The aim of this study was to investigate the effects of the preemptive administration of a single dose of intravenous (IV) ibuprofen on the intraoperative hemodynamic parameters, recovery characteristics, and postoperative pain management in patients undergoing laparoscopic cholecystectomy. The time to first analgesic requirement during postoperative period was the main goal of this study.
Following ethical committee approval, sixty patients scheduled for laparoscopic cholecystectomy with American Society of Anesthesiologists (ASA) physical status I-II and aged 30-65 years of either genders were included in this prospective, randomized, placebo-controlled double blinded study. Patients were randomly divided into two groups.
The study group (group I) received 400 mg ibuprofen in 100 ml IV saline 15 min before anesthesia induction, whereas the placebo group (group C) received IV 100 ml saline only. The study drug and the saline were administered by an anesthesia nurse blinded to the study. The same general anesthesia protocol was applied in both groups. Hemodynamic parameters (non-invasive systolic (SAP), diastolic (DAP) and mean (MAP) arterial pressure, heart rate (HR), bispectral index (BIS) values and SpO2 values were recorded before induction (baseline) and after induction, peroperative 10, 20, 30, minutes., before extubation. The time to achieve a modified Aldrete score of ≥ 9 was recorded as the recovery time. During postoperative period, the time to first analgesic requirement and the total amount of analgesics within 24 hours was recorded. Patients were asked to give a number between from 1 to 5 for the satisfaction assessment for the anesthesia management.
There was no difference between the groups in terms of hemodynamic findings before anesthesia induction and in the peroperative period. The time until Aldrete score of 9 was statistically significantly shorter in Group I (Group I 3.8 ± 1.4 min, and Group C 6.3 ± 1.9 min, p < 0.001). Sevoflurane consumption was lower in the group given preemptive single dose IV ibuprofen, but the time to first postoperative analgesic requirement was longer (p < 0.001). Total analgesic consumption was highest in Group C (p < 0.001).
Preemptive single dose i.v. ibuprofen (400 mg) can be used in laparoscopic cholecystectomy with the advantages of reducing the consumption of peroperative sevoflurane, providing better VAS scores, shortening the time to the first postoperative analgesic requirement and reducing analgesic consumption.
Ibuprofen, Preemptive analgesia, Laparoscopic cholecystectomy, Postoperative analgesia
Laparoscopic cholecystectomy is a widely preferred minimally invasive surgical technique for gallstone diseases due to its shorter hospitalization, faster healing, a better cosmetic outcome, and less postoperative pain characteristics. The pain after laparoscopic cholecystectomy is regarded as visceral, quite complex and resulted from the insufflation of carbon dioxide into the peritoneal cavity, abdominal distension, port-site incisions and patient factors [1]. Although the pain intensity and duration are less than the open surgical approach, the optimum analgesic modality has remained a challenging issue. Multimodal analgesia regimen combining opioids, non-steroidal anti-inflammatory drugs, and local anesthetic infiltration to the port sites are the most recommended treatment of choices for postoperative pain management after laparoscopic cholecystectomy [2].
Preemptive use of systemic analgesics combined with the general anesthesia has some beneficial effects such as blocking nociceptive pathways, reducing the amount of pharmacological agents needed to maintain the general anesthesia, and decreasing the time to recover from the drug-induced central nervous system depression [3]. Adequate preemptive analgesia has two basic requirements; verification of the effectiveness of the direct pharmacological effect of treatment and the extension of an antinociceptive treatment into the initial postoperative period [4].
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the good treatment of choices for the postoperative pain unless contraindicated due to its opioid-sparing effect and minimizing the opiate-induced adverse reactions [5]. The guideline of the American Society of Anaesthesiologist, Task Force on Acute Pain Management recommends that this group of drugs have a significant role in postoperative multimodal pain management [6].
