Odontogenic cysts and tumors located in the upper jaw are infrequent and when they grow up can cause bone destruction. The histologies of odontogenic cysts and tumors are diverse and the treatment is surgical. Different surgical approaches have been described to be able to perform complete exeresis of these lesions, based mainly on obtaining adequate exposure.
Endonasal surgery with endoscopes has undergone constant evolution and different extended approaches to the maxillary sinus have been described, making it possible to resect cysts and odontogenic tumors with good vision and less morbidity.
Three patients were treated for a keratocyst, a dentigerous cyst, and an ameloblastoma of the maxillary sinus that caused bone destruction of two or more walls, using an endonasal approach with endoscopes alone or combined with an anterior maxillary sinusotomy.
The resections were complete, no recurrences were detected during follow-up, and there were no complications.
Odontogenic cysts, Ameloblastoma, Maxillary sinus, Endoscopic surgery
Odontogenic cysts and tumors located in the upper jaw are infrequent [1].
As they grow within the sinus, they can produce late signs and symptoms such as headache, nasal obstruction and facial deformity, and can erode the bony walls of the maxillary sinus.
Cysts can be inflammatory or originate from alterations in the development of the epithelium that forms the teeth, which may be included within the bone or mucosa.
Tumors can have different histologies, with ameloblastoma being the second most frequent after odontoma [1].
The treatment is surgical, and the techniques used may be different, depending on the aggressiveness (histology), location and size of the lesions and the experience of the team in external and endonasal surgery.
Endoscopic endonasal surgery has had a significant evolution and the description of different extended approaches to the maxillary sinus has improved and facilitated the resection of these tumors by an endonasal approach alone or combining this technique with an anterior maxillary sinusotomy.
To determine the efficacy of the endonasal approach with endoscopes alone or in combination with anterior maxillary sinusotomy to completely remove odontogenic cysts and tumors with destruction of the bony walls of the maxilla.
Descriptive and retrospective.
The electronic medical records of all patients who were treated by an endonasal approach alone or combined with an anterior sinusotomy due to odontogenic cysts or odontogenic tumors with destruction of two or more walls of the maxillary sinus, between July 2015 and August 2022 were reviewed and analyzed.
Two patients with odontogenic cysts who did not have destruction of the bony walls of the maxillary sinus and who underwent endonasal surgery were excluded.
All patients were evaluated by nasal endoscopy, computed tomography (CT), and contrast-enhanced magnetic resonance imaging (MRI).
A previous biopsy was performed in one patient under general anesthesia.
The surgeries were performed under general anesthesia and the patients were hospitalized for 24 hours.
Endoscopes of 0 and 30 degrees and conventional instruments for endoscopic rhinosinusal surgery were used.
The endonasal surgical approaches consisted of performing a medial maxillary mega-antrostomy (preserving the nasolacrimal sac and duct), a medial and inferior maxillary mega-antrostomy, and a medial maxillary mega-antrostomy plus a prelacrimal approach. Endonasal surgery was combined with an anterior maxillary sinusotomy in some patients.
At the end of the surgery was placed hemostatic matrix in the nasal cavity.
The controls were made by nasal endoscopy and computed tomography.
The surgical approach was considered effective when it allowed adequate exposure and complete resection of the lesion, and the surgery had a low incidence of complications.
Three patients were treated for odontogenic cysts and tumors that had destruction of the bony walls of the maxillary sinus.
All three were men and the mean age was 24 years (12-45).
The histologies were: Dentigerous cyst, keratocyst and ameloblastoma. All the lesions were in the left maxillary sinus, and the reasons for consultation were facial tumor in two and headache in another.
The presence of bony destruction of the walls of the maxillary sinus, and the presence of a dental piece inside the lesions in the three patients were diagnosed by tomography.
In two patients, a medial maxillary mega-antrostomy was performed through the endonasal approach combined with an anterior maxillary sinusotomy through the sublabial approach. In one of them, a lower maxillary antrostomy was also performed (Figure 1 and Figure 2).
