Spontaneous rupture of the renal pelvis is one of the rare complications and is commonly known to occur secondary to obstructed distal ureteric calculus [1]. Malignant ureteric obstruction and bladder outlet obstruction are few other causes that could like to rupture of renal pelvis secondary to the back pressure changes [2]. Pregnancy is one of the non-renal extra-luminal causes of the spontaneous renal fornix rupture [3]. However, blowout of renal pelvis secondary to an obstructing bowel has not been reported earlier. We decided to report this case as the twisted sigmoid mesentery resulted in extrinsic compression of the distal ureter leading to spontaneous rupture at the Pelvic- Ureteric Junction (PUJ) as a result of severe back pressure changes. Sigmoid volvulus is one of the common causes of intestinal obstruction accounting for 2 to 5% of emergency case load in the western world [4]. The sigmoid colon twists around its own mesentery leading to intestinal obstruction and a compromised blood supply [5].
A 57-year-old lady was admitted as emergency with abdominal pain and distension. Her background included cerebral palsy and learning difficulties for which she was institutionalized. There were no previous surgical or urological issues for this lady. The caretakers had noted progressive abdominal distension and no bowel movements for four days and hence subsequent surgical referral.
Vital parameters on admission showed a pulse of 100 beats per minute, blood pressure of 130/80 mmHg and O2 saturation of 96% on room air. The abdomen was distended, tense and tender on palpation but no guarding or rigidity was elicited. Rectal examination showed an empty rectum. Patient responded well to initial resuscitation.
Blood investigations showed a Hemoglobin of 137 g/L (Normal 110 g/L-165 g/L), raised white cell count of 17.6 × 109/L (reference 4.5 × 109/L - 11 × 109/L), normal platelets and C reactive protein (CRP) of 70 mg/L (Normal < 10 mg/L). Her electrolytes, liver and renal functions were essentially normal. The eGFR at the time of presentation was 82 (reference range > 90). Urine dip stick examination was essentially within normal limits. Her chest X-ray did not identify any evidence of pneumoperitoneum while abdominal X-ray showed a classic coffee bean sign suggestive of a volvulus (Figure 1). A Computerized Tomography scan (CT scan) of Abdomen and Pelvis confirmed the features of volvulus and no other bowel related pathology was identified. No other intra-abdominal catastrophes noted on the initial CT scan.
