The arthroscopic BANKART technique is part of the panel of surgical treatment of anterior shoulder instability, allowing reinsertion of the anterior-inferior labrum as well as the capsule at the level of the anterior glenoid rim. Its indication is based on a set of criteria gathered in the ISIS score, which must be less than or equal to 3 for an optimal result and a lower recurrence rate.
Our initial experience has shown the success of this technique with a zero recurrence rate after an average follow-up of 26 months. The perspective remains to enlarge the series with a long follow-up for a better management.
Shoulder, Anterior instability, BANKART, Arthroscopy, ISIS
Anterior shoulder instability is a common condition in young, active, and often athletic individuals dominated by recurrence of anteromedial dislocations. The treatment of this instability involves surgical procedures on the soft tissue and bone, either open or by arthroscopy.
The arthroscopic Bankart technique allows reinsertion of the anterior-inferior labrum and the capsule at the level of the anterior glenoid rim. It uses a set of criteria for the selection of eligible patients for a better result and therefore less recurrence. We report on our initial experience through a series of 5 cases operated on using this technique.
Between January 2018 and June 2021, our series includes 5 patients with recurrent anterior dislocations treated exclusively by an arthroscopic Bankart in the orthopaedic trauma department "A" at the CHU Mohammed IV of Oujda.
The average post-operative follow-up was 26 months, with extremes ranging from 12 months to 42 months. The recurrence rate was zero, with satisfactory results according to the ROWE score.
The 5 patients were male (100%), with a mean age of 25 years (22-29 years) at the time of surgery. The dominant side was right in all cases (100%). The symptomatology was dominated by recurrent dislocation (4 cases), associated with one case of recurrent subluxation. We noted an average of 9 dislocations per patient (4-13 accidents). The first episode of dislocation always occurred in a traumatic context. Three patients played sports at different levels, but all occasionally.
On clinical examination, no deformity, amyotrophy or pain was noted with preserved active mobility, the apprehension to the arm was positive in all cases (100%), the relocation test was positive (2 cases), the tendon and subacromial impingement tests were negative, with no constitutional hyperlaxity (Beighton's signs) [1], or neurological deficit.
All of our patients had a standard radiological work-up including a frontal view (neutral, internal and external rotation) and a Bernageau profile. Five patients had undergone a CT scan of the shoulder. This radiological assessment did not show a Malgaine notch with only one case of Bony Bankart on the scan (Figure 1).
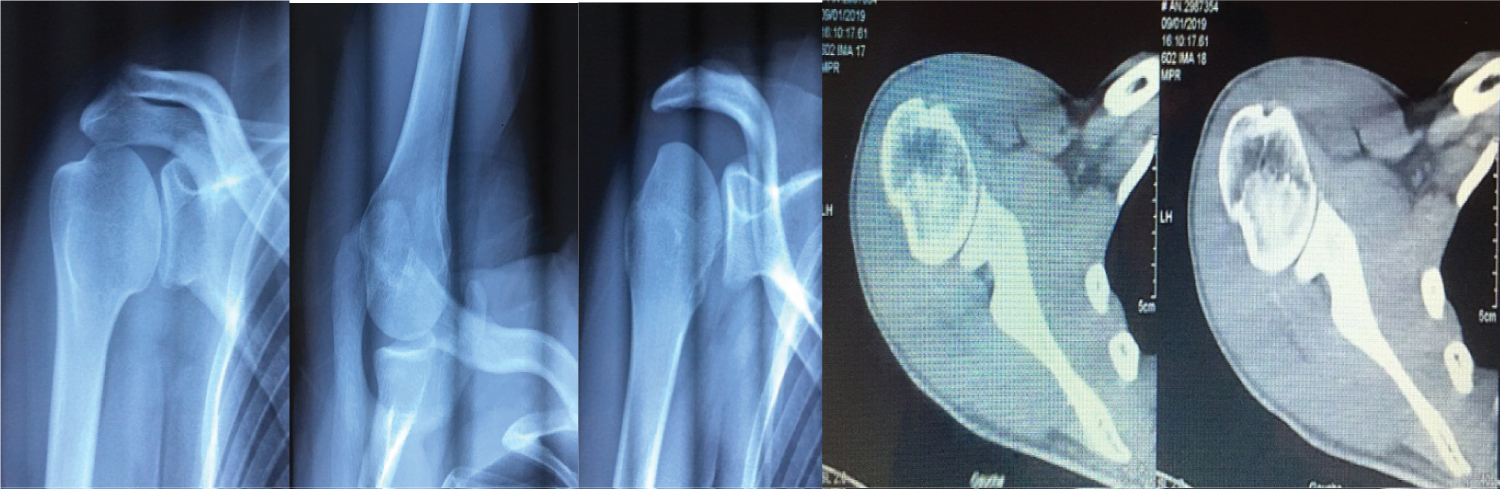 Figure 1: Frontal radiograph of the shoulder in external rotation, Bernageau Incidence, Garth Incidence, Axial scan section showing a "Bony Bankart'".
