Ceruminous Pleomorphic Adenoma is a very rare, benign neoplasm originating from the ceruminal glands in the external auditory canal. Clinical manifestations are nonspecific. Meticulous preoperative clinical, pathologic, and radiologic evaluations are crucial in effective management of patients.
Its diagnosis depends on identification of proliferation of regular epithelial and myoepithelial cells embedded in a chondromyxoid stroma. We present a case of pleomorphic adenoma of external auditory canal diagnosed in a 25-year-old female Ethiopian patient hoping to help clinicians and pathologists in recognizing this rare benign neoplasm.
Pleomorphic adenoma, External auditory canal, Ethiopia, Ceruminous adenoma
Pleomorphic adenoma (PA) is a benign tumor arising mainly from major salivary glands. It also arises from minor salivary glands, lip, check, nasal cavity, bronchus, skin, breast, and soft tissues [1].
A much rarer site of origin is external auditory canal (EAC), as first described in 1951 [2]. Since then, only 49 cases in 44 articles published in English language have been reported in the literature [3].
Ceruminous glands, modified apocrine glands, located primarily in the skin lining cartilaginous/membranous portion of EAC are believed to be origins of PA [4].
We report a rare case of PA arising from EAC.
An excisional biopsy specimen was received at pathology department from EAC of a 25-year-old female patient who presented with a painless mass of 01-year duration. Physical examination revealed a well delineated mobile firm mass at EAC. Preoperative radiologic, endoscopic and pathologic investigations were not done.
Grossly mass received at department of pathology was well circumscribed, 1.8 × 1.5 × 1 CMS with firm grey-white cut surface and had no skin lining.
Microscopy disclosed proliferation of tubulo-glandular structures lined by two-layers of epithelium in a chondromyxoid stroma. Cells lack pleomorphism, necrosis and prominent mitotic activity (Figure 1A and Figure 1B). With these findings a diagnosis of PA of EAC was made.
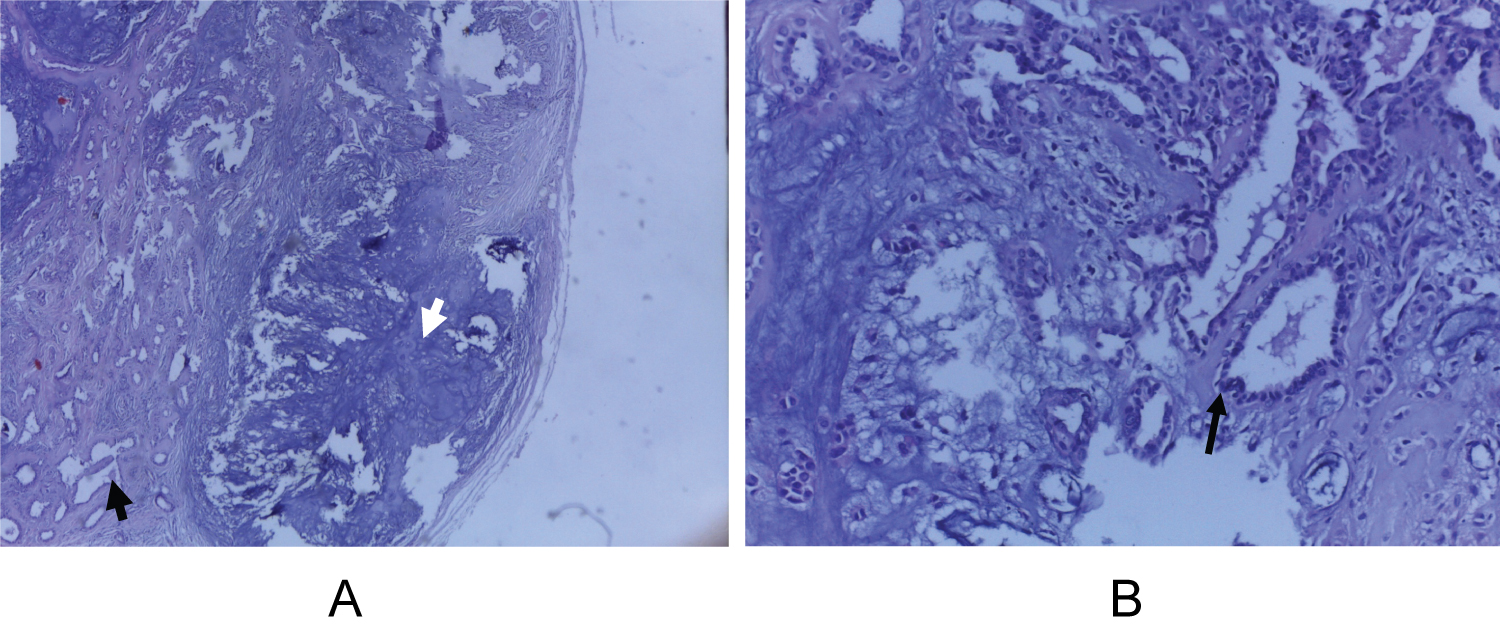 Figure 1: (A) Low power view showing circumscribed proliferation of tubule - glandular structures (black arrow) embedded in a chondromyxoid stroma (white arrow) (H & E, X40); (B) Higher magnification shows glandular structures lined by two layers of regular epithelial and myoepithelial cells without atypia. (Arrow) The hypocellular chondromyxoid stroma can be seen on the left side (H & E, X400).
