patients remained after the exclusion, 50.8% of which were female. The average patient age was 43 years ± 15.3. The predominant clinical symptoms were pyrosis (37.3%), abdominal pain (36.3%), and regurgitation (23.8%). Other symptoms were present less frequently: nausea (19.7%), retrosternal chest pain (13.0%), dysphagia (11.4%), vomiting (10.4%), cough/dysphonia (10.4%), gastrointestinal bleeding (6.7%), weight loss (3.1%), choking sensation (1.6%).
To establish the diagnostic significance of occupied/unoccupied gastric pits, sensibility, specificity, and positive and negative predictive values were calculated based on histological findings (gold standard) (Table 1). The statistical findings for predicting H. pylori infection in occupied/unoccupied pits in this group of patients are as follows: sensitivity 66.00% (95% confidence interval [CI] 51.23%-72.79%), specificity 95.10% (95% CI 90.17%-98.01%), positive predictive value (PPV) 82.50% (95% CI 69.02%-90.89%), negative predictive value (NPV) 88.89% (95% CI 84.44%-92.18%). This study also found that RUT (Hp FastTM GI Supply Inc) had a sensitivity of 58.00% (95% CI 43.21%-71.81%), and specificity of 83.92% (95% CI 76.85%-89.52%), with a PPV of 55.77% (95% CI 44.75%-66.25%) and NPV of 85.11% (95% CI 80.37%-88.86%) (Table 2).
Table 1: Sensibility, specificity, and positive and negative predictive values of gastric pit appearance. View Table 1
Table 2: Sensibility, specificity, and positive and negative predictive values of RUT. View Table 2
One hundred percent of the endoscopies revealed gastritis. Classification of the type of gastritis was made based on the mucosal patterns described by Anagnostopoulos, et al.: 58.0% of cases displayed a subepithelial capillary network with a honeycomb appearance, coupled with a regular arrangement of collecting venules and round pits (type 1 gastritis), 31.6% showed loss of the collecting venules (type 2 gastritis) and 10.4% were found to have a loss of the normal subepithelial capillary network and collecting venules in addition to enlarged, white pits surrounded by erythema (type 3 gastritis) [6]. The type 4 pattern of gastritis was not identified in any case. The most prevalent gastritis was type 1; 85.7% of patients with type 1 gastritis had a negative biopsy result and 95.5% had an empty crypt appearance on magnification endoscopy. Type 3 gastritis was the least common, found in only 20 patients (10.4%). However, 70.0% of patients with type 3 gastritis had a positive biopsy result (Table 3) and 75.0% had occupied crypt appearance on magnification endoscopy (Table 4).
Table 3: Correlation between the type of gastritis identified on magnification endoscopy and H. pylori infection. P = 0.001. View Table 3
Table 4: Correlation between the type of gastritis identified on magnification endoscopy and crypt appearance. P = 0.001. View Table 4
Other endoscopic findings included the presence of collecting venules, which were seen in 51.1% of endoscopies, increased space between pits (41.5%), filled pits (20.72%), and gastric and duodenal ulcers, which were found in 4.1% and 2.1% of patients, respectively.
Empty or unoccupied gastric pits, identified by magnification endoscopy for having a central umbilication, are representative of an H. pylori - free mucosal surface, whereas occupied pits, which lack said umbilication, are associated with infection and correspond to the ideal place to take a sample for histological examination. Given their high negative predictive value, empty pits suggest a very low probability of finding H. pylori when using the gold standard for diagnosis. This study also found that analyzing whether pits are empty or occupied has greater diagnostic value (sensibility, specificity, positive predictive value, and negative predictive value) than RUT (Hp FastTM GI Supply Inc) (Table 1 and Table 2). Altogether, these findings suggest that the use of magnification-guided biopsy sampling serves as an excellent tool in the diagnosis of H. pylori.
Based on magnification endoscopy, it was found that mucosal patterns consistent with type 3 gastritis (i.e., enlarged, white pits surrounded by erythema and loss of the normal subepithelial capillary network and collecting venules) were more commonly associated with positive H. pylori biopsy results and occupied pit appearance [6]. Grading of gastritis was based solely on the mucosal appearance revealed by magnification endoscopy, and not on the degree of inflammation seen on histopathologic examination, which is why the Sydney Classification that is typically used for grading chronic gastritis associated with H. pylori infection is not included in this article [8]. The significance of the association between the type of gastritis revealed histologically and the patterns seen on magnification endoscopy is beyond the scope of this study.