View Figure 1
Figure 1: Frontal radiograph of the shoulder in external rotation, Bernageau Incidence, Garth Incidence, Axial scan section showing a "Bony Bankart'".
View Figure 1
After clinico-radiological evaluation, the therapeutic decision based on the ISIS score, established between 1 and 2 for all cases, was to perform an arthroscopic BANKART. After exploration, the procedure consisted of assessing the presence of a HILL SACKS lesion, which was noncommittal in all cases, and did not require a filling procedure. The anterior-inferior labral detachment and the capsule were then fixed at the anterior glenoid rim at around 15 and 17 o'clock using metal anchors after the anteroinferior edge had been raised (Figure 2 and Figure 3). It should be noted that the patients had no associated lesions on the rest of the labrum.
 Figure 2: Non-engaging Malgaine notch, Anteroinferior labral detachment, Anteroinferior glenoid rim advancement, Implantation of a metal anchor.
View Figure 2
Figure 2: Non-engaging Malgaine notch, Anteroinferior labral detachment, Anteroinferior glenoid rim advancement, Implantation of a metal anchor.
View Figure 2
 Figure 3: Tightening of the anchor knot, Two anchors placed at 15 and 17 o'clock of the glenoid rim, Reinsertion of the anteroinferior labrum by two anchors, Radiological control of the anchor location.
View Figure 3
Figure 3: Tightening of the anchor knot, Two anchors placed at 15 and 17 o'clock of the glenoid rim, Reinsertion of the anteroinferior labrum by two anchors, Radiological control of the anchor location.
View Figure 3
Post-operatively, the upper limb was immobilized in elbow to body for 4 weeks with pendulum movements allowed, followed by self-passive rehabilitation until two months when active rehabilitation was started.
The average operative time after the first dislocation was 6 years with an average postoperative follow-up of 26 months.
All patients were reviewed with regular check-ups. The follow-up included a clinical evaluation, based on mobility, pain and instability, leading to a functional result assessed by the Rowe score [2], with an excellent result in 2 cases, good in 3 cases.
A follow-up radiological check consisted mainly of an evaluation of the position of the anchors in relation to the anterior glenoid rim and the appearance of glenohumeral osteoarthritis, assessed by the Samilson classification [3]. This check was without abnormalities.
No cases of recurrence of dislocation were noted.
Anterior shoulder instability is a frequent and disabling condition in young people. It is easy to diagnose with a wide variety of surgical treatments depending on the terrain and the anatomical and pathological lesions that dictate the choice of treatment. Capsulo-ligamentary lesions are the site of disinsertion of the anteroinferior capsule and its ligamentous reinforcements of the anteroinferior edge of the glenoid. Glenoid lesions are anteroinferior and are either crushes or true fractures (Bony Bankart); humeral bone lesions are represented by posterosuperior notches of the humeral head known as Malgaigne (or Hill Sacks).
The surgical techniques described all seek to eliminate one or more of the factors that contribute to instability.
The Bankart technique is the standard procedure for capsuloligamentous retractors [4], either open or arthroscopic. Proper positioning of the labrum and capsular retention helps to prevent humeral head translation and compression [5,6].
In arthroscopy, the technique was first described by Lany Johnson [7] in 1982. Since then, research has led to the development of new techniques using metallic and resorbable anchors.
The treatment strategy for anterior glenohumeral instability is defined according to the Instability Severity Index Score (ISIS) published in 2007 by Balg and Boileau [8], which highlights risk factors for failure of treatment of instability by arthroscopic Bankart repair. The higher the ISIS score, the higher the risk of recurrence. Thus, an ISIS score ≤ 3 is associated with a 5% risk of failure of isolated arthroscopic Bankart and an ISIS score greater than 6 is correlated with a 70% risk of failure.
The therapeutic choice between isolated Bankart, Bankart and Hill Sachs Filling or bone block under arthroscopy is therefore proposed according to the history, the type of sport practised, the age of the patient, the presence of hyperlaxity during the clinical examination, and the bone defects noted on the imaging work-up (X-ray and CT scan): Size of the Hill Sachs lesion, presence of glenoid erosion or glenoid fracture. All these criteria are combined in the ISIS score, which plays an important role in the treatment strategy [9].
This technique is associated with a recurrence rate of 11 to 22% in young patients, depending on the author. Indeed, Wheeler [10] in 1989 published a recurrence rate of 22% for Bankart under arthroscopy in a population of young athletes. Mazzoca [11] in 2005 found a recurrence rate of 11% after Bankart repair in young people playing contact sports. In 2014, a study by Loannis Gigis [12] reported a 13% recurrence rate after arthroscopic Bankart.
The weakness of these studies is that they underestimate the failure rates of the treatments because their follow-up is often equal to 2-3 years whereas 50% of failures appear after 2 years post-surgery [13,14].
The arthroscopic Bankart procedure has proven successful in young patients with anterior shoulder instability, meeting the ISIS score evaluation criteria with a lower recurrence rate. The challenge remains to recruit the right candidates for this technique for early management and better outcome.
The authors declare that they have no conflicts of interest in relation to this article.
All authors contributed to the conduct of this research work and read and approved the final version of the manuscript.