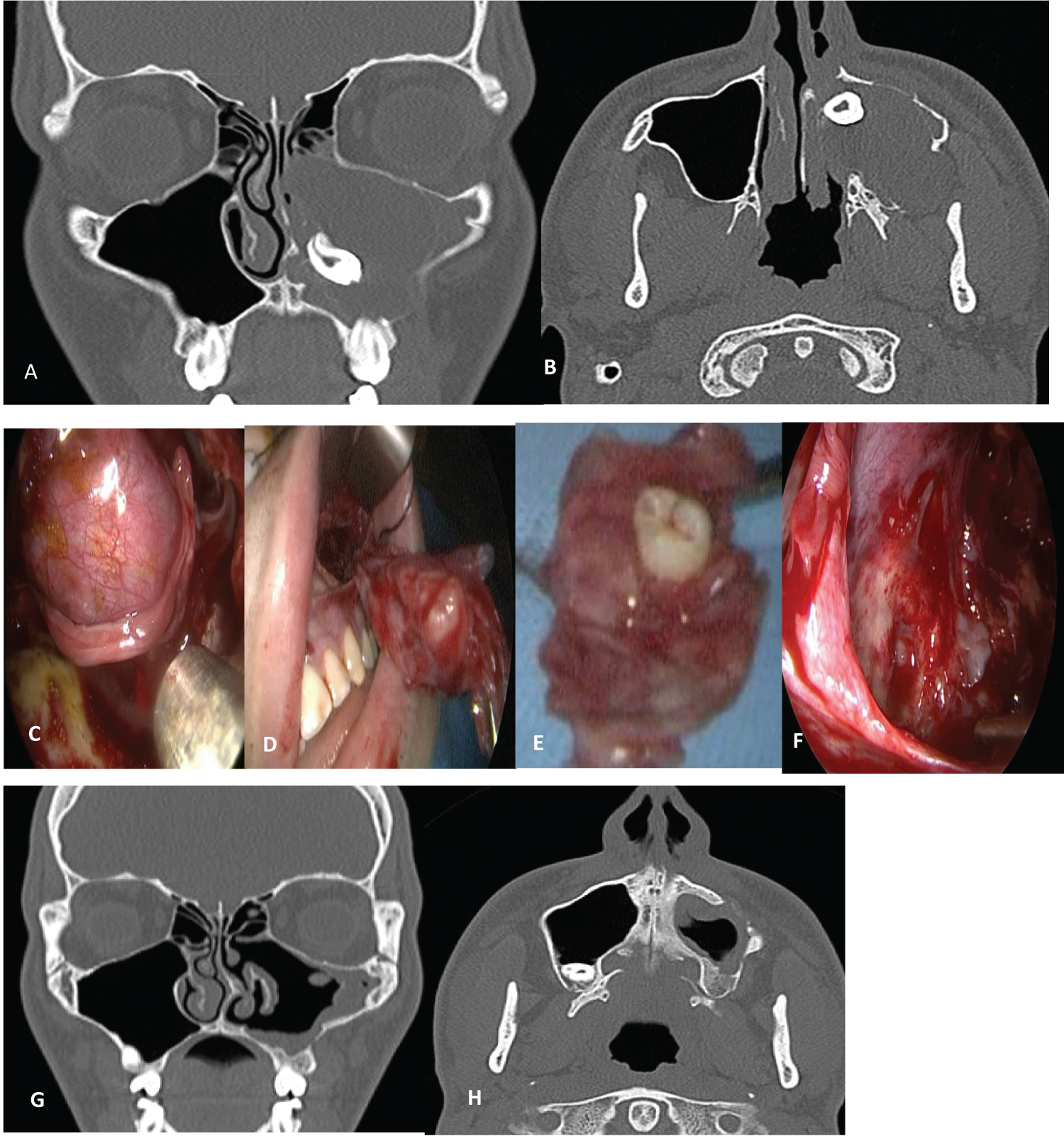 Figure 1: Keratocyst: A) Computed tomography showing the destruction of the medial and posterior wall of the maxillary sinus with extension of the cyst to the nasal cavity and pterygomaxillary fossa; B) Computed tomography showing the destruction of the medial and posterior wall of the maxillary sinus with extension of the cyst to the nasal cavity and pterygomaxillary fossa; C) Combined surgical approach: View through the anterior maxillary sinusotomy; D) Cyst resection; E) Tooth included; F) Endonasal view with an endoscope of the medial maxillary mega-antrostomy; G) Postoperative computed tomography - coronal; H) Postoperative computed tomography - Axial.
