Wilms' tumor (WT) or nephroblastoma, is an embryonal kidney cancer, with a low incidence rate in adults, less than 0.2 per million per year [1]. There are no clinical or radiological differences with renal cell carcinoma (RCC), so its diagnosis is unexpected and overdue [2]. In addition, due to its rarity, adequate and risk-adapted treatments, in accordance with international protocols (developed from the pediatric oncology perspective), are delayed [3]. That explains why survival outcomes have been historically worse in adult WC when compared with WT in children [4].
We herein report the case of a 23-years-old patient diagnosed of stage IV rapidly progressive WT, treated with nephrectomy and right lobe partial hepatectomy, who could not start adjuvant chemotherapy because of WT aggressiveness. A review of the previous literature was also performed.
A 23-year-old man was studied in November 2014 for monosymptomatic, left-flank pain, resistant to analgesia.
The abdominal X-ray showed a heterogeneous, calcified, poorly delimited image of 5 cm in the left hypochondrium (Figure 1). Tumoral markers, and hepatic-renal profiles were normal on blood test. CT scan showed a heterogeneous and calcified left renal mass, sized 12 × 7.6 cm, dependent on the upper pole, with no vascular invasion. Left hiliar and para-aortic adenopathies, up to 3 cm were also reported. Moreover, a 4 × 3.6 cm hypodense lesion in the 6th hepatic segment, and another one, 12 mm, in the hepatic dome, compatible with metastasis, were described (Figure 1).
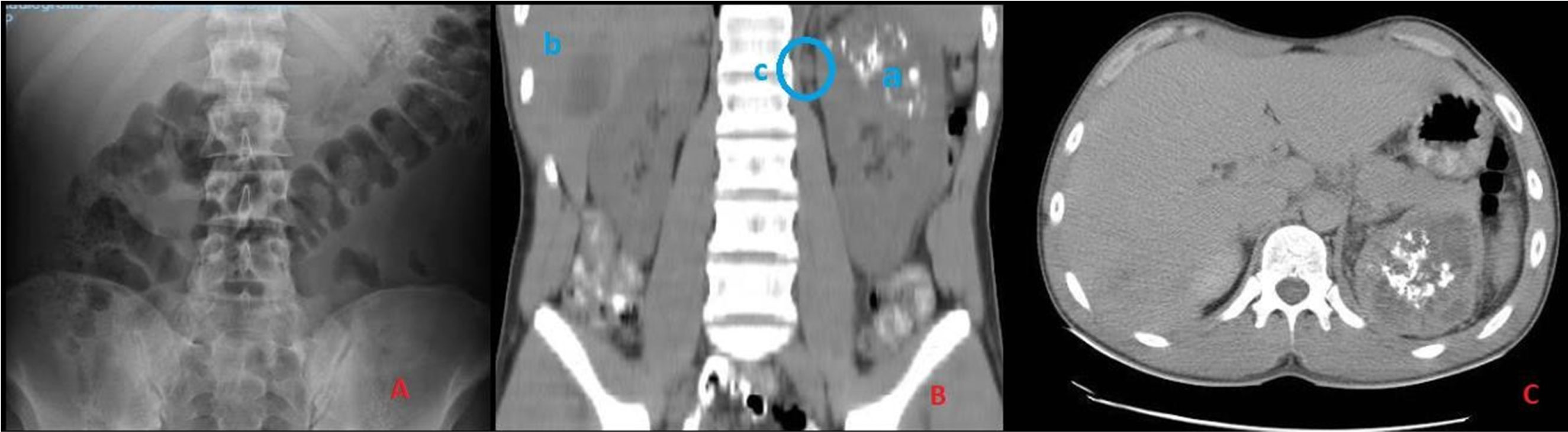 Figure 1: A) Renal Wilms tumor with a classic hematoxiline - eosine histology (left) and less differentiated diffuse pattern (right) (HE × 100); B) Anaplastic cells area with big irregular shaped nuclei (HE × 200); C) Inmunohistochemical stain for p53 was negative in the well differentiated area, while focally positive in anaplastic cells (IHC p53 × 100); D) WT1 was diffusely positive in both patterns (IHC WT1 × 100); E) Wilms tumur metastasis in liver with few trapped hepatocites (arrows) (HE × 200).
View Figure 1
Figure 1: A) Renal Wilms tumor with a classic hematoxiline - eosine histology (left) and less differentiated diffuse pattern (right) (HE × 100); B) Anaplastic cells area with big irregular shaped nuclei (HE × 200); C) Inmunohistochemical stain for p53 was negative in the well differentiated area, while focally positive in anaplastic cells (IHC p53 × 100); D) WT1 was diffusely positive in both patterns (IHC WT1 × 100); E) Wilms tumur metastasis in liver with few trapped hepatocites (arrows) (HE × 200).
