Spontaneous pneumomediastinum (SPM) in children was first defined by Hamman in 1939, Its Association to a posterior tracheal tear is even more uncommon. We report the case of an 18-month-child that presented a SPM associated to a posterior tracheal tear. The patient had no medical history and presented two days before her admission a dry cough and a shortness of breath. The radiological investigation showed a pneumomediastinum with an extensive subcutaneous emphysema and a posterior tear in the trachea. A conservative approach was adopted with a monitoring and surveillance of the regression of the emphysema, that showed a good evolution of the patient.
The rare cases published in the literature make it hard to understand the features of this presentation, but the conservative approach has shown great results in patients as the prognosis is still favorable.
Spontaneous pneumomediastinum, Peadiatric, Tracheal breach
Spontaneous pneumomediastinum (SPM) in children was first defined by Hamman in 1939 [1] as the leak of air in the mediastinum though there are no underlaying pulmonary pathologies nor any traumatic event. Its Association to a posterior tracheal tear is even more uncommon. We report the case of an 18-month-child that presented a SPM associated to a posterior tracheal tear, and we review the cases reported in the literature and discuss the different treatment management proposed by the authors.
We report the case of B.L an 18-month-old child, with no particular medical history; no history of asthma, a cervicothoracic trauma nor any history of intubation; who presented 2 days before her admission a dry cough followed by a sudden onset of a shortness of breath and an extensive oedema.
The patient got admitted to peadiatric intensive care as she was instable with a heart rate at 120 bpm, polypnea at 40 cpm and thoracoabdominal balancing and intercostal pulling with 93% oxygen saturation in ambient air.
The clinical examination noted the presence of thoracic, cervical and facial subcutaneous emphysema with subcutaneous crepitation, Hamman's sign. Pulmonary auscultation revealed crackling rales projecting to the cardiac area. The rest of the examination was normal. The initial biological assessment made of Blood cell count, C-reactive protein, ionogram showed no abnormality.
The cervicothoracic CT scan was performed in the emergency room and allowed the individualization of a large pneumomediastinum and an extensive subcutaneous emphysema dissecting the thoracic, cervical and facial tissues. No foreign body was individualized nor any other sign laryngotracheal obstruction (Figure 1, Figure 2 and Figure 3).
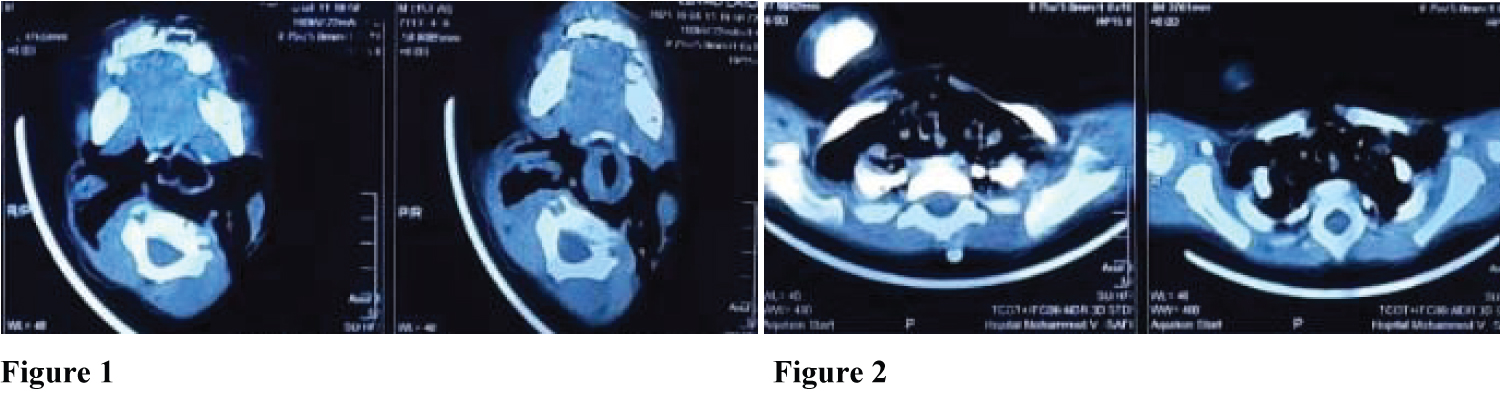 Figure 1: Axial section of cervicothoracic CT scan, showing an extensive subcutaneous emphysema dissecting the face tissues.