View Figure 1
Figure 1: Keratocyst: A) Computed tomography showing the destruction of the medial and posterior wall of the maxillary sinus with extension of the cyst to the nasal cavity and pterygomaxillary fossa; B) Computed tomography showing the destruction of the medial and posterior wall of the maxillary sinus with extension of the cyst to the nasal cavity and pterygomaxillary fossa; C) Combined surgical approach: View through the anterior maxillary sinusotomy; D) Cyst resection; E) Tooth included; F) Endonasal view with an endoscope of the medial maxillary mega-antrostomy; G) Postoperative computed tomography - coronal; H) Postoperative computed tomography - Axial.
View Figure 1
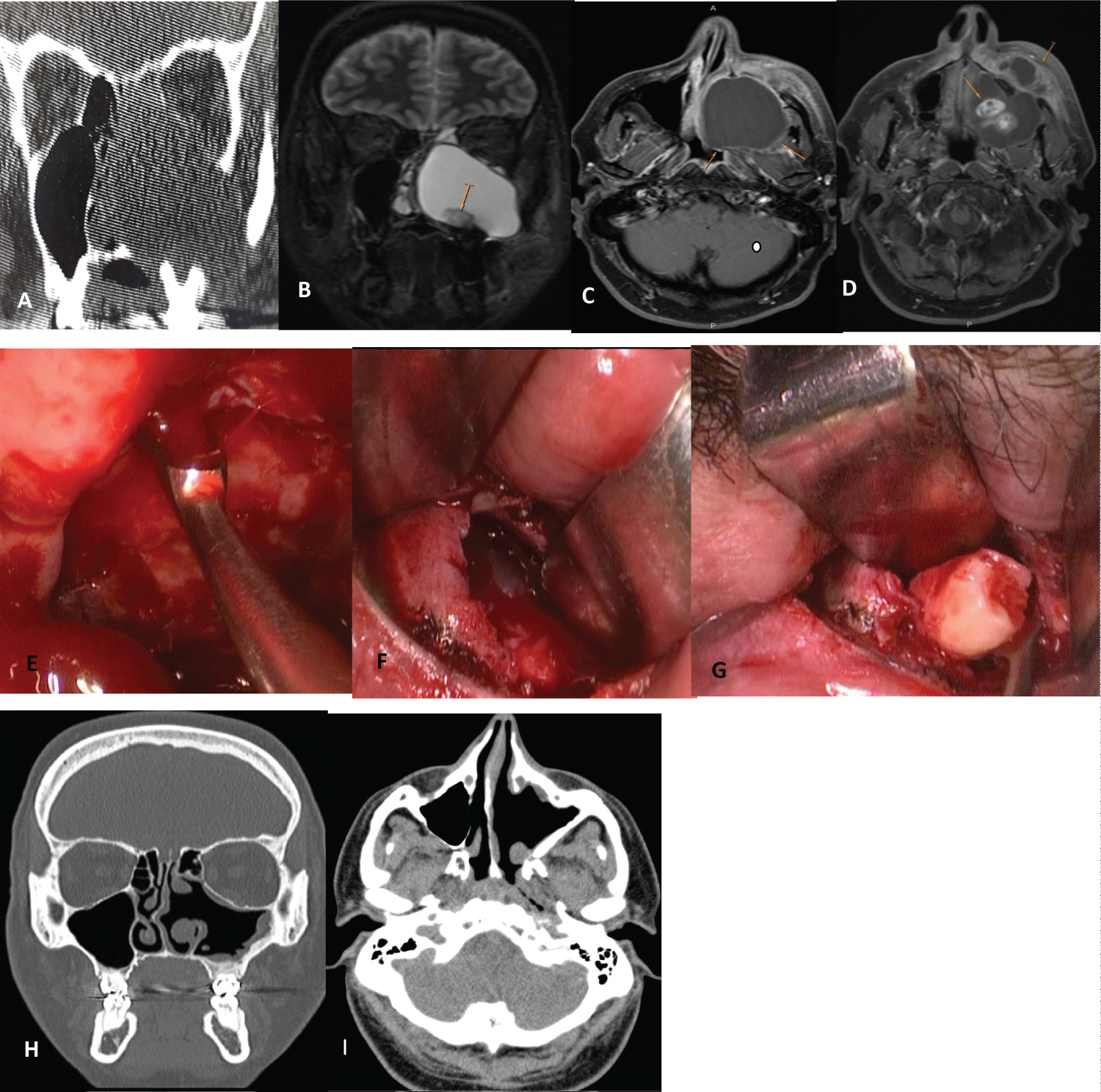 Figure 2: Unicystic ameloblastoma: A) CT showing destruction of all the bony walls of the maxillary sinus; B,C,D) MRI showing the extension of the tumor to the nasal cavity, pterygomaxillary fossa, infratemporal fossa with dental piece included; Combined surgical approach: E) Endonasal view with an endoscope through the middle and lower maxillary mega-antrostomy (curette resection of the tumor adhered to the periorbita); F,G) Anterior maxillary sinusotomy showing the resection of the tumor with the tooth; H, I) Postoperative coronal and axial computed tomography 6 years after surgery with no evidence of tumor persistence.
View Figure 2