View Figure 1
On December 2014, elective left radical nephrectomy with loco-regional lymphadenectomy and right lobe partial hepatectomy was performed. Despite a good initial evolution, an urgent open hepaticojejunostomy was performed on the 4th postoperative day, as the patient started with elevation of cholestasis' enzymes, as well as coluria and acolia, and CT scan described intrahepatic bile duct dilatation and pneumoperitoneum. Afterward, the patient evolved favorably, being discharged on January 2015.
Pathology reported a 11 cm WT, with a three-phase histological pattern (mucinous differentiation and bone metaplasia in the stromal component) (Figure 2). Also described 30% of necrosis and multiple foci of anaplasia, not reaching the surgical margin. Tumor infiltrated renal capsule and homolateral suprarenal gland respecting surgical-margin.
 Figure 2: A) Renal Wilms tumor with a classic hematoxiline - eosine histology (left) and less differenciated diffuse pattern (right) (HE × 100); B) Anaplastic cells area with big irregular shaped nuclei (HE × 200); C) Inmunohistochemical stain for p53 was negative in the well differenciated area, while focally positive in anaplastic cells (IHC p53 × 100); D) WT1 was diffusely positive in both patterns (IHC WT1 × 100); E) Wilms tumur metastasis in liver with few trapped hepatocites (arrows) (HE × 200).
View Figure 2
Figure 2: A) Renal Wilms tumor with a classic hematoxiline - eosine histology (left) and less differenciated diffuse pattern (right) (HE × 100); B) Anaplastic cells area with big irregular shaped nuclei (HE × 200); C) Inmunohistochemical stain for p53 was negative in the well differenciated area, while focally positive in anaplastic cells (IHC p53 × 100); D) WT1 was diffusely positive in both patterns (IHC WT1 × 100); E) Wilms tumur metastasis in liver with few trapped hepatocites (arrows) (HE × 200).
View Figure 2
On immunohistochemical study: Tumor cells expressed diffusely WT1 and maintained nuclear expression with INI1; p53 was over-expressed in anaplasia foci. Tumor infiltration was present in 3 hiliar adenopathies and 2 metastatic foci, not reaching surgical-margin, were found on right hepatectomy.
At the first clinical review, 15 days later, the patient reported dorsal back pain, constitutional syndrome and loss of 14 kg. CT scan showed a large retroperitoneal mass in nephrectomy's bed that extends to the perivascular retroperitoneal space and the ipsilateral psoas muscle. Multiple hypo-attenuating lesions in the liver. Free fluid in right subphrenic space and pelvis of new appearance with peritoneal uptake. Multiple pulmonary nodules in both inferior lobes and lytic lesions in vertebral bodies in relation to metastasis.
Patient was hospitalized, starting symptomatic treatment, and a biopsy of the retroperitoneal mass was performed to confirm the recurrence of nephroblastoma.
The patient suffered a significant deterioration in general condition and dead on February 2015, with no possibility of administering adjuvant chemotherapy treatment.
Wilms tumor (WT) is a kidney tumor, extremely rare in adult population, but is the most common solid tumor in children. Adult WT incidence rates vary between 0.17 and 0.27 per million per year. About 70 new adult WT are diagnosed in Europe each year. The proportion of WT among all kidney cancers in adults was 0.33% or less in most registries [1].
Pathological diagnosis of adult WT is based on 6 criteria: primary renal neoplasm; primitive blastematous spindle or round cell component; formation of abortive or embryonal tubular or glomeruloid structures; no area of tumor diagnostic of hypernephroma; pictorial confirmation of histology ; age over 15-years-old [5].
There is no histopathologic difference between adult or child WT. WT comprises blastemal, stromal and epithelial components, which are present in varying proportions. These proportions determine different prognosis. Blastemal predominance is suggested to have poor outcome despite therapy. Epithelial and stromal kinds represent intermediate risk tumors [6-8].
Anaplasia, characterized by multipolar mitotic figures, enlarged nuclei at least three times and hyperchromatic nuclei, is described in approximately 10% of cases of WT. Its identification, and description of its focal or diffuse distribution is important. Patients with diffuse anaplastic tumors showed a higher relapse rate and worse outcome [6-8].
Immunohistochemistry studies are not normally required, but the presence of cytokeratin, vimentin, desmin, actin, and WT1 allows to distinguish predominant blastemal tumors from rare tumor. WT1 is seen in some blastemal and epithelial elements but not in the stromal components [6-8].
