Health Literacy (HL) is a multidimensional concept which core domains are: Health promotion, health care and disease prevention.
To describe the HL level of a group of diabetics and/or hypertensive patients from a northern region of Portugal; To verify the influence of sociodemographic variables and clinical variables on the HL level.
Descriptive-exploratory cross-sectional quantitative study. Sample of convenience n = 664 users enrolled in 3 groupings of health centers in the northern region of Portugal. A survey was used with the HL European Health Literacy Survey (HLS-EU-PT, translation valid for Portugal). Descriptive and inferential statistics techniques were used using IBM SPSS Statistics, software version 25. Ethical research principles were respected.
An inadequate or problematic level of HL was noted with adult/elderly users. From the dimensions studied, it was found that it is easier for users to take care of their health and more difficult to promote health. Sociodemographic and clinical variables influence HL levels. Seeing the doctor and the nurse are fundamental educators to increase the level of HL.
More information and more time in the medical and nursing consultations can ease the users' management of the therapeutical regime, improve the decision making for health promotion and disease prevention.
What is already known about the Topic?
• International data refer to a general level of problematic or inadequate HL, which includes Portugal. The most prevalent chronic non-communicable diseases are Diabetes and Hypertension.
• Portugal has the highest prevalence rate of diabetes in Europe and there are 3 million people with high blood pressure.
• The European Union stresses the promotion of health, disease prevention and the promotion of supportive environments for healthy lifestyles as a priority for the population. It is known that the HL level is an important variable in the health/disease process.
What this paper adds
• The evidence found partially responds to the National Program for Health, Literacy and Self-Care, referring to a micro context of the northern region of Portugal.
• There was an inadequate or problematic level of HL in patients with Diabetes and/or Hypertension. Users are more likely to take care of health and less likely to promote it.
• In users' opinion, doctors and nurses are fundamental educators to enable them to provide more and better information for the effective management of their health project.
• The results show a multidisciplinary investment in the three dimensions of HL, in order to effectively manage resources and increase health gains.
Health literacy, Diabetes mellitus, Hypertension, Primary health care, Portugal
Health Promotion (HP) contributes to the reduction of population diseases, especially when promoting healthy lifestyles. One of the HP strategies is health education. It aims at improving health, disease prevention, rehabilitation, transition or adaptation to a new condition of life. Health education empowers people to care for their health project, that is, to enable them to acquire the knowledge, skills and competencies to improve their quality of life and thus be responsible for their health and those around them [1].
Currently, chronic diseases are estimated as a growing public health problem because of the high mortality rates and disability they cause. According to the National Institute of Statistics (NIS), in Portugal it is estimated that 40.3% of the resident population, aged over 16 years, suffer from health problems or chronic diseases [2].
Chronic diseases, such as hypertension and Diabetes Mellitus (DM), are of increasing concern to health entities, both for their level of chronicity and for the wide range of effects they can have on people's daily lives [3].
Globally, it is estimated that more than 400 million adults have DM, with an expected growth estimate of more than 640 million adults by 2040 [4]. According to the World Health Organization (WHO), one in five adults worldwide has hypertension [5].
The Organization for Economic Co-operation and Development (OECD) says in its 2017 health report, Portugal is one of the countries with the highest prevalence of diabetes in Europe [4]. In parallel, in Portugal, there are 3 million people with AHT, that is, one in three [6].
Thus, chronic noncommunicable diseases such as hypertension and DM require the education and empowerment for people to achieve adequate control of the disease, to prevent complications and to take responsibility for the control of their health project and the groups where they are inserted [7].
To validate the above mentioned, the European Commission on Health Strategies points out as the fundamental principle in empowering citizens, the capacity they have for decision-making in their health project [8]. As demonstrated by the literature on the subject, the empowerment of each person to act to effectively manage health resources is directly related to the level of Health Literacy (HL).
HL is a multidimensional concept which core domains include: i) Health care; (ii) Disease prevention and (iii) Health promotion. The first domain, health care, is defined as the ability to process information about health problems, to understand medical information, to interpret it and to evaluate it in order to make decisions about it. The domain of disease prevention is understood as the ability to process information about health risk factors, in order to understand them, interpret them and evaluate information to make decisions that protect health. Finally, health promotion is related to the ability to identify health determinants in social and physical environments, to understand the influence of contextual variables on individual or family health, and how to act on them to reduce their harmful effects. The HL also integrates four levels of information processing with regard to decision making: access, comprehension, evaluation and utilization [9-11].