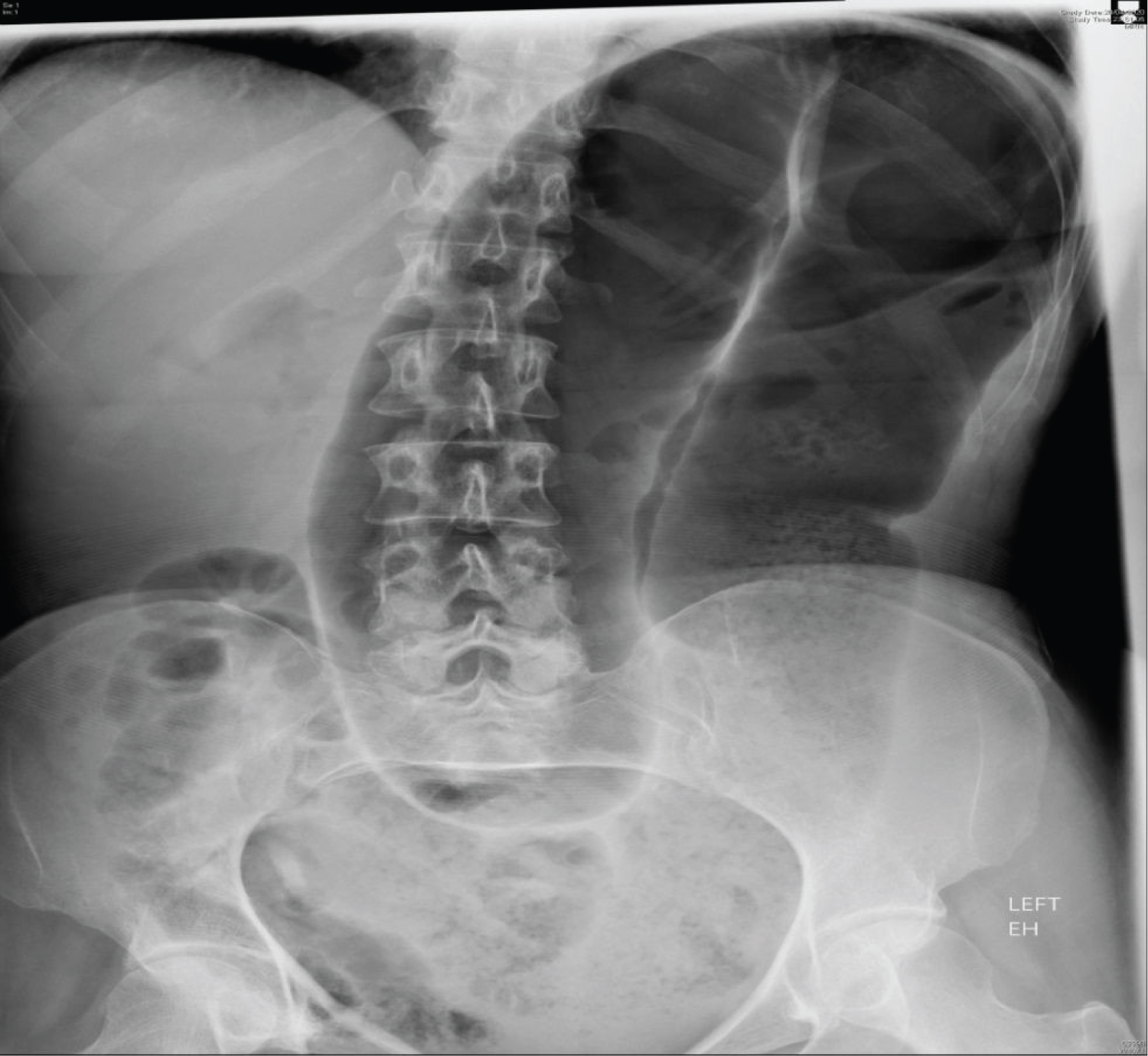 Figure 1: Plain X-ray of the abdomen showing classic omega "coffee-bean" sign.
View Figure 1
Figure 1: Plain X-ray of the abdomen showing classic omega "coffee-bean" sign.
View Figure 1
A rigid sigmoidoscopy with flatus tube insertion was performed to decompress the bowel, and was successful to some extent. The intention was to decompress the bowel as soon as possible and the procedure was carried out in the ward. Due to ongoing COVID crisis, the surgical intervention was deferred unless definitely indicated and, therefore, a flexible sigmoidoscopy with bowel decompression was planned as next intervention. As flexible sigmoidoscopy was an aerosol generating procedure and with certain restrictions in place during the pandemic, it was worthwhile to proceed with rigid sigmoidoscopy rather than flexible sigmoidoscopy.
The following day, the patient appeared more distressed and complained of intermittent colic in the left flank pain. Clinical assessment showed increasing tenderness over abdomen. Repeat blood investigations showed markedly raised inflammatory markers with CRP of 430 mg/L (Normal < 10 mg/L) and blood gases showed metabolic acidosis. Interestingly, the renal functions demonstrated a rapid drop in eGFR to 32 (reference range > 90). The serum creatinine which was 86 umol/L (reference range: 49-90 umol/L) at the time of admission raised to 141 umol/L (reference range: 49-90 umol/L) the following day. An urgent CT scan of Abdomen and pelvis with contrast was ordered to rule out ischemic gut. CT scan demonstrated a left sided hydronephrosis and hydroureter associated with active extravasation of contrast from the left renal pelvis into the retroperitoneum indicating a rupture (Figure 2). The dilatation of the ureter was evident till the lower end where the root of the sigmoid mesentery is attached. CT also reported that there was no evidence of contrast in the distal ureter and the ureter was non-dilated beyond the transition point of extrinsic compression. The rupture appeared spontaneous as a result of extrinsic compression of twisted sigmoid mesentery. The bowel wall of the sigmoid colon appeared non-enhancing suggesting ischemia.
 Figure 2: Coronal oblique maximum intensity projection image from post-contrast urographic phase CT scan showing dilated left pelvicalyceal system and contrast outside the PCS suggesting leak.
View Figure 2
Figure 2: Coronal oblique maximum intensity projection image from post-contrast urographic phase CT scan showing dilated left pelvicalyceal system and contrast outside the PCS suggesting leak.