Figure 1: Axial section of cervicothoracic CT scan, showing an extensive subcutaneous emphysema dissecting the face tissues.
Figure 2: Axial section of cervicothoracic CT scan, showing an extensive subcutaneous emphysema dissecting the thoracic tissues.
View Figure 1 & 2
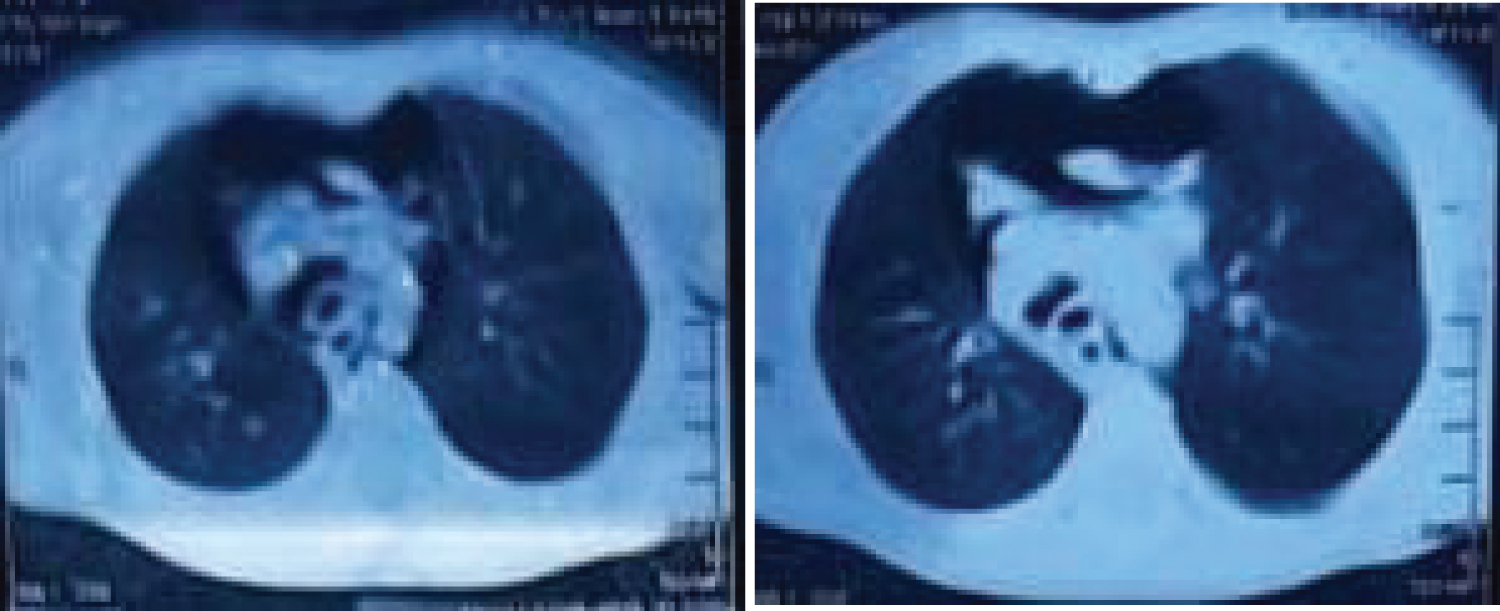 Figure 3: Axial section of cervicothoracic CT scan, showing the pneumomediastinum.
View Figure 3
Figure 3: Axial section of cervicothoracic CT scan, showing the pneumomediastinum.
View Figure 3
The conservative approach was decided with close monitoring of the patient. Prophylactic antibiotic therapy was given with discontinuation of feeding and monitoring of the clinical condition.
