A survey was conducted of practicing oral and maxillofacial surgeons with double degrees, a Doctor of Dental Surgery or Doctor of Dental Medicine, (DDS/DMD) and Doctor of Medicine or Doctor of Osteopathic Medicine (MD/DO). These responding dual degree, oral and maxillofacial surgeons were all current members of the American College of Oral and Maxillofacial Surgeons (ACOMS). The survey consisted of seven questions; such as, was their medical degree obtained in a combined MD/oral and maxillofacial surgery residency program, were they practicing under their dental license, medical license or both, if they felt their dual degree status enhanced their referrals, income, patient's confidence, do they feel that their dual degree status gave them an advantage over single degree oral and maxillofacial surgeons, and if they had it to do over, would they pursue the dual degree pathway again. The results were that if these oral and maxillofacial surgeons had it to do over again the majority would make the same choice again.
Until 1930, Oral and Maxillofacial (OMS) training typically consisted of a 1-year internship followed by a year of didactic coursework in anatomy and physiology at a different institution [1]. In 1967, this training evolved into a 3-years integrated program wherein the first year remained an internship, and the second year included coursework in medicine, anesthesia, surgery, and an elective (3 months each). OMS Residency was performed in the final year [1,2].
The first dual-degree (DD) OMS training program in the US was established in 1971 at Massachusetts General Hospital and Harvard [2,3]. In the subsequent 5 decades, this model has expanded to 46 DD programs, nearly half of the 100 accredited OMS training programs in the United States [4,5]. Another type of dual degree OMS training program was recently established at the University of Rochester [6] which an integrated Executive MBA degree/OMS Certificate program provides a pathway to earn a degree in finance during residency.
With nearly half of the OMS training programs requiring 2+ years of medical school and 4 years of OMS training after 4 years of undergraduate education, and 4-years of dental school the decision to choose between a single degree (SD) or DD residency program can be difficult [5].
Reasons for seeking a DD OMS training can vary among those particular candidates [7-9] For some, the decision to pursue dual degree, MD OMS training stems from a desire to become involved in OMS hospital or academic administration and/or leadership positions within the OMS specialty [2,5,6,9] A recent survey of academic plastic surgeons found that those who had DDs, were almost twice as likely to hold academic or society leadership roles [9]. The current listing by the American Association of Oral and Maxillofacial Surgeons of accredited OMS training programs showed that of 100 chairman and program director positions, 45 department chairman and 46 program directors were held by DD professionals [5,9,10]. The numbers of DD OMS in leadership roles should only grow with the increase in dual degree OMS training programs [5,9,10].
Department chairs, and academic deans must lead organizations that thrive not only in academics but finances and financial production [6]. The addition of a MD degree does not specifically address this aspect of administrative responsibilities in these leadership positions [6] An MBA may be a better "second" degree. The University of Rochester recently started an option for those interested in OMS leadership positions, the opportunity to participate in a combined integrated program with the business school to complete an executive MBA while completing their OMS training [6].
Given the growth of DD OMS programs, the time since these programs first appeared (55 years ago) that the initial DD OMS survey completed 33 years ago [2,7] it is an ideal time to survey DD practitioners to see if they agree with their decision to pursue DD OMS training. This survey was developed to capture the perspective of practicing DD OMS related to whether the additional financial and time commitment of a DD program was justified by the professional benefits those degrees engendered. This information is particularly relevant to young professionals who are applying to OMS residency programs and must decide between 4-year, single-degree programs and 6-year, MD integrated, OMS residency programs.
Redcap survey resource was used to create a survey consisting of 7 questions regarding the DD surgeon's education and perceived value of pursuing additional medical training (Table 1). 2513 emails listed with the American College of Oral and Maxillofacial Surgeons received information regarding this survey. Only recipients that received dual-degree training in OMS were invited to participate and were electronically consented to do so. This process eliminated SD surgeons from participating in this study.