Differential diagnosis between WT and other renal cell cancers is not possible by X-ray, ultrasound or other radiological exam [2]. Contrast-enhanced MRI is the most accurate imaging modality to detect extension local and vascular extension, nephroblastomatosis or contralateral affectation at diagnosis [9]. Nevertheless, abdominal and chest CT scan is recommended by the International Society of Pediatric Oncology (SIOP) to diagnose WT in adults and its local or distant extension [3]. Some studies have been published describing radiological characteristic of WT in both image modalities [10]. Screening of other metastasis sites is not advised unless suggestive symptoms are present. PET-CT currently has no role in the initial diagnosis, but it may be useful at the first relapse to accurate diagnosis of the full metastatic disease [10].
Staging criteria of WT are based on the anatomic extent of the tumor at nephrectomy piece. There are two main classifications: The National Wilms' Tumor Study Group (NWTS) which proposes a pre-chemotherapy nephrectomy [11]; and the SIOP classification which advises 4-6 cycles of chemotherapy previous to nephrectomy [6] (Table 1).
Table 1: SIOPS and NWSTG Wilms tumor staging system according to anatomical extension. View Table 1
Adult series report a higher incidence of advanced disease (stage III or IV), ranging from 45-70%, compared with 33% in pediatric series. Historically, the stage-for-stage prognosis in adults was poorer compared with children. Adult WT prognosis has been improved in the last decade by adapting pediatric protocols to adults population, following the recommendations of SIOP and Children's Oncology Group (COG) [3].
This consensus recommends include in pediatrics trials adults who are suitable to be recruited. Moreover, therapeutic recommendations for adult patients who can't be recruited re described in Figure 3.
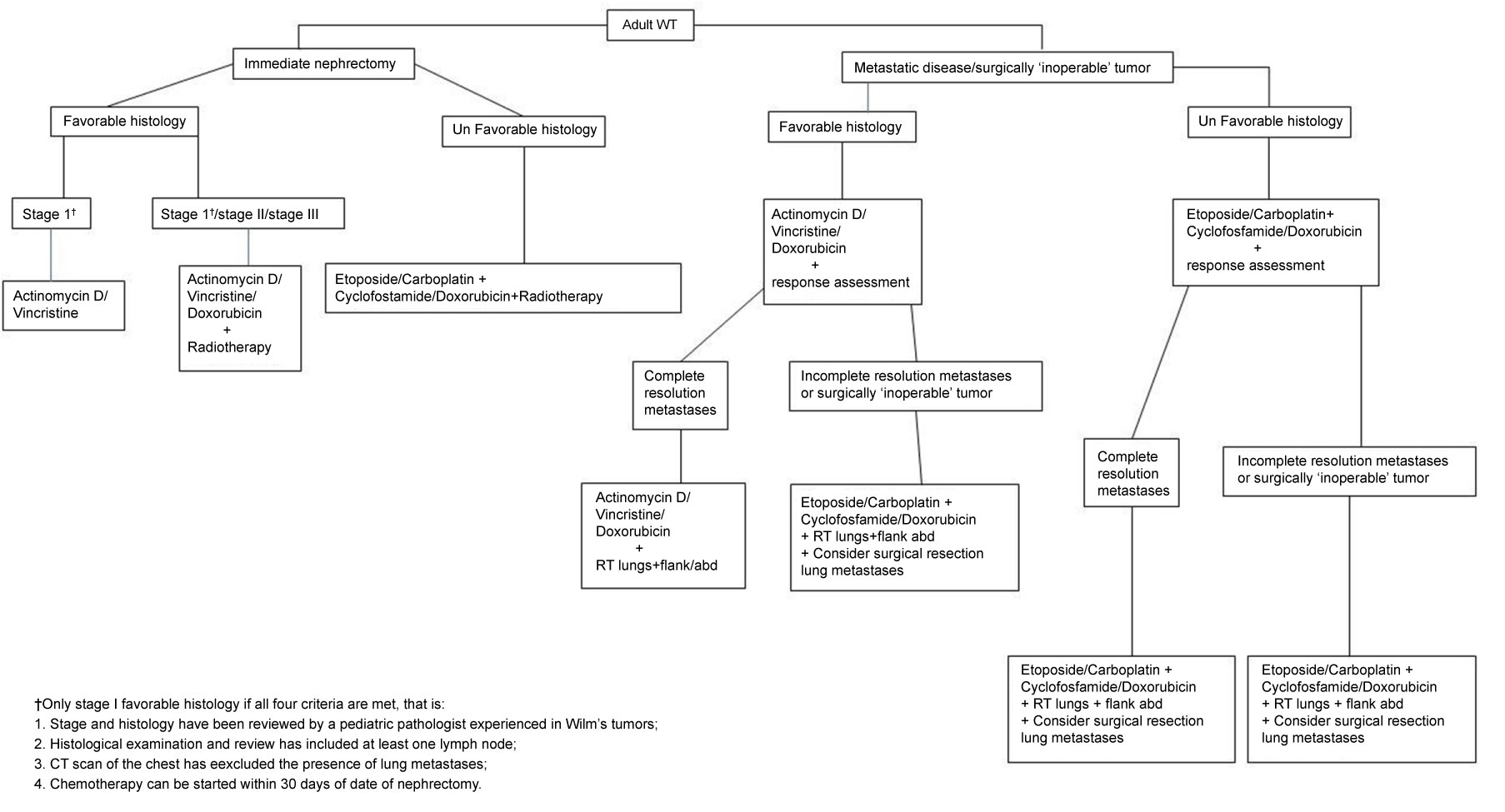 Figure 3: Therapeutic algorithm, proposed by the SIOP and COG, in adults with Wilms tumor according to the performance of previous nephrectomy and the prognostic group [3].