Figure 2: Unicystic ameloblastoma: A) CT showing destruction of all the bony walls of the maxillary sinus; B,C,D) MRI showing the extension of the tumor to the nasal cavity, pterygomaxillary fossa, infratemporal fossa with dental piece included; Combined surgical approach: E) Endonasal view with an endoscope through the middle and lower maxillary mega-antrostomy (curette resection of the tumor adhered to the periorbita); F,G) Anterior maxillary sinusotomy showing the resection of the tumor with the tooth; H, I) Postoperative coronal and axial computed tomography 6 years after surgery with no evidence of tumor persistence.
View Figure 2
In another patient, a medial maxillary mega-antrostomy was combined with an endonasal prelacrimal approach (Figure 3).
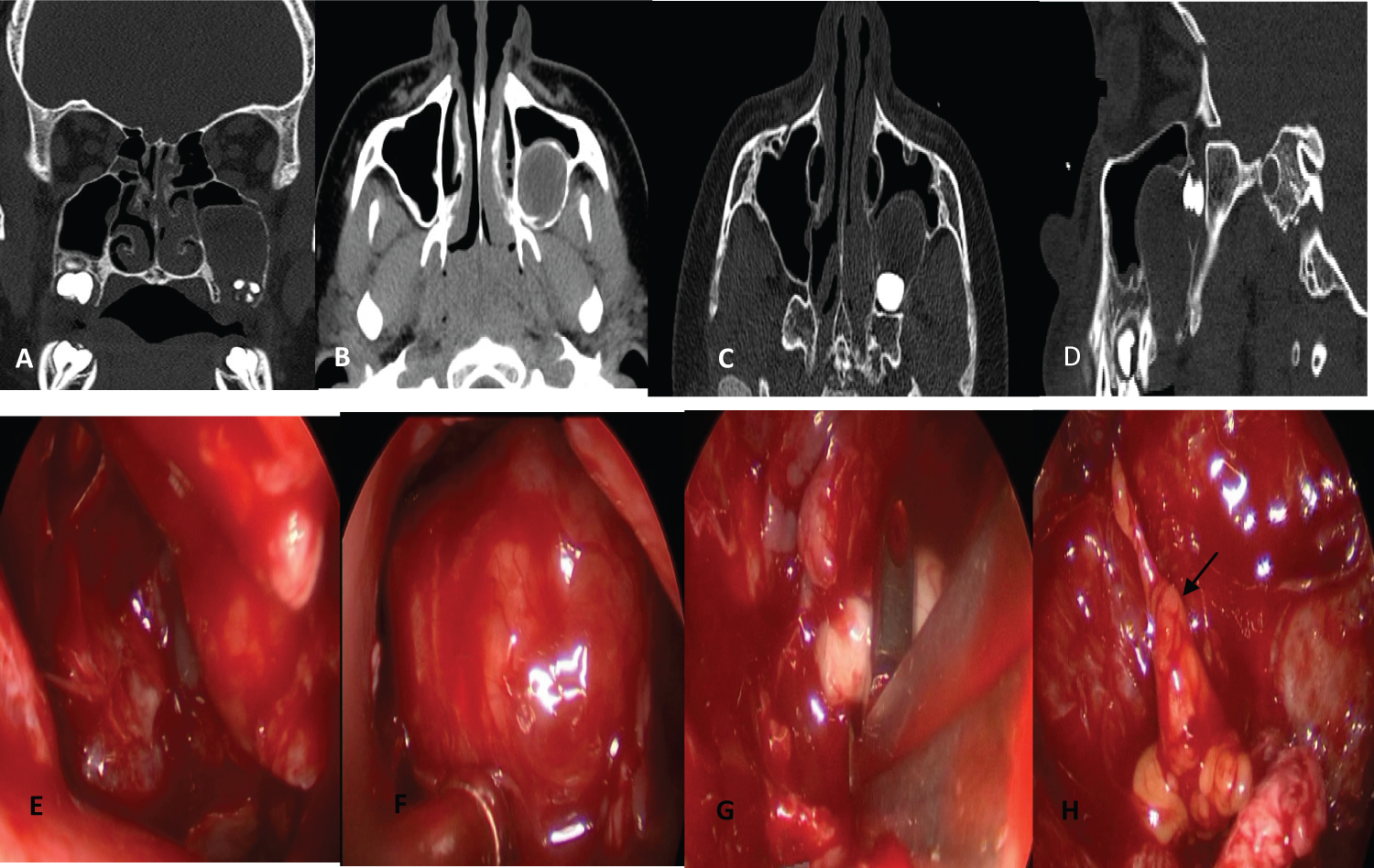 Figure 3: Dentigerous cyst: A, B, C, D) Computed tomography where the destruction of the inferior and posterior wall of the maxillary sinus with the inclusion of the dental piece is observed. Endonasal resection of the cyst with an endoscope, through a median mega-antrostomy and a prelacrimal approach to the upper jaw; E, F) view of the tumor through the prelacrimal access; G) Resection of the cyst and the tooth included through a median mega-antrostomy; H) Fat extruded from the pterygomaxillary fossa after resection (black arrow). With these approaches, a very good exposure of the tumors within the maxillary sinus was obtained and complete resections were possible.
View Figure 3