Like other NSAIDs, ibuprofen has anti-inflammatory, antipyretic, and analgesic properties. It causes a rapid, reversible and competitive inhibition of the cyclooxygenase (COX) isoenzymes. The analgesic property is related to the inhibition of COX-2, whereas the inhibition of COX-1 isoenzyme results in the gastrointestinal or kidney side effects [7]. This drug is a propionic acid derivative and the oral form has been widely used for many years. By the introduction of ready-to-administration intravenous ibuprofen solution, it's increasingly been used in multimodal analgesia for the management of postoperative pain [8]. It's been shown that the use of intravenous (IV) ibuprofen is a safe and effective drug to reduce the severity of pain, and opioid consumption in surgical interventions such as bariatric, orthopedic, abdominal, and gynecologic surgeries [9-12]. The effect of NSAIDs on wound healing is a debating issue and animal studies indicated that non-selective NSAIDs generally inhibit wound healing. However, either COX-1 or COX-2 selective NSAIDs tend to show no effect on wound healing [13].
The aim of this study was to investigate the effects of the preemptive administration of a single dose of IV ibuprofen on the intraoperative hemodynamic parameters, recovery characteristics, and postoperative pain management. The time to first analgesic requirement during postoperative period was the main goal of this study.
This prospective, randomized, placebo-controlled double blinded study was conducted after receiving the approval of the ethics committee (2020/514/170/24) and the written, informed consent of all of the participants, according to the Good Clinical Practice guidelines and the principles of the Declaration of Helsinki. Sixty patients scheduled for laparoscopic cholecystectomy with American Society of Anesthesiologists (ASA) physical status I-II and aged 30-65 years of either genders were included the study.
Patients with a body mass index of more than 30 kg/m2, pregnancy, cardiac or renal failure, mental disturbance, neurological disease, communication difficulties, being unable to comprehend visual analogue scale, previous clinical history of chronic pain, a history of long-term or during recent 24 h nonsteroidal anti-inflammatory drug use, a history of peptic ulcer, gastrointestinal bleeding or inflammatory bowel disease, known allergy to ibuprofen or other nonsteroidal anti-inflammatory drugs were excluded.
Randomization was achieved by using a computer-generated randomization program operated by another clinician blinded to the study and the patients were allocated into two groups to receive either preemptive single dose IV ibuprofen (Intrafen 400 mg/4 ml, en İlaç Ve Sağlık Ürünleri San. Ve Tic. Ltd. Sti., Ankara, Türkiye) (Group I = 30) or IV saline (100 ml) (Group C = 30).
Patients were interviewed preoperatively to explain the study and introduced to the concept of the visual analog scale (VAS), with a 10-cm vertical score ranged from 0 = no pain to 10 = worst pain imaginable. The patients fasted for both solids and clear liquids at least 8 hours prior to the surgical procedure. No premedication was applied.
On arrival to the preoperative care unit, IV access was established with an 18-G IV cannula. The study group received 400 mg ibuprofen in 100 ml IV saline 15 min before anesthesia induction, whereas the placebo group received IV 100 ml saline only. The study drug and the saline were administered by an anesthesia nurse blinded to the study.
Before induction of anesthesia, a bispectral index sensor (BIS Quatro; Medtronic plc, Dublin, Republic of Ireland) was placed on the patient's forehead and connected to a BIS Vista monitor (Medtronic plc, Dublin, Republic of Ireland). Following standard monitoring included a 3-lead electrocardiogram (ECG) with continuous ST-segment analysis, peripheral oxygen saturation (SpO2), and non-invasive blood pressure, anesthesia in both groups was established with IV 1 μg/kg fentanyl and 2-2.5 mg/kg propofol. Endotracheal intubation was facilitated by the administration of IV rocuronium 0.6 mg/kg. Anesthesia was maintained with sevoflurane of 2-3% in 50% oxygen-air mixture in a fresh gas flow of 2 L/minute.
Hemodynamic goals were to maintain the intraoperative mean arterial pressure and heart rate within 20% of the pre-induction values. If the mean arterial pressure and heart rate increased more than 20%, supplementary dose of 1 μcg/kg fentanil was applied. In case of decreasing more than 20%, 5 mg IV ephedrine was administered. Sevoflurane was titrated to maintain a BIS value between 40 and 60.