View Figure 3
Figure 3: Therapeutic algorithm, proposed by the SIOP and COG, in adults with Wilms tumor according to the performance of previous nephrectomy and the prognostic group [3].
View Figure 3
In order to anticipate the diagnosis and improve the management of WT by neoadjuvant chemotherapy, some groups propose the performance of renal tumor biopsy (RTB) before nephrectomy [12].
There are several data supporting percutaneous biopsy previously to surgical treatment of renal mass in young adults. On patients aged 18-45 years, the reported incidence of benign histology on piece is over 20% [13]. Patients younger than 40-years-old, just represents 0.5-2% of all renal cell cancer (RCC) [14]. In addition, the proportion of different histologies of RCC in this group of age, varies with respect to older patient, with a decrease of clear cell RCC [15]. In these patients, nephron sparing management avoid detriment of renal function and the consequent deterioration at cardiovascular level [16]. The median age at presentation of adult WT is 34years, according to EUROCARE study [1].
RTB is a procedure with a high accuracy. The median concordance rate of tumor histology between RTB and surgical pathology vas 90.3%. Median Cohen kappa coefficient value was 0.683 (IQR: 0.52-0.95), indicating a good degree of agreement. It is also a safe procedure with a median overall complication rate of 8.1%, and only a few of the Clavien > 2 complications [17,18].
It is reported, that not delaying WT diagnosis when it is suspected has a great importance. For this porpoise SIOP and COG recommend refer the nephrectomy sample to a specialized pathologist for WT confirmation, before ruling out other pathologies. Chemotherapy and radiotherapy, if necessary, should be planned to start ideally by day 14 post-nephrectomy, although delaying the start until day 30 is acceptable [3]. Tarenziani, et al. reported differences in 5-years event free survival when starting treatment within 30 days post-surgery (60 ± 15%) compared with those who delayed treatment greater than 30 days (14.3 ± 13%) (p = 0.003). Differences in OW were 80 ± 12% vs. 28, 6 ± 17% respectively (p = 0.005) [4].
According to SIOP, neoadjuvant chemotherapy for 4-6 weeks reduce tumor size and intraoperative tumor rupture rates, thus, decreasing difficulty of the surgery and local recurrence rates. Therefore, preoperative core biopsy should be considered in young adults (18-40 years) to establish proper pathological diagnosis and give the chance of neoadjuvant chemotherapy benefits [3].
Wilms tumor is a rare entity in adulthood, with a main presentation in the third decade of life. Its diagnosis is histological, since there are no radiological tests that differentiate it from other renal tumors. Avidity in the diagnosis, for which expert pathologist should be consulted at the time of suspicion, and the quickness in the beginning of the adjuvant chemotherapy treatment according to the SIOP international consensus (ideally before 14 dais), will mark the prognosis of this pathology.
Renal Cell Carcinoma is infrequent in population under 40-years-old. In these patients, clear cell RCC's histological variants, as WT, are more frequent. Also, benign histologies are reported up to 20% of series. RTB, allows presurgical diagnosis with 90% accuracy, and low rate of complications. RTB enable a nephron sparing approach, which is mandatory to preserve renal function, and also, given the opportunity to administer neoadjuvant treatment in tumors as WT, in which it is indicated.