Figure 3: Dentigerous cyst: A, B, C, D) Computed tomography where the destruction of the inferior and posterior wall of the maxillary sinus with the inclusion of the dental piece is observed. Endonasal resection of the cyst with an endoscope, through a median mega-antrostomy and a prelacrimal approach to the upper jaw; E, F) view of the tumor through the prelacrimal access; G) Resection of the cyst and the tooth included through a median mega-antrostomy; H) Fat extruded from the pterygomaxillary fossa after resection (black arrow). With these approaches, a very good exposure of the tumors within the maxillary sinus was obtained and complete resections were possible.
View Figure 3
Buccomaxillary fistulas did not occur and the teeth adjacent to the lesions could be preserved. We had no complications, and the hospitalization was in all 24 hours. In the controls carried out with nasal endoscopy and CT no recurrences were found. Follow-up was 7 and 6 years in two patients and 5 months in another (Table 1).
Table 1: Patients treated by an endonasal approach alone or combined with maxillary anterior sinusotomy for odontogenic cysts or tumors. View Table 1
Odontogenic cysts can be inflammatory, such as radicular cysts that originate from Malassez remnants in the periodontal ligament, or they can be produced from remnants of dental pieces due to developmental alterations. Dentigerous cysts originate in the odontogenic epithelium associated with the crown of an included tooth, and keratocysts originate from remnants of the dental lamina [2].
In a study carried out in Canada [3] they determined that the most frequent cysts were radicular (65.15%), followed by dentigerous (24.08%) and then by keratocysts (4.88%).