A second Cervicothoracic CT scan was performed after 48 hours and showed a continuity solution in the posterior tracheal wall at the C7 vertebra level, measuring 3.1 mm and extending over 2.9 mm, with no clearly individualizable foreign body; complicated by a large anterior and posterior pneumomediastinum radiating to the cervical region and a subcutaneous emphysema dissecting the cervical soft tissues, chest wall and axillary regions, extended to the deep spaces of the face (Figure 4 and Figure 5).
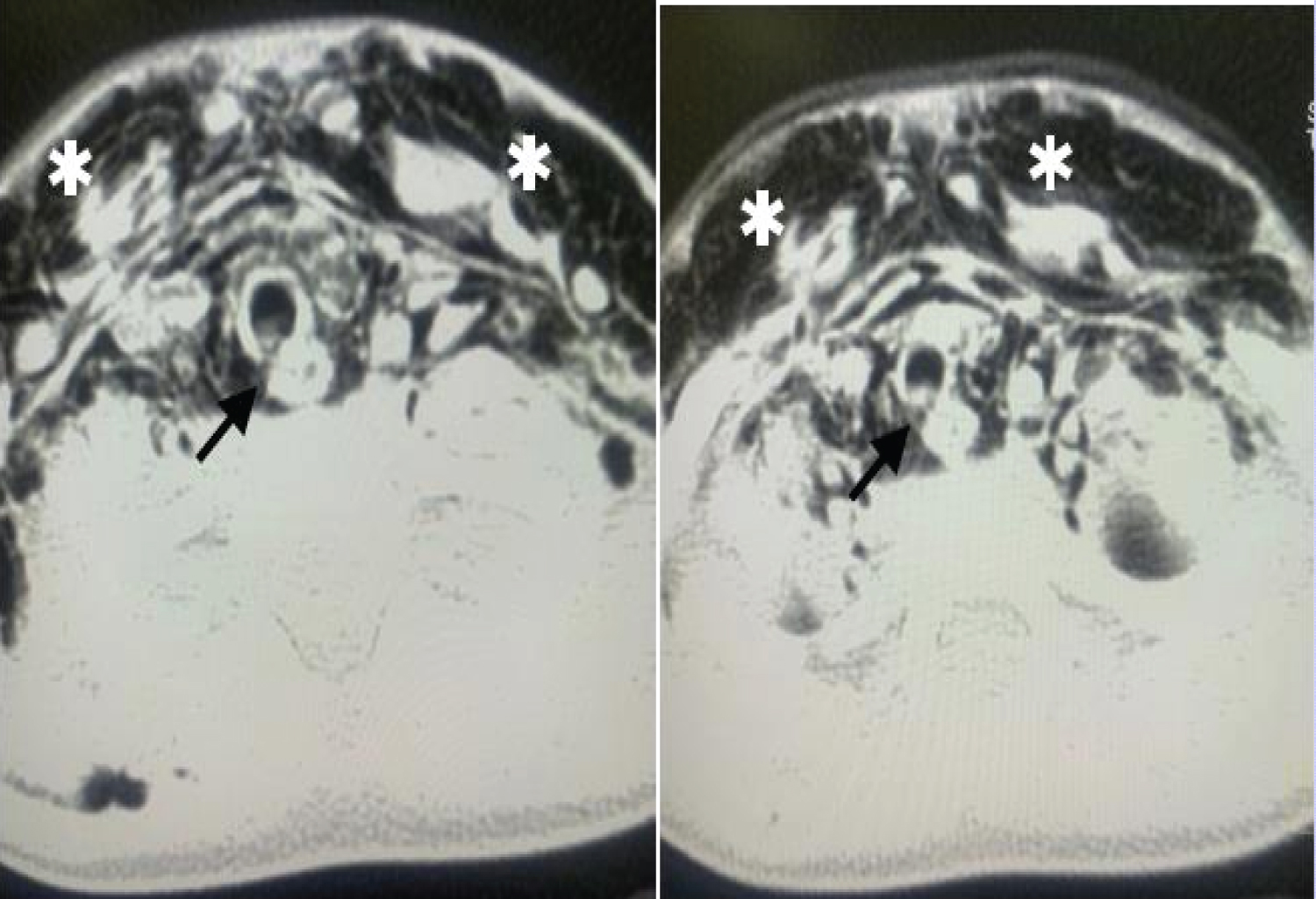 Figure 4: Axial section of a cervicothoracic CT scan. The arrow points to the continuity solution of the trachea. The asterixis shows the dissection subcutaneous emphysema.