Laparoscopic cholecystectomy was performed with four-port standard technique by highly experienced surgeons in laparoscopic interventions. After insertion of a subumblical 10-mm port, pneumoperitoneum was created by placing a Veress needle and the intraabdominal pressure was maintained at 10-12 mmHg. The operation table was positioned in reverse Trendelenburg and sided to the left. A 10-mm trocar was placed in the epigastrium to the right of the falciform ligament with two additional 5-mm ports in the right upper abdomen. After resection of gallbladder, it was retrieved through the epigastric port. Nasogastric tube was used only for decompression of the stomach and then removed. No abdominal drainage was used to any patient.
At the end of the surgery, the anesthetic gas mixture was replaced with 100% oxygen and the neuromuscular block was reversed using a neostigmine (0.05 mg/kg) and atropine (0.01 mg/kg) combination. After adequate ventilation, protective airway reflexes and the patients' response to verbal commands were achieved, patients were extubated. Following transfer to the post-anesthesia care unit, they discharged to the general surgery clinic when patients attained a modified Aldrete score of ≥ 9.
Patient characteristics of age, gender, height, weight, and ASA physical status were recorded. Hemodynamic parameters (non-invasive systolic (SAP), diastolic (DAP) and mean (MAP) arterial pressure, heart rate (HR), bispectral index (BIS) values and SpO2 values were recorded before induction (baseline) and after induction, peroperative 10, 20, 30, minutes, before extubation.
The time to achieve a modified Aldrete score of ≥ 9 was recorded as the recovery time. During postoperative period, the time to first analgesic requirement and the total amount of analgesics within 24 hours was recorded. Patients were asked to give a number between from 1 to 5 for the satisfaction assessment for the anesthesia management.
The demographic characteristics and collected data of the patients were entered into IBM® SPSS® (the Statistical Package for the Social Sciences) Statistics version 23. Variables were characterized using mean, maximum and minimum values, and percentage values were used for qualitative variables. Normal distributions were reported as mean ± SD