Ameloblastoma is a benign, aggressive tumor that originates from the epithelium of the dental lamina. It represents 1% of oral tumors and 10% of odontogenic tumors and is more frequently located in the mandible (80%) than in the maxilla (20%) [4].
The treatment of these lesions is surgical resection.
The surgical approach can be endonasal with endoscopes, and the techniques to access the maxillary sinus through its medial wall can be diverse: Medial antrostomy, medial mega-antrostomy, medial and inferior antrostomy, medial maxillectomy, endoscopic Denker and prelacrimal access. The traditional external approach has been the anterior sublabial maxillary sinusotomy, which can be combined with the endonasal approach.
In dentigerous cysts, complete resections of the cyst with its capsule and the included tooth or marsupialization are the recommended techniques.
We prefer to perform complete resection, especially in giant cysts with destruction of the bony walls of the maxillary sinus.
In a patient with a dentigerous cyst that caused destruction of the posterior and inferior wall of the maxilla, we had an excellent view of the lesion through a wide medial antrostomy and a prelacrimal access. We were able to completely remove the cyst without the need to combine the endonasal approach with an external maxillary sinusotomy.
The use of prelacrimal access combined with a medial antrostomy is possibly the endonasal technique of choice to expose and completely remove these lesions.
We used this combination only in this case, since before 2019 we did not perform the prelacrimal endonasal approach.
Keratocysts have a greater possibility of recurrence, so complete resection of the cyst with a peripheral bone sector is advisable [5]. This could be done endonasally using a drill and drilling through the medial maxillary antrostomy or through the prelacrimal access. Others apply a solution to remove any epithelial remnants of the keratocyst that could persist after resection (Carnoy's solution consisting of 60 ml of ethanol, 30 ml of chloroform, 10 ml of glacial acetic acid and 1g of ferric chloride) [6].
In one of the patients described with a giant keratocyst that caused the destruction of the medial, anterior, and posterior bony walls of the maxillary sinus, we performed a wide medial and inferior maxillary antrostomy and combined it with an anterior sinusotomy to completely resect the lesion.
The diagnosis of keratocyst was made by the deferred histopathological study of the piece of surgical resection. We resected the adjacent bone, peripheral to the cyst with curettes.
In a systematic review of the literature, they identified 16 case series that included 45 patients with odontogenic cysts who were treated surgically using endonasal techniques with endoscopes. Sixteen were radicular cysts, 10 dentigerous cysts and 12 keratocysts. They reported no recurrences or serious complications with a mean follow-up of 29 months [7].
In another study they reported the results of the treatment of 30 patients with odontogenic cysts located in the maxillary sinus (11 had radicular cysts, 11 dentigerous cysts, 7 keratocysts and one had a glandular cyst). Sixteen were treated endonasally only, and 14 using an endonasal approach and maxillary anterior sinusotomy.
Twenty-two had large cysts, and the resection was complete in 20.
A keratocyst recurrence occurred during the mean follow-up of 31 months and no complications were reported [8].
The usual treatment of ameloblastoma is complete surgical resection with free margins by partial or total maxillectomy with reconstruction [9].
Endonasal surgery may be indicated in selected patients with unicystic ameloblastomas of the luminal or intraluminal type. In those with mural compromise, maxillectomy with a margin of 1 to 2 cm is advisable [10].
In the patient we treated for an ameloblastoma of the maxillary sinus, the previous biopsy was reported as an epithelial cyst without atypia, and the deferred histopathological study of the surgical resection performed through the endonasal route and by anterior maxillary sinusotomy diagnosed a unicystic ameloblastoma.
Some studies [4,11] report case series of selected patients with ameloblastomas of the maxillary sinus successfully treated by endonasal approaches alone or combined with anterior sinusotomy (Figure 4).