HL has been the object of study because of the preponderant role it plays in maintaining a person's health and quality of life, as well as in their ability to actively manage their health condition, allowing for greater interaction with health professionals [10,12,13]. Thus, HL has an impact on the management of individual and community resources, translating into health gains [13-15].
The level of HL is not a characteristic, but rather a state that partly reflects the experience of each person in their health/illness process [16]. The studies indicate that a person with a sufficient/excellent HL level is more likely to make clinical decisions in relation to the health of his/her family and the community where he/she is inserted. Research results show that people with higher levels of HL reduce health care costs, are more knowledgeable about health, use health services less frequently, and when hospitalizations occur, they are of shorter duration [10].
In contrast, low HL levels are associated with greater difficulty in managing their own heath, in understanding and following instructions from health professionals, and in perceiving information leaflets. As service users, people with low HL levels tend to seek health care less frequently for health promotion and disease prevention, and when hospitalizations occur, they are longer and usually have complications resulting from poor chronic conditions [3].
Thus, HL has gained increasing importance in the area of health education, especially in empowering people to manage their health and the resources they have access to [8,17-19], once it can contribute to the way people assimilate health knowledge and control the symptoms associated with their pathologies and contextual variables of the environment in which they live [20].
The scientific community has been awake to the monitoring of HL levels in different populations and contexts, in which a general level of problematic or inadequate HL stands out [11,21,22].
Because of the implications of different HL levels, there is a growing concern about this in the formulation of European health policies. This is supported by the European Union's strategic health plan, which aims to promote health, disease prevention and promotion of supportive environments for healthy lifestyles. According to the Despacho n.° 3618-A/2016 [23], it should be noted that in this strategy the operational objectives are to identify, disseminate and promote good evidence-based practice and good disease-prevention practice, as well as health promotion activities. In Portugal the Directorate-General for Health [12], proposed actions to promote HL as a measure of health promotion and disease prevention, particularly in chronic diseases and their associated risk factors.
Despite the importance of HL, information about its level in populations remains low. As such, in 2016, the low HL levels observed in Portugal led the Government to prioritize health promotion through a new ambition for public health, particularly through the creation of the National Program for Health Literacy and Self-Care [12,13].
Given the importance of the topic and the implications that the level of HL has for the effective management of the disease and, in particular, the chronic disease, we ask: What is the level of HL in people with diabetes mellitus and/or hypertension under treatment in Family Health Units from a region of Northern Portugal? This question was the subject of an investigation, the objectives of which were to describe the level of HL of a group of diabetics and/or hypertensives under treatment in a Family Health Unit of a Northern region of Portugal and to verify the influence of sociodemographic variables and clinical variables at the HL level of a group of diabetics and/or hypertensives.
A cross-sectional descriptive study was carried out. Data collection was conducted from February 2019 to May 2019 (authorization n°99/2018). A convenience sample (n = 664) was chosen as the result of data collection in three Health Center Groupings (ACES) of a region in the North of Portugal, with a total of 13842 subscribers. Inclusion criteria were defined as being diabetic, hypertensive or both, age equal to or older than 18 years, being enrolled in a Family Health Unit and attending the nursing consultation for diabetes or hypertension.
The data collection instrument was a questionnaire survey, divided into three groups, group I being composed of sociodemographic issues (gender, age, literacy, marital status and professional activity). Group II included the scale of the HL - European Health Literacy Survey [10,24], validated for the Portuguese reality [15]. The scale is composed of 47 items, which integrate the three dimensions: Health care, disease prevention and health promotion - dimensions assessed in questions 1-16, 17-31 and 32-47, respectively, [24]. The answers to each of the 47 items obey a Likert scale (1. very difficult, 2. difficult, 3. easy, 4. very easy, 5. do not know/no answer). The pre-assigned values for the scale assume a minimum value of zero and a maximum of 50, with increasing values of literacy. Levels of literacy can still be divided into categories, classified as inadequate, problematic, sufficient and excellent [25]. The formula for calculating the various HL levels was as follows:
Score = (average - 1) × (50/3).