Table 1: Questionnaire dual degree oral and maxillofacial surgeon's participants completed. View Table 1
Of the 2513 survey requests, 223 individuals consented to participate. Fifty-seven additional surveys were removed due to having completion rates of less than 10%. Data were evaluated on the remaining 166 surveys.
The overwhelming majority (82%) of respondents received their DD status through combined OMFS/MD programs, followed by those who received it after (11%), or prior to residency (2%). The majority (73%) reported receiving both degrees from the same institution, followed by unaffiliated (17%) and affiliated institutions (15%). When asked to report their current licensure, the majority were practicing under both a dental and medical license (Figure 1).
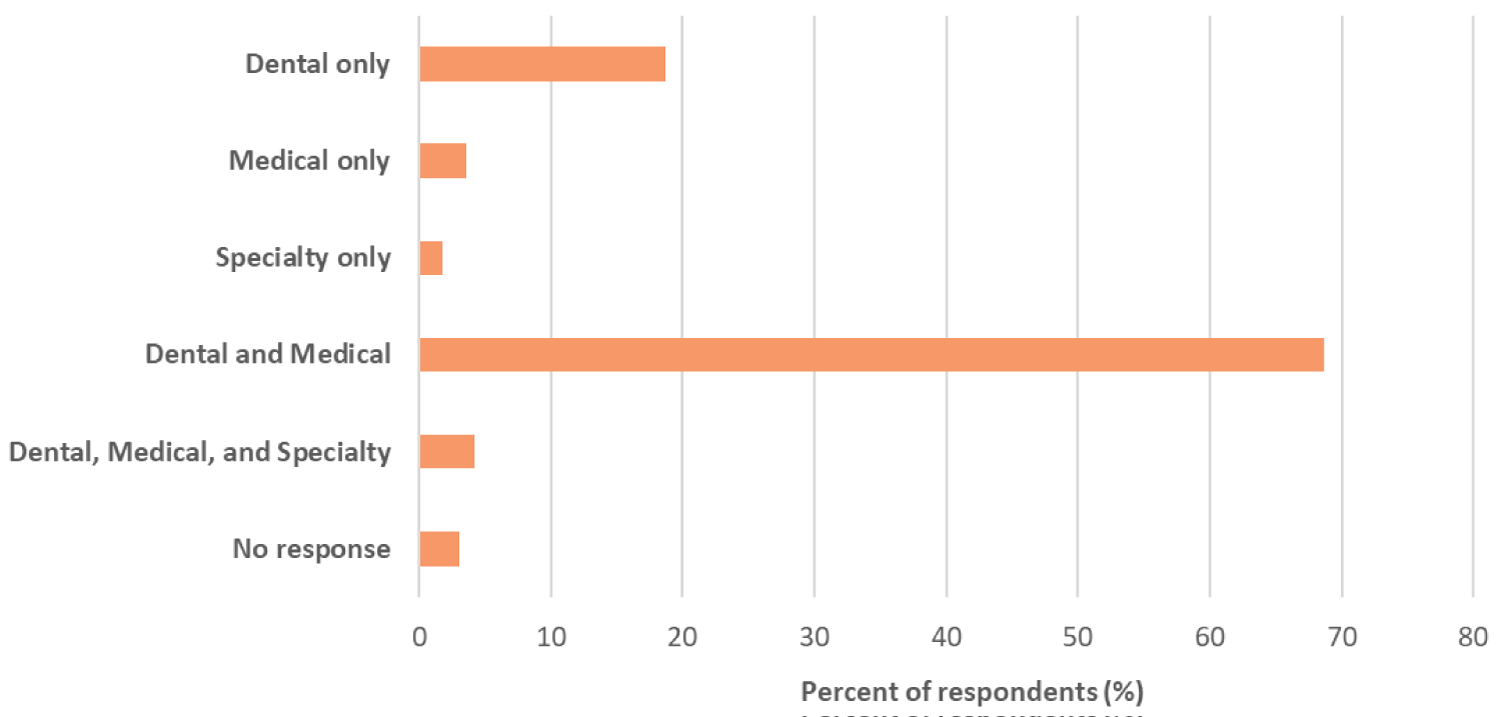 Figure 1: Types of licenses under which respondents are practicing at the time of survey.