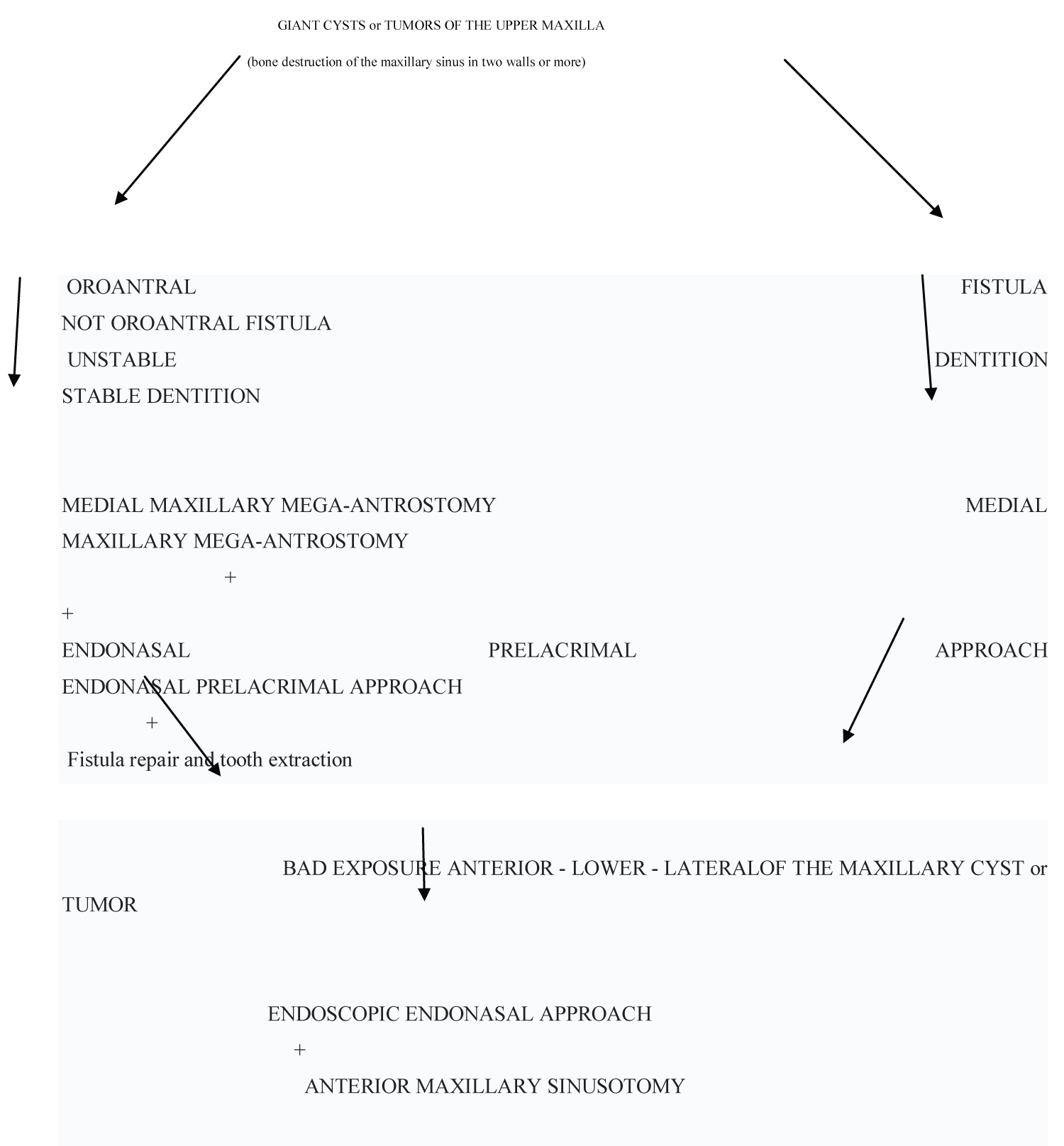 Figure 4: Surgical treatment algorithm for odontogenic cysts and tumors of the maxillary sinus.
View Figure 4
Figure 4: Surgical treatment algorithm for odontogenic cysts and tumors of the maxillary sinus.
View Figure 4
The endonasal approach with endoscopes through a wide medial maxillary antrostomy, combined with a prelacrimal approach or anterior maxillary sinusotomy was very effective to expose adequately and completely remove odontogenic cysts and tumors.
The prelacrimal endonasal access allows an adequate visualization of the anterior, lateral, and inferior sector of the maxillary sinus and allows drilling of the bone if necessary.
None.