View Figure 4
Figure 4: Axial section of a cervicothoracic CT scan. The arrow points to the continuity solution of the trachea. The asterixis shows the dissection subcutaneous emphysema.
View Figure 4
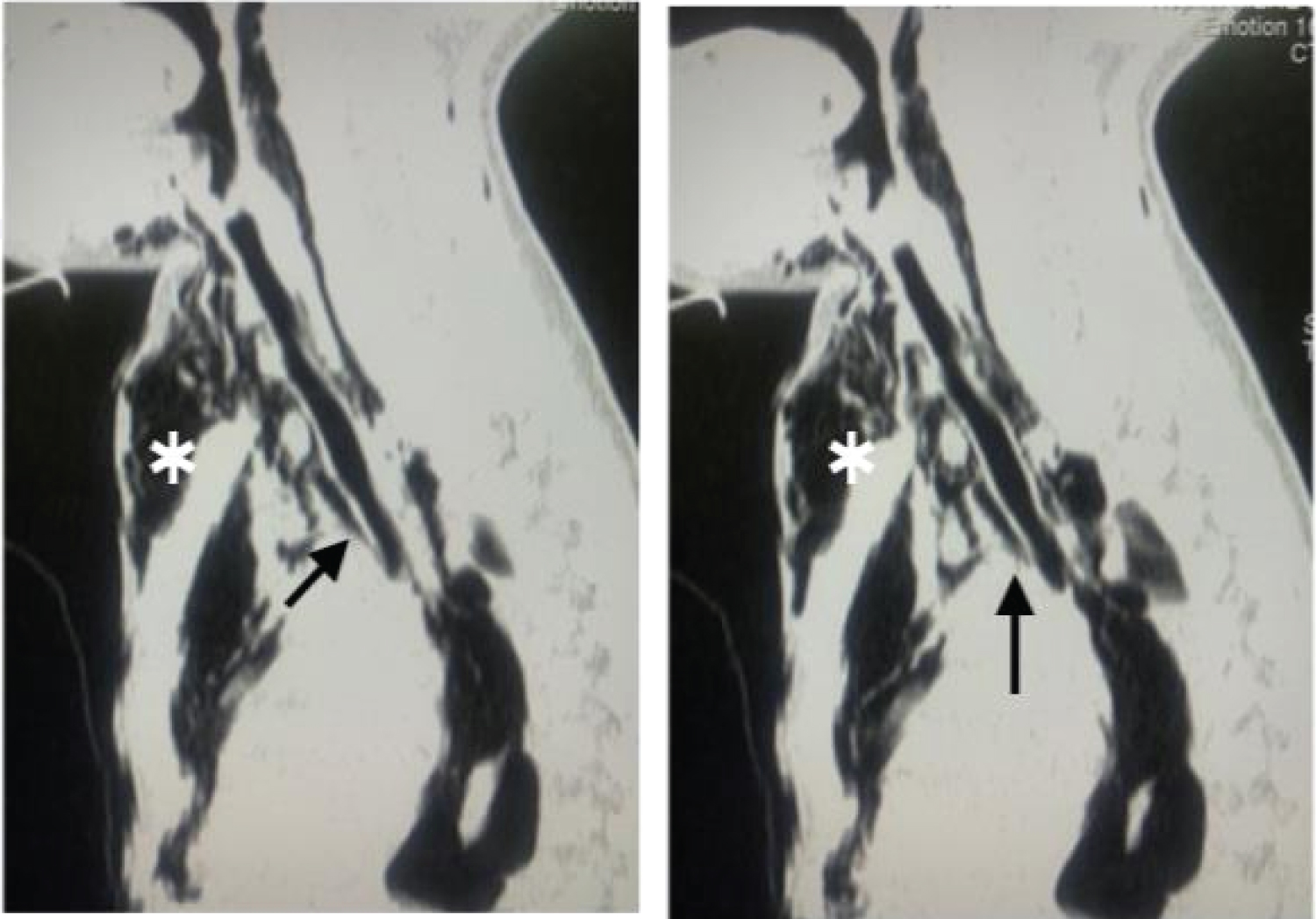 Figure 5: Sagittal section of a cervicothoracic CT scan. The arrow points to the continuity solution of the trachea. The asterixis shows the dissection subcutaneous emphysema.