View Figure 1
Figure 1: Types of licenses under which respondents are practicing at the time of survey.
View Figure 1
Only 27.7% of respondents reporting feeling that their DD status enhanced their income potential. However, a strong majority (67.5%) reported feeling it still gave them an advantage compared to those graduating from SD OMFS programs, and if given the choice, 87.4% of respondents would again participate in another DD program (Figure 2).
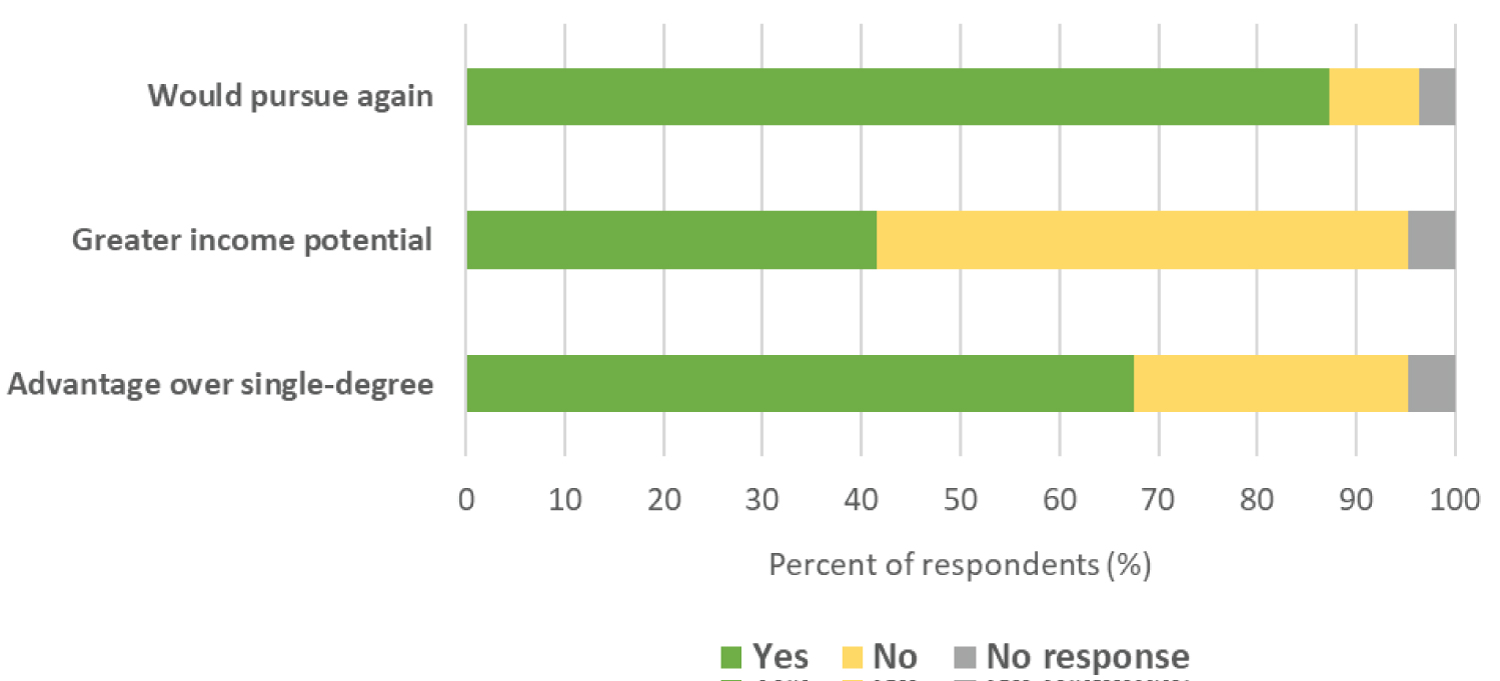 Figure 2: The response rate for survey items "Do you feel that your dual degree training gives you an advantage over single degree OMFS" (bottom), "Do you feel that your dual degree status has enhanced your income potential (middle), and "If you had to do it over, would you pursue the dual degree pathway again?"