Group III referred to the clinical variables (pathology, health services that have been used in the last 6 months and which health professional contributes to increase health knowledge), including an open question to request strategies to increase health literacy.
To collect the information, authorization was requested from the Ethics Committee of the Regional Health Administration of the North. Subsequently, a meeting was held with the coordinators of three groups of health centers (ACES), to present the project and request collaboration. At the time of the consultations, the users were invited to participate in the study, and a space with privacy for the collection of data was made available in each Family Health Unit (FHU). Ethical principles applied to human studies (the Helsinki Declaration) were respected and the informed consent form was applied. The anonymity and confidentiality of the data collected has been guaranteed and scrupulously respected.
In the overall characterization of the sample, the numerical variables were summarized through the mean and standard deviation (SD), and are presented in the text through the mean ± SD. Qualitative variables were used for absolute and relative frequencies. Mann-Whitney tests (HL comparison between two groups of subjects), ANOVA (comparison of HL between three or more groups of subjects) were used to verify the existence of relations between sociodemographic/clinical variables and HL. Pearson's correlation (relationship between age and HL). All test values of the tests (p-value) were considered statistically significant if they were less than 0.05. Statistical analysis was performed using IBM SPSS software version 25.
In the first place the results of the descriptive analysis are presented, and then the results obtained through the inferential analysis.
This study had the participation of 664 users, 47.7% male and 52.3% female, which translates into a very fair sample in terms of gender. As for the age, people aged 60 or older predominated, that is, the majority were adult users approaching the elderly age (61.6%). These users had low schooling (54.8% with only 4 years of compulsory education), were predominantly married (74.1%), mostly retired (56.8%), with only 30.9% of them professionally active.
From the general analysis of the scale used (HLS-EU-PT) it should be noted that the majority of users presented inadequate or problematic HL level (Graph 1).
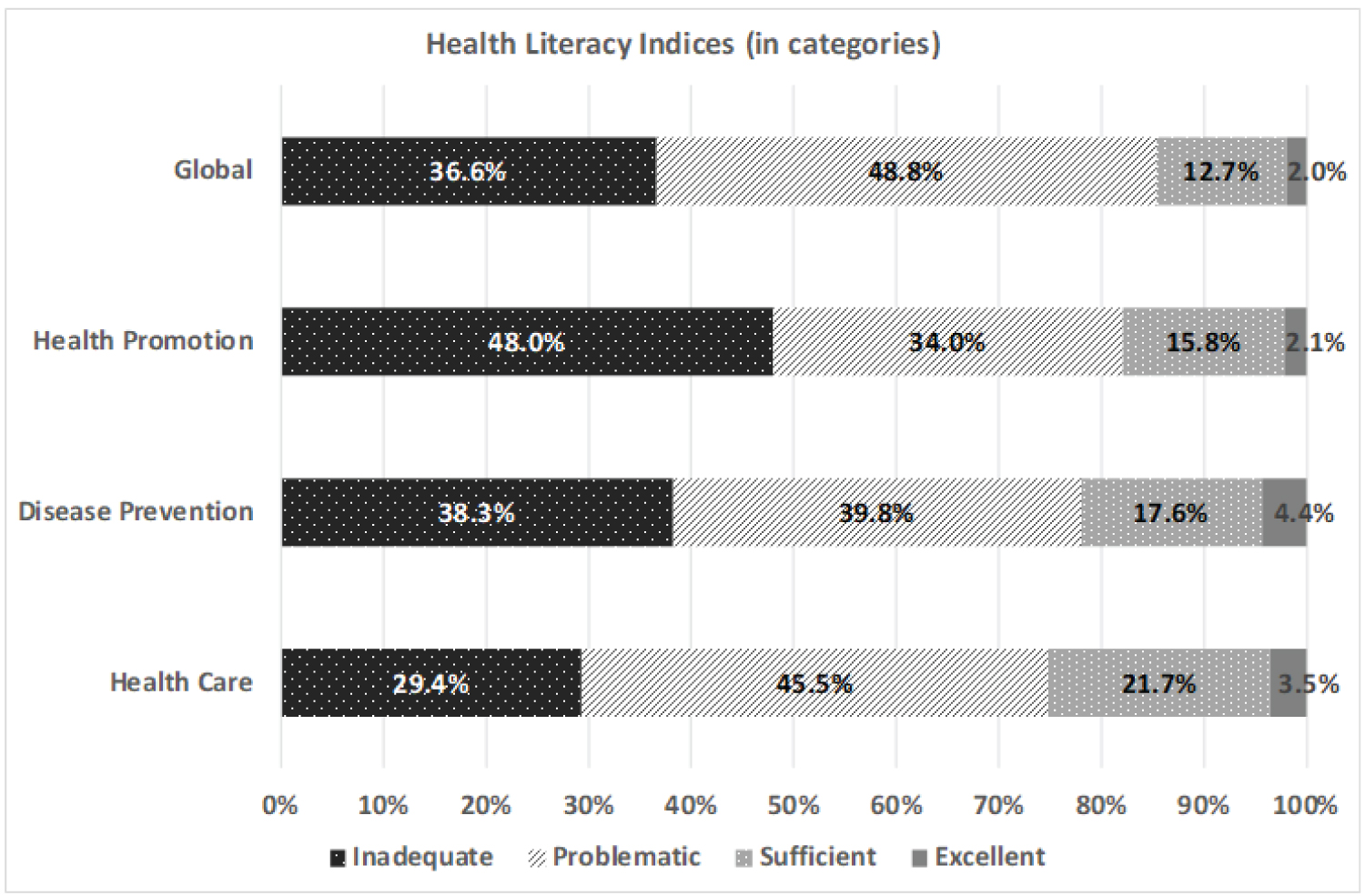 Graph 1: HL of a group of diabetic/hypertensive patients from a region in Northern Portugal (N = 664).
View Graph 1