View Figure 1
Figure 1: (A) Low power view showing circumscribed proliferation of tubule - glandular structures (black arrow) embedded in a chondromyxoid stroma (white arrow) (H & E, X40); (B) Higher magnification shows glandular structures lined by two layers of regular epithelial and myoepithelial cells without atypia. (Arrow) The hypocellular chondromyxoid stroma can be seen on the left side (H & E, X400).
View Figure 1
Patient was followed for 01 with no recurrent lesion.
PA is the most common benign tumor of salivary glands. Majority of cases arise from parotid gland. It is a slow growing tumor where identification of epithelial and myoepithelial/stromal components are essential for diagnosis. Surgical excision with sufficient margins is the standard mode of treatment with a recurrence rate of 1-5% [5,6].
Other possible sites of origin include nasal cavity, bronchus, skin, and soft tissues [1]. A much more rarer site is external auditory canal (EAC), first described in 1951 by Mark and Rothberg [2]. Since then, only 49 cases in 44 articles published in English language have been reported in the literature [3]. PA of t EAC belongs to a group of benign and malignant tumors derived from ceruminous glands [1].
World Health Organization recognizes 2 categories of ceruminous neoplasms: malignant and benign [7] (Table 1).
Table 1: Ceruminous gland neoplasms. View Table 1
Most patients with ceruminous gland neoplasms present with a mass and / or non-specific symptoms. Mass in EAC, fullness, hearing loss, pain and pruritus are most common symptoms in majority of benign tumors. Malignancies are characterized by pain, bleeding, otorrhea, mass and secondary otitis externa. As there are overlap in manifestations review of patient’s medical history; comprehensive physical examination (mainly to evaluate for extension from parotid); full otoscopic evaluation; radiologic evaluations (to determine extent of tumor, involvement of underlying bone and adjacent organs) are essential [4].
Benign Ceruminous Neoplasms account for 5.7% of all EAC and auricular tumors [4]. Tumors are well-circumscribed without destruction of surrounding structures. Imaging reveals a well-defined soft tissue lesion with homogeneous or rarely non-homogeneous enhancement with or without cystic changes [8].
Malignant ceruminous neoplasms are slightly more common than benign ones. Infiltration into surrounding tissue with destruction of osseous and cartilaginous structures is common. Imaging studies reveal heterogeneously enhancing tumor infiltrating and effacing the surrounding tissues.
Ceruminous pleomorphic adenoma (CPA) is the second most common benign neoplasm of the EAC. Progressively enlarging mass and pain are most common presenting symptoms. There is a slight male predominance (8:5) and mean age at presentation is 50.5 years [4].
Primary PA of the parotid could grow in to the EAC through the Foramen Huschke, invading the fallopian canal, cartilaginous fissures of Santorini and petrotympanic sutures. Therefore, parotid gland origin must be excluded. In magnetic resonance imaging, PA of the EAC have well-defined margins with hypo intensity on T1-weighted images and hyperintensity on T2-weighted images and Computed tomography imaging of cases shows no bony erosion [3].
Preoperative diagnosis of PA can be made by fine-needle aspiration cytology [9].
On excisional biopsy specimens, tumors are typically well circumscribed with firm grey-white cut surface. Histologically, there is haphazard proliferation of tubulo-glandular structures lined by two-layers of regular epithelium. Cells lack pleomorphism, necrosis and prominent mitotic activity. Background stroma is hypocellular myxochondroid [4].
Complete local excision with adequate margin of normal tissue, to prevent recurrence, and long-term follow-up are important in the management of PA of EAC [10].
PA of EAC is extremely rare and should be considered in differential diagnosis of a mass at EAC. Since majority of neoplasms at this site are malignant with overlapping manifestations with benign neoplasms; we recommend preoperative evaluations to include FNAC and imaging studies. Excision with a wide margin and long term follow up are necessary as recurrence and malignant transformation are possible.