and Student's t-test was used for comparisons between groups. For the analysis of qualitative variables Pearson chi-square test was used if the group was small, Fisher's exact test was used. Nonparametric continuous variables were recorded as median and intermittent distribution and compared using Mann-Whitney U tests. In the comparison of both groups in terms of VAS, two-way ANOVA test was used for the change in time. p < 0.05 value was considered statistically significant.
Totally 60 patients were recruited into the study (Figure 1). Patients' characteristics were shown in Table 1.
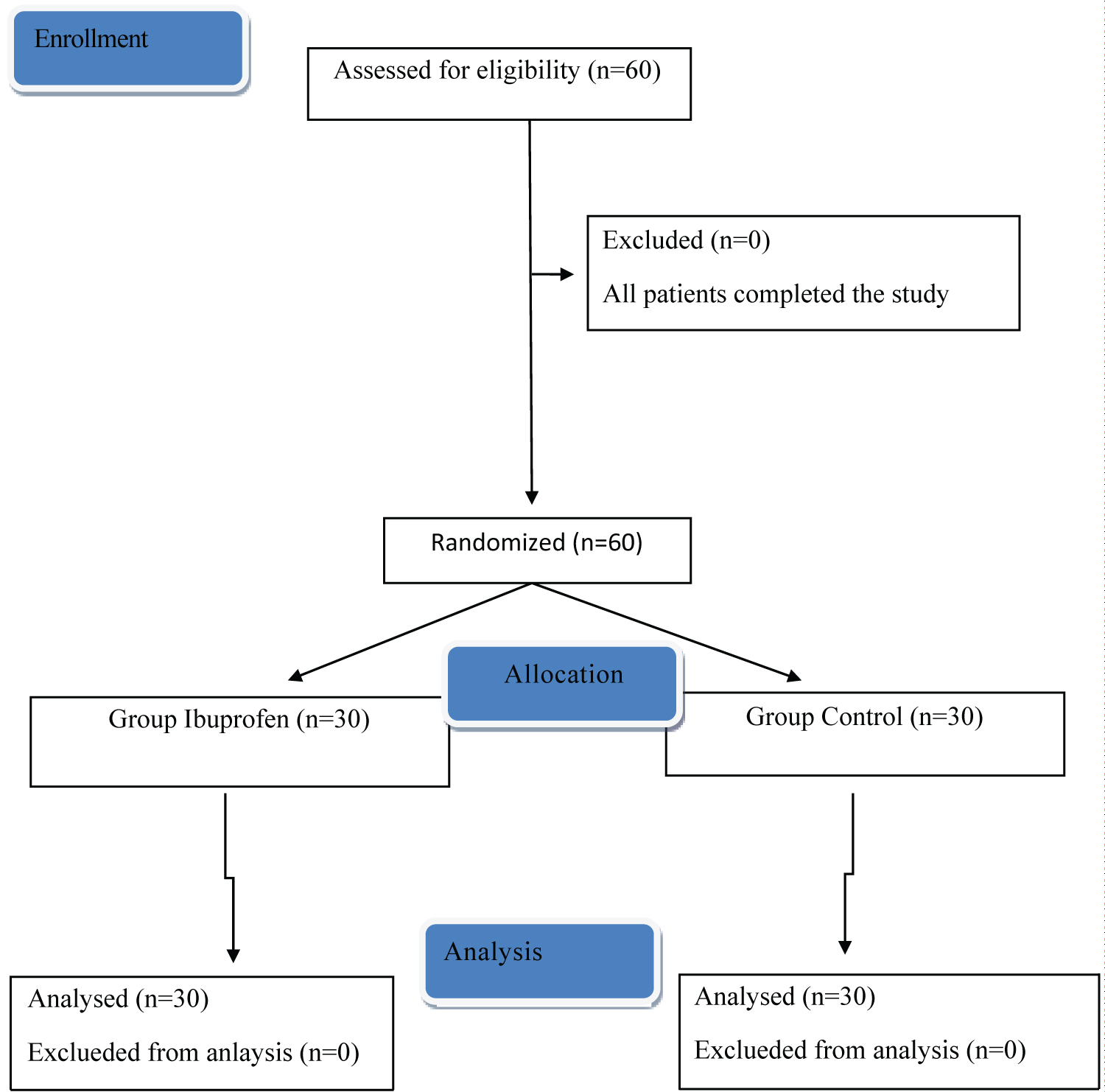 Figure 1: The CONSORT flowchart of the study. View Figure 1
Figure 1: The CONSORT flowchart of the study. View Figure 1
Table 1: Patients characteristics. View Table 1
There was no difference between the groups in terms of hemodynamic findings before anesthesia induction and in the peroperative period. However, BIS values were found to be higher in Group I from the 20th minute to the pre-extubation period compared to Group C and were statistically significant in this regard (Table 2).
Table 2: Hemodynamic parameters of the patients (mean ± SD). View Table 2
Aldrete 0 minute scores were similar between groups (7.4 ± 0.5 in Group I, and 7.2 ± 0.5 in Group C, p = 0.139). Aldrete 1st hour scores were 9 in all patients. The time until Aldrete score of 9 was statistically significantly shorter in Group I (Group I 3.8 ± 1.4 min, and Group C 6.3 ± 1.9 min, p < 0.001).
Sevoflurane consumption was lower in the group given preemptive single dose IV ibuprofen, but the time to first postoperative analgesic requirement was longer (Table 3). When the total amount of analgesics used in the first postoperative 24 hours was compared, only 1g i.v. paracetamol was sufficient for all patients in Group I, whereas the control group required 1.7 ± 0.7g i.v. paracetamol (p < 0.001). In addition, 100 mg i.v. tramadol was administered to all patients in the control group as an additional analgesic.
Table 3: Consumption of the anesthesia drug and time to first analgesic requirement. View Table 3
When both groups were compared in terms of VAS scores, patients who were given preemptive single dose i.v. ibuprofen had significantly lower VAS scores (Table 4).