Graph 1: HL of a group of diabetic/hypertensive patients from a region in Northern Portugal (N = 664).
View Graph 1
From the positioning of the answers it is verified that the users have HL levels in the middle of the scale of 0 to 50 points (mean of 26.56 and SD of 7.84): This means that 85.4% of respondents have a HL considered inadequate (0 to 25 points) or problematic (26 to 33 points). Of the three areas that make up the scale, health care was the most "positive" (it is easy for them to take care of health) and health promotion was the most "negative" (they have more difficulty in promoting health).
Data analysis (Table 1) shows that men have more HL than women, not only at the global level (averages of 27.33 vs. 25.86, respectively), but also in each of the 3 domains of the scale.
Table 1: HL vs. sex of a group of diabetic/hypertensive patients from a region in Northern Portugal (N = 664). View Table 1
It is also noted that the older the users are, the less HL they have (Table 2), but this correlation is weak (r = -0.448).
Table 2: HL vs. age of diabetic/hypertensive patients from a region in Northern Portugal (N = 664). View Table 2
By analyzing the data, it was also possible to verify (Table 3) that the higher the level of education the higher the level of HL, not only at the global level (increasing averages of 19.20 for people without studies, up to 33.35 for people with secondary education or higher), but as well as in each of the 3 domains of the scale.
Table 3: HL vs. qualifications of diabetic and/or hypertensive patients from a region in the north of Portugal (N = 664). View Table 3
Table 4 shows that the professionally active users have more HL than the inactive, not only at the global level (averages of 30.25 vs. 24.91, respectively), but also in each of the 3 domains of the scale.
Table 4: HL vs. professional situation of diabetic/hypertensive patients from a region in the north of Portugal (N = 664). View Table 4
Regarding the clinical variables, it was possible to verify that 50% of the users were diabetic, about 4 out of 5 respondents were hypertensive and about one third reported having the 2 pathologies at the same time. In addition to diabetes and/or hypertension, one-third of participants reported having other diseases. The majority of users use Family Health Units (86.3%), to the detriment of differentiated health care (30.1%) (This question allowed more than one answer).
The majority of respondents considered that both physicians and nurses contribute to their HL, with a higher prevalence for physicians 78.9% and 66.4% referred nurses (this question allowed for more than one response).