View Figure 2
The patient�s presentation was discussed urgently with the urologists. A Double J-stent (DJ stent) was inserted in the left renal tract under fluoroscopic guidance (Figure 3). Subsequent laparotomy revealed a non-viable gangrenous segment of sigmoid colon twisted at the root of its mesentery. Sigmoid colectomy was carried out with end colostomy.
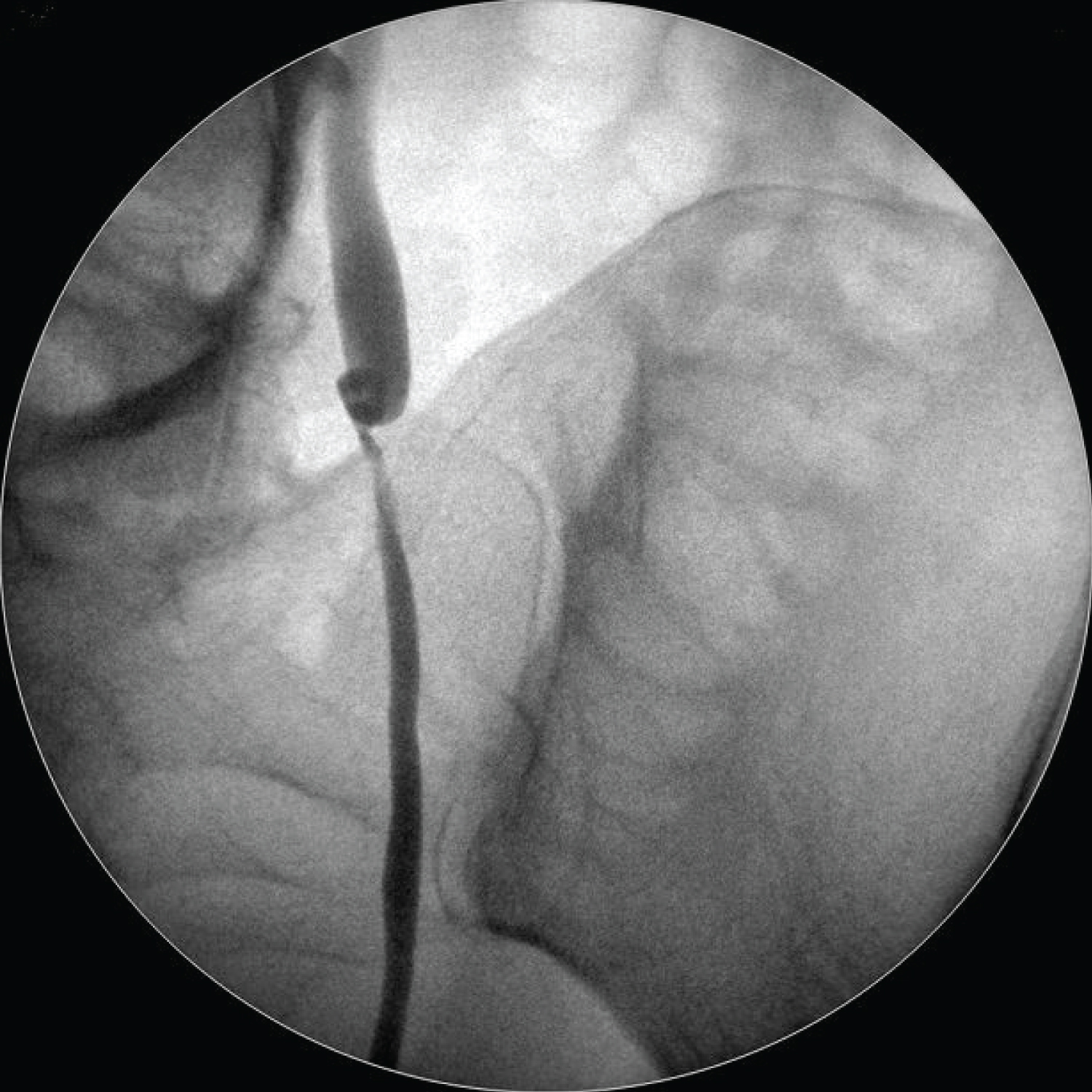 Figure 3: Intra-operative fluoroscopic guided image of the ureter.