Table 4: The comparison of VAS values between Group I, Group C. View Table 4
Nausea and/or vomiting was not observed in any patient.
The aim of this study was to evaluate the effect of postoperative analgesic effectiveness of preemptive ibuprofen on peroperative hemodynamic parameters and recovery criteria in laparoscopic cholecystectomy. As a result of the study, it was observed that the pre-operative ibuprofen decreased peroperative sevoflurane consumption, the time to first analgesic requirement. Besides, the time to recovery was shorter, and there was a statistically significant decrease in VAS scores compared to the control group. Also in the group given ibuprofen, analgesic consumption was found to be less in the postoperative period.
In the postoperative period, patients complain of severe pain c after laparoscopic cholecystectomy [14]. For this reason, many analgesic drugs are applied to patients before, during or after surgery [15]. An effective postoperative analgesia results in early mobilization, shortened hospital stay, and reduced costs. One method for postoperative pain management is preemptive analgesia. This method represents analgesic administration before painful stimulation begins [16]. Local anesthetics such as bupivacaine, lidocaine and drugs such as ibuprofen, gabapentin, pregabalin can be used [17].
To reduce postoperative opioid consumption, analgesic and/or anti-inflammatory drugs and opioids are used before and during surgery. Among these drugs most commonly paracetamol and ibuprofen with low potential for side effects are used [8].
In a study evaluating the effect of ibuprofen on postoperative pain, 800 mg ibuprofen was found to reduce postoperative opioid consumption [18]. In another study, preemptive analgesia together with postoperative primary care analgesic treatment has been shown to reduce opioid use more effectively [19].
Gazal, et al. found lower VAS scores in their group given ibuprofen and attributed this to anti-inflammatory activity of the drug [20]. Moss, et al. showed that single dose i.v. ibuprofen significantly reduced opioid consumption in the postoperative period in children undergoing tonsillectomy [21]. In our study, VAS scores, postoperative analgesic need together with the time to first analgesic need of the group who were given preemptive i.v. ibuprofen were comparatively lower.
Southworth, et al. stated that ibuprofen is a good option because of its analgesia and balanced anti-inflammatory effect [22]. In another study, it was reported that preoperative i.v. ibuprofen reduces stress response in laparoscopic cholecystectomies [23].
In their meta-analysis Moore, et al. emphasized that ibuprofen had a stronger analgesic effect compared to ibuprofen and paracetamol. However, in their study, oral forms of drugs were used [24]. The i.v. form of ibuprofen has been evaluated in different studies as for postoperative pain management.
In a study evaluating the effectiveness of i.v. ibuprofen and paracetamol for postoperative pain management in laparoscopic cholecystectomies, 800 mg i.v. ibuprofen has been shown to result in lower pain scores and opioid consumption [25]. It has been reported that i.v. ibuprofen is very safe and effective in patients who will undergo orthopedic surgery [26].
In our study, we used a single dose of i.v. ibuprofen 15 minutes before anesthesia induction. Our aim was to reach peak plasma concentration at the beginning of the surgical stimulus and to see fewer side effects with a single dose of 400 mg.
There are some limitations for this study. First, ibuprofen 400 mg was used as a single dose regardless of patients' weight. Different results and a different side effect profiles may have been obtained with a dose of 800 mg. The second limitation is that the 400 mg dose was used only before surgery and not after surgery. We aimed to evaluate the effectiveness of the preemptive dose. Third, the effect on the length of hospital stay has not been evaluated.
In conclusion, preemptive single dose i.v. ibuprofen (400 mg) reduced analgesic consumption in the first 24 hours postoperatively in patients undergoing laparoscopic cholecystectomy. Preemptive single dose of ibuprofen (400 mg) can be used in laparoscopic cholecystectomy with the advantages of reducing the consumption of peroperative sevoflurane, providing better VAS scores, shortening the time to the first postoperative analgesic requirement and reducing analgesic consumption.