View Figure 5
Figure 5: Sagittal section of a cervicothoracic CT scan. The arrow points to the continuity solution of the trachea. The asterixis shows the dissection subcutaneous emphysema.
View Figure 5
The evolution was favorable, after 72 hours of monitoring, with progressive regression of the subcutaneous emphysema and signs of respiratory struggle (Figure 6 and Figure 7).
 Figure 6: Picture showing the subcutaneous emphysema after 48 H of the patient admission.
View Figure 6
Figure 6: Picture showing the subcutaneous emphysema after 48 H of the patient admission.
View Figure 6
 Figure 7: Picture showing the subcutaneous emphysema after 5 days following the patient admission and a notable regression of the subcutaneous emphysema.
View Figure 7
Figure 7: Picture showing the subcutaneous emphysema after 5 days following the patient admission and a notable regression of the subcutaneous emphysema.
View Figure 7
Spontaneous pneumomediastinum (SPM) in children is rare and represents 1/400 of admission in the emergency room [2,3], It was first described by Hamman in 1939 [1,4] it is defined by the presence of air in the mediastinum with no underlaying lung disease nor any traumatic or surgical procedure, it is mostly described in early twenties sportive young adults [3,5]. In children it is mostly seen between the age of 3 to 4-years-old [6]. The association of a SPM and a spontaneous rupture of the trachea are even more uncommon. This association is mostly reported following a violent trauma [7,8].
The etiopathogenesis behind it isn't clear, though there are two mechanisms reported: Increased intra-alveolar pressure and reduced interstitial pressure [5,9-11]. A spontaneous alveolar or a respiratory bronchiole rupture may cause the leak of air in the mediastinum [3,6,7]. In a case reported by S. Ohja in 2018, stated the case of a 12-year-old male child that presented a SPM associated to a tracheal breach and surgical emphysema, and assumed that it could be secondary to a preexistent posterior tracheal wall weakness, that ruptured and caused the SPM [12].
The main clinical presentation found in the literature are chest pain, dyspnea, Hamman's sign; A hallmark sign that is a precordial crepitation heard with cardiac systole; and crepitus on palpation [1,6,13]. The CT scan is the main investigation to assess the diagnosis and shows the extension of the SPM and its association to a possible tracheal breach, a pneumothorax or a subcutaneous emphysema [6,12-14].
M. Tortajada, stated that the SPM is usually benign and self-limiting, and should be treated conservatively without the need of an invasive procedure [14]. Other authors share this same point of view as a simple observation and administration of prophylactic antibiotics, to prevent the occurrence of mediastinitis, are the gold standard of treatment of SPM. As for the posterior tracheal rupture the surgery is mainly indicated if the tear is superior to 2 cm [12], if not the conservative attitude with a good surveillance of the patient is the best option in these cases. The prognosis is favorable [12,13,15].
The origin of the spontaneous pneumomediastinum and the spontaneous rapture of the trachea is still not understood as the cases reported in the literature are still rare. The conservative approach is the best therapeutic option as it has shown a great regression of the symptomatology and a good evolution of the patients.
The authors declared that there is no conflict of interests.
None.
Informed consent was obtained from the patient's mother for publication of this case report and accompanying images.