Ear Nose Throat (ENT) surgery has been the highest risk of postoperative nausea and vomiting. Despite the advancement of the modern anesthetic techniques in the management and understanding of postoperative nausea and vomiting (PONV), the events of nausea and vomiting in ENT surgery still remains a major problem for participants in the postoperative care unit. Therefore, the aim of this study was to determine the incidence and identify the risk factors of PONV among surgical ENT participants in Orotta Medical Surgical National Referral Hospital.
The study was hospital based prospective quantitative design conducted in Orrota National Referral Hospital (ENT department). A total of 125 participants scheduled and followed for elective ENT surgery during the study period from December 1, 2017 until February 28, 2018. The participants were followed for the outcome of nausea, retching and vomiting for 24 hours post-operatively. Data was collected by direct observation in the recovery room and filling a questionnaire in the participants ward. Then data was analyzed using SPSS version 22. Univariate analysis was performed and variable with p-value less than 0.05 were considered as significant.
The study concluded that the overall incidence of PONV in ENT Orrota National Referral Hospital was 32.8%. Out of the occurrence of PONVs, the highest percentage was vomiting (48.8%) while nausea, retching as well as nausea and vomiting together had 17.1%. The study revealed that age less than 15-years-old (RR = 1.78, 95% CI, 1.00-3.15), history of motion sickness (RR = 2.78, 95%CI, 1.82-4.24), use of thiopental as induction agents (RR = 1.72, 95%CI, 1.03-2.87), administration of combined neostigmine and atropine as reversal agents (RR = 1.80, 95%CI, 1.07-3.03), and presence of pain post-operatively (RR = 2.38, 95%CI, 1.34-4.22) has significant risk factor for PONV.
The study concluded that the overall incidence of PONV in ENT Orrota National Referral Hospital was 32.8%. The risk factors for the incidence of PONV were; age less than 15-years-old, history of motion sickness, use of thiopental as induction agent, administration of combined neostigmine and atropine as reversal agents, and presence of pain postoperatively.
Incidence, PONV, ENT
BMI: Body Mass Index; CDC: Center for Disease Control; CTZ: Chemoreceptor Trigger Zone; ENT: Ear, Nose and Throat; HMIS: Health Management Information Service; IPPV: Intermittent Positive Pressure Ventilation; MAC: Minimum Alveolar Concentration; NGT: Naso-gastric Tube; ONRH: Orrota National Referral Hospital; OR: Operating Room; PONV: post-operative Nausea and Vomiting; POV: Post-operative vomiting; SPSS: Scientific Package for Social Science; WHO: World Health Organization
Postoperative nausea and vomiting (PONV) is one of the leading, distressing and undesirable feeling of nausea and vomiting postoperatively following surgery, anaesthesia and opioid therapy. Nausea and vomiting are not synonyms, being important to separate them since some drugs are more effective against nausea and others against vomiting [1]. Nausea is the uncomfortable sensation associated to the need for vomiting, while vomiting is the forced expelling of gastric content [2].
The causes for PONV are multifactorial, including participant-related, anesthetic and surgical factors. Female gender, as a participant related factor, is consistently the strongest well established risk factor for PONV with an odds ratio (OR) of aproximately 3, which indicates that female participants are on average three times more likely than men to suffer from PONV [3-5]. Non-smoking status and history of motion sickness or PONV are also highly associated participant-related risk factors. Similarly, in adult participants with increasing age the incidence of PONV decreases. For paediatric participants, age increases the risk of POV (Postoperative vomiting), such that children older than 3 years have been shown to have an increased risk of POV compared to children younger than 3 [3]. The use of dose dependent volatile anesthetic drugs has associated with a two-fold increment in the incidence of PONV and no significant difference on the use of different volatiles [3,6]. On top of that, opioid administration in the intraoperative or postoperative period leads to higher incidence of PONV [3-5,7]. Some surgical procedures which are associated to higher incidence of PONV such as strabismus correction, ENT, gynecologic, shoulder and laparoscopic surgeries have similar relative risk when assessed by Apfel's risk factor tool [2]. In general, those factors requires release of 5-hydroxytryptamine (5-HT) in a cascade of neuronal events involving both the central nervous system and gastrointestinal tract. The 5-HT subtype 3 receptor (5-HT3) participates selectively in the emetic response [8].