View Figure 2
Figure 2: The response rate for survey items "Do you feel that your dual degree training gives you an advantage over single degree OMFS" (bottom), "Do you feel that your dual degree status has enhanced your income potential (middle), and "If you had to do it over, would you pursue the dual degree pathway again?"
View Figure 2
When queried on several specific ways that having a DD might enhance the practitioner's job experience, increased patient confidence was reported as the largest benefit (75.9% of respondents). Enhanced ability to treat patients and obtaining medical referrals were also seen as a benefit by the majority (68.1% and 62.1%, respectively) of participants. Half of respondents did not feel that having a dual degree benefited hospital privileges, and less than reported a benefit for dental referrals (Figure 3).
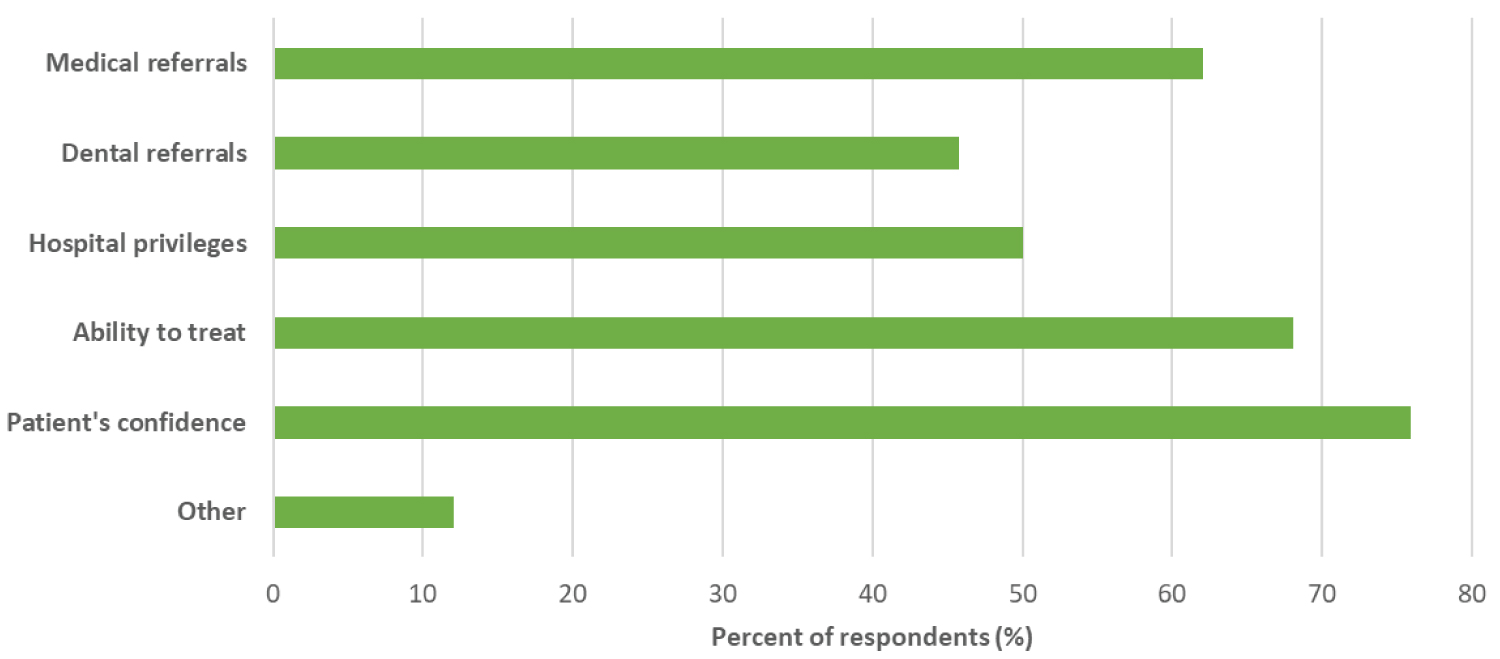 Figure 3: Participant views on different ways in which a dual degree enhanced their ability to practice.