View Figure 3
Figure 3: Intra-operative fluoroscopic guided image of the ureter.
View Figure 3
The patient made an uneventful recovery and was discharged 2 weeks following her admission with further support from the community nurses. The urologists removed the stent after an interval of 3 months. There were no urological issues after the stent was removed. Throughout this episode, her family members were kept involved in the discussions and decisions.
Wunderlich in 1856 first described spontaneous rupture of renal pelvis (SRRP) as �Spontaneous apoplexy of renal capsule� [6]. The extravasation of urine in peri-nephric space due to ruptured renal pelvis is commonly associated with obstructive ureteric stone. Flank pain radiating to groin is most common clinical presentation. SRRP is also associated with hematuria [7]. Serial ultrasound examinations, contrast enhanced CT scans and Intravenous Pyelogram are commonly employed imaging studies used for diagnosis of SRRP [8]. Diversion of urine by means of a Double J-stent or a percutaneous nephrostomy are the treatment modality employed for small ruptures of renal pelvis [9].
Sigmoid volvulus is one of the common causes of large bowel obstruction. The Latin term "volvere" which means "to roll" is the origin of word volvulus [10]. The incidence of sigmoid volvulus increases with advancing age and is also known to occur in patients with neuro-psychiatric illnesses, chronic constipation and overuse of laxatives. The sigmoid volvulus is seen more commonly in population who consume high fiber in their diet [11].
The sigmoid flexure of the colon is the most frequent site of volvulus to occur [12]. The sigmoid colon twists around its own mesentery leading to significant intra-luminal obstruction that may compromise its blood supply [13]. Torsion in the sigmoid colon produces a closed loop obstruction due to a patent ileo-ceacal valve. The proximal colon distends with air and fluid giving rise to the characteristic X-ray feature that resembles a coffee bean [14]. The resulting increase in intraluminal pressure progressively compromises venous and then arterial flow. This results in serious complications and also changes the prognosis of such patients if not treated immediately.
While majority of patients present with long standing abdominal symptoms such as distension or intermittent pain, a small percentage present as acute abdomen [15]. Common complications of sigmoid volvulus include intestinal ischemia with subsequent gangrene and perforation. The mortality rate due to sigmoid volvulus rises significantly in the presence of complications [16]. Therefore, this condition would warrant an immediate intervention.
The aim is to deflate/decompress the bowel by passing a flatus tube beyond the obstruction or endoscopic measures involving sigmoidoscopy to pass beyond the obstructing point. The other ways include percutaneous fixation of colon (sigmoidopexy) or percutaneous sigmoid colostomy. Laparotomy is usually considered if there is clinical deterioration and in the suspicion of complications due to sigmoid volvulus [17].
In our patient as a result of the pressure exerted by twisted mesentery on the left distal ureter resulted in gross hydroureteronephrosis and subsequent rupture at the pelvic-calyceal region. The probable reasons behind spontaneous renal pelvis rupture could have been due to the traction exterted by sigmoid volvulus on the ureter. The tractional force resulted in disruption injury of renal pelvic-ureteric junction as it is one of the weakest point of the urinary system. Other possibility could be an avulsion secondary to acceleration-deceleration injury affects pelvic-ureteric junction as there is a change in calibre of the ureter. The lower circumferential tensile strength in proximal ureter could have also been a contributory factor for rupture at this site [18]. Furthermore, the rupture of renal pelvis could be secondary to back pressure changes that lead to high intra-ureteric pressure due to obstructed distal ureter [19].
The spontaneous rupture of renal pelvis is secondary to sigmoid volvulus, to our best of knowledge has not been reported so far in the literature and such possibility should be kept in mind by the treating team.
A. Spontaneous rupture of ureter commonly occurs at renal fornix. Rupture of renal pelvis usually occurs secondary to obstruction of distal ureter.
B. The symptoms of renal pelvis rupture mimic a renal colic. Stenting of ureter is treatment modality employed for small ureter ruptures.
C. Sigmoid volvulus is a common surgical emergency and prompt intervention is needed to prevent further complication.
D. Having a high index of suspicion for extra-intestinal complications would help in early identification and prompt intervention.
E. There is no uniform consensus to manage these patients and the management is tailored to individual patients. A multi-disciplinary team input at an early stage improves patient outcome.