Regardless of these findings, biopsy-based testing for visual identification of the bacteria is still the most accurate diagnostic tool to confirm or rule out H. pylori infection. It is considered the gold standard, but its outcome and reliability are influenced by location and the number of samples taken [9]. Serology used to be the most frequently ordered test in the United States, but low sensitivity and specificity, lack of reimbursement from insurance companies, and the need for confirmatory tests have obliterated the demand for this method, making gastric biopsy the most common diagnostic tool followed by stool antigen immunoassay testing [10].
We identified data regarding the prevalence of H. pylori-infected mucosa that was quite interesting despite extending beyond the primary purpose of this study. H. pylori is said to infect up to half of the world's population [11,12]. The prevalence of infection varies with age and geographic and socioeconomic factors. Nonetheless, prevalence is considered to oscillate between 50-60% in western countries, reaching up to 80% in developing countries [11-13]. In this cohort, colonization of gastric mucosa with H. pylori was found to be 25.9% (Table 3), which is considerably less than expected. The discrepancy between this study's findings and data previously published may be explained by the socioeconomic status of the patients included in this research project. The subjects were selected from a private hospital in Monterrey, Mexico, which translates into the fact that they mostly pertain to the middle and upper socioeconomic class. Therefore, even though this study may underestimate the prevalence of H. pylori infection as compared to the general population, these findings still raise the question of whether or not incidence and prevalence are truly decreasing in the general population. Further cross-sectional and cohort studies analyzing the role that socioeconomic status plays in the prevalence of H. pylori are needed to determine the true meaning of this study's secondary findings.
Even though there is a limited number of studies that explore magnification endoscopy findings in H. pylori-infected patients, this technique currently plays an important role in evaluating Barrett's Esophagus, studying premalignant and malignant mucosal lesions of the stomach, gastric atrophy, and intestinal metaplasia [14-17]. This study main limitation is the fact that there are few works like it; while existing reports discuss the relevance of certain mucosal patterns seen on magnification endoscopy in patients with H. pylori infection, more studies centered around the diagnostic potential of crypt appearance (occupied/unoccupied) are yet to be developed. A study discussing the endoscopic features of H. pylori-infected mucosa using various techniques found that visualizing obliterated collecting venules with BLI is 98.00% sensitive and 92.00% specific for the diagnosis of H. pylori [18]. Even though the study's objectives and methodology differ from our own, these findings support the idea that the inflammatory changes induced by the bacteria can be identified with magnification endoscopy and aid in the diagnosis of infection.
This study's prime purpose, which was to identify the diagnostic value of using BLI- Bright and magnification endoscopy during biopsy sampling in patients with suspected H. pylori infection was met, revealing that this technique does, in fact, improve the endoscopist's ability to identify altered mucosal patterns secondary to H. pylori infection. BLI-Bright magnification endoscopy is not a replacement for histologic examination, but rather a tool to help select the potentially infected areas of the stomach based on the appearance of the gastric pits, which could increase the accuracy of biopsy for detection of H. pylori. Ongoing research comparing random blind biopsy sampling with BLI-Bright- guided sampling and endoscopic identification of altered mucosal patterns may enhance these new methods' diagnostic potential, thereby reducing the number of samples needed to make an accurate diagnosis, patient risk, and procedure expenses.
This manuscript is submitted on behalf of the following authors, all of which have participated in the work to be published:
Ulises Leal-Quiroga: Conception, study design, clinical analysis, data acquisition, revision of intellectual content, corresponding author; Abigail Sara Kane: Data collection, manuscript drafting, revision of intellectual content, writing assistance, language editing, proofreading, co-author; Eduardo Mendoza-Fuerte, Clinical analysis and data acquisition; Omar David Borjas-Almaguer: Analysis and interpretation of statistical data; Eugenia Leal: Data collection, proofreading; Rafael Castañeda-Sepúlveda: Proofreading.