View Figure 3
Figure 3: Participant views on different ways in which a dual degree enhanced their ability to practice.
View Figure 3
An overwhelming number of respondents (87.4%) felt that if they had it to do over again, would again do the DD OMS training option (Figure 2). This is consistent with the prior survey performed by Barber and Sejud (1988), who found that the most respondents would choose to attend a DD program again. This was true even when considering the greater financial expenditure required for dental and medical school [2,7]. Taken together, these two surveys indicate generally strong agreement that the time and financial commitments of an additional 2-3 years of medical school was beneficial. This is despite very few (27.7%) of new survey participants feeling that their DD status conferred a greater income potential. Looking at other specific comparisons of this study to the original Barber study these stand out; referrals from both the medical and dental communities, overall ability to treat patients, and hospital privileges, were positive factors, but to a lesser degree when compared to the previous survey (Figure 3).
There are two interesting results of our survey that require further investigation. Nearly one-third (32.5%) of our sample did not feel that their DD gave them an advantage over their SD colleagues, and that a minority (27.7%) feel that their DD enhanced their income potential. While salary data are difficult to capture, we did find one website that lists the starting salary for a SD and DD OMS. Physician Thrive, physician planning company (physicianthrive.com, May 2022) reports the starting salary for a SD OMS at $225,000 and for a DD OMS at $240,000, only a $15,000 difference [11]. This may support the fact that our sample did not feel the DD enhanced their income potential. Also, if we look at the response regarding whether they felt they had an advantage over SD OMS, those results could also be related to the minimal financial advantage noted between the DD OMS and SD OMS.
The DD OMS did report that their status did enhance the confidence that their patients had in them. This could be related to the patient's confidence that the increased medical education makes the DD surgeons "better" surgeons than SD OMS. The additional years of medical education may be why the sample reported an increased enhancement with their ability to treat the OS needs of their patients when compared to SD OMS (Figure 3). It should be noted, the actual months of OMS training is the same whether SD or DD OMS trained.
Another interesting finding from our survey of DD OMS was the relatively low response that their DD status enhanced their ability to gain dental or medical referral from each of those specific communities. The results were 63% from the medical community and only 45% from the dental community (Figure 3). This finding may correlate directly with our DD OMS response that their DD did not give them a financial advantage. If the DD OMS training does not enhance significantly their income potential or their referral base, it appears that the enhanced patient confidence is the main factor that separates SD OMS from DD OMS.
There must be other factors that go into the decision-making process to decide between SD and DD OMS training, such as fellowship training. The desire to participate in DD OMS training for some is based upon the desire to pursue cosmetic surgery fellowships, for which a medical degree would be beneficial [2,6,8] A survey by Halepas, et al. [8] of US OMS regarding their use of minimally invasive cosmetic fillers, OMS were more inclined to perform these procedures if they had DD and/or additional fellowship training. They further found that those OMS practicing under their medical licensure were more inclined to provide minimally invasive cosmetic fillers, even if not specifically trained in the procedure during the 2-years in medical school [8].
As there has been advancements in the OMS training with the development of the MD model, Kaban and Perrott [2] also point out, "new challenges exist for dual degree training." These challenges would include issues such as the possibility of some medical schools requiring a total of 4-years of medical school for OMS residents, some medical schools eliminating accepting transfer students altogether (eliminating OMS residents transferring into medical schools as 3rd-year medical students), and some states requiring 2 or 3 additional years of training for full medical licensure [2]. These are factors that could make the dual degree choice a less attractive and less practical option in the future.
Overall, results of this survey show that DD OMS still have a generally favorable view of the DD affords them, even if those benefits do not exceed increased income potential or referral rates. Most report their DD status is connected to things that make them better practitioners, including a better ability to treat patients and higher patient confidence. It will be interesting to see how these perspectives shift in the future given the recent and ongoing changes to the structure of DD OOMS programs.