When asked to suggest measures that could increase their HL, only 1 in 5 respondents answered, of which almost half reported the dissemination of more health information and a quarter suggested that health professionals should devote more time to informing users.
In this study, which had the collaboration of a group of users enrolled in three ACES, the sample was characterized by its homogeneity with regard to sex, adult users approaching the elderly, mostly retired and with low levels of schooling. They were diabetic or hypertensive and some even carry other pathologies. Most have turned to primary health care (FHU) for monitoring and follow-up of their disease.
Based on the objectives of this investigation, it was verified that a group of diabetic and/or hypertensive patients under treatment in three Family Health Units of a region in the North of Portugal presented an inadequate or problematic level of HL. These results are corroborated by several national and international studies [15,22,26-31].
The agreement of the results of this study with the remaining empirical evidence reinforces the need for health professionals to be aware of the importance of HL because, as Osborn [32], mentions, people with low HL tend to have more complications resulting from poor chronic diseases of which they are carriers, namely hypertension and DM. With such limited levels of HL, it is crucial that health professionals, health agencies, government and society in general invest in health education for the population in the various domains, enabling them to effectively manage their health [22].
Particularly for the three domains that make up the HL scale, the health care dimension was the one with the highest results, with health promotion having the lowest levels. These results are also in agreement with the other studies, namely the study carried out by Espanha, Avila and Mendes [28].
It is highlighted in this study that the sociodemographic variables influence the users' HL levels. Male participants were at a higher HL level, which is in line with the study by Saboga-Nunes, Sorensen, Rodrigues [30]. However, other studies point out that there is no relationship between the sex variable and the HL level [28,33].
It was verified that, the more education the users have, the higher the HL level is. According to Pedro, Amaral, Escoval [15] there is a relationship between the level of schooling and the HL level, which is corroborated by authors such as Gonçalves [34], Espanha, Avila, & Mendes [28]. Low schooling according to Margoto, Colombo, Gallani [35] is considered a risk factor that could trigger a greater number of hospitalizations, due to an increase in the incidence of chronic disease exacerbations. Thus, the higher the level of schooling, the better the ability to understand and adhere to the therapeutic regime [26].
In the relationship between the age variable and the HL level, it was found that adults have more HL than the elderly. This evidence has already been reported in several studies, notably by Davey [33], as one of the main influencers of the HL level of populations worldwide. Pedro, Amaral, Escoval [15] report that as the age increases, the level of health literacy tends to decrease. This seems to be a factor of agreement and risk in HL, since several authors point out the elderly as the most vulnerable group [22,28,30].
It should be noted that the professionally active users had higher HL levels when compared to the retired ones. In 2016, a group of researchers reached similar results to those found in the present study [28], indicating that people who were employed presented better levels of HL compared to the rest [15,22,30].
This trend of outcome may be related to the fact that active people interact with colleagues and other social agents, which may contribute to the increase in the level of HL.
It was explicit that users perceive the doctor and the nurse as fundamental educators to increase their level of HL. They were of the opinion that these professionals should provide more information to guide them in their health project and they would like these professionals to make more time available in the consultations.
There are limitations to our study that warrant further discussion. Firstly, the fact that data were collected from a sample living in a specific region with a small representation of the population. However, it should be noted that these data can provide a significant contribution to the (re)definition of the HL promotion strategies on in the region where the study was conducted. Considering the specific characteristics of this study, the results answered the research question, identifying a predominance of an inadequate or problematic HL level.
The results presented here refer to an operational strategy to identify the HL level of a group of users from a specific region of northern Portugal. It responds to a topic from the European Union's strategic health plan and the National Health, Literacy and Self-Care program. The evidence found represents a further set of indicators for the multidisciplinary team of health professionals, especially in the Family Health Units, to have these values as a reference in planning the activities and outlining strategies to improve their users' HL levels. We suggest a multidisciplinary investment in the three dimensions of HL, in order to effectively manage resources and increase health gains.
This research did not receive any specific Grant from funding agencies in the public, commercial or not-for-profit sectors.
None to declare.
The authors would like to thank all the participants, the entire team of professionals and the three clusters of healthcare centers where the data was collected, for the opportunity.