PONV is not a benign condition as it leads to many physiological and economic problems. About 0.2% of participants may suffer untreatable PONV, delaying hospital discharge, requiring unexpected admissions, generating a low level participants' satisfaction and increasing hospital costs. In addition to the above mentioned complications, more severe situations may be generated, such as suture dehiscence, vomiting, aspiration pneumonia, dehydration, hydroelectrolyte changes, esophageal rupture and increased intracranial pressure [5,8].
However, despite the advancement of the modern anesthetic in the management of PONV, it remains a major problem for participants in postoperative care unit with an incidence ranging from 20-30% [3]. Moreover, children especially above 3-years-old experienced highest (40%) incidence of PONV than the other age group of children [4]. In higher risk populations, which have been mentioned in the above, who are undergoing surgeries such as ENT, Eye, Laparoscopic and others, the incidence was approximates 80% [9]. Furthermore, if prophylactic antiemetic was not given for participants undergoing ENT surgeries of Adenotonsillectomy and Middle ear, the incidence of PONV would be up to 36-76% and 80% respectively [5,10]. Hence, ENT surgery cases are relatively healthy and ambulant without the occurrence of nausea or vomiting that make them sick and delay from hospital discharge [11]. Therefore, putting in consideration the impact of its occurrences, the aim of this study was to assess the incidence and risk factors of PONV in participants after ENT surgeries in Orotta Medical Surgical National Referral Hospital.
Prospective quantitative hospital based study was conducted. The study site was department of ENT in Orrota National Referral Hospital in Asmara, Eritrea. The ENT department is the only ENT referral center in the nation, contains 29 inpatient beds for all types of ENT cases that includes medical as well as surgical treatments.
All participants scheduled for elective surgery from all ages including; pediatric and adult, and those who fit the inclusion criteria (participants scheduled for elective ENT surgery and willing to participate as well as participants under the ASA classification I and II) were included in this study. The period of the study was from December 1, 2017 to February 28, 2018.
All (n = 125) participants who were undergoing elective ENT surgery were taken in the study.
A structured questionnaire was used for data collection tool. Input from experts including the authors and statisticians fuelled the quality of the questionnaire. The questionnaire was prepared in English and translated into the native Tigrigna language and back translated to maintain its original meaning. In order to assure the understandability of the questionnaire by the participants, a pre-test was done. Finally arrangement of the questions was made after the pretest. Before commencement of data collection, training was given to the data collectors for 5 days. Then data was collected preoperatively, intraoperatively and postoperatively. The questionnaire contains three sections; in which the first part has fixed participant characteristics predictive of PONV, second part contains the preoperative assessment with details of the type of surgery and induction of anesthesia and the last portion consists of postoperative outcome under observation. The intervals of assessment were 0-2 hours, 2.01-12 hours and 12.01-24 hours; the first 2 hours spent in recovery and the remaining hours mostly in the ward. The data was recorded by the experienced ENT anesthetists and completeness of it was reviewed by the corresponding author. The patents' were interviewed preoperatively 30 minutes before surgery. Intraoperative anesthetic techniques and drugs were recorded. Postoperatively, participants were observed for the presence of vomiting and asked for the feeling of nausea and retching.
All participants received balanced anesthesia. All adult participants were not given any premedication drugs but few of the paediatric received opioids. Dexamethasone and atropine were given as premedication drug during the induction time of anesthesia. Anesthesia was induced with sodium thiopental or propofol and fentanyl at clinically required doses. Few paediatric participants were induced by halothane. Tracheal intubation was facilitated after suxamethoniumorrocuronium. Then anesthesia was maintained on O2, Air and isoflurane or halothane. Rocuronium, at clinically required dose, was used as a muscle relaxant. Ventilation was done with IPPV and few participants were under spontaneous ventilation. Neuromuscular block was antagonized using neostigmine and atropine in standard doses and tracheal extubation was done when the participants were fully awake. Postoperatively, for those participants who had nausea and vomiting metochlopramide was given.
The socio-demographic variables were; age, sex, BMI, smoking. The clinical parameters were; drugs, site of surgery, duration of surgery, NGT presence, pain, fasting time, early feeding, and anesthetic techniques. The outcome variable was postoperative nausea and vomiting.
Content validity of the questionnaire was checked by expert's opinion from the department of anesthesia and ENT Clinicians. A pretest was performed to ascertain the comprehension and understandability of the questions.
Data was coded and entered into computer software SPSS version 22 and was cleaned. Descriptive analysis for socio-demographics was done using percentage and mean (SD) or median (IQR) depending on normality. The background information, preoperative, intraoperative and postoperative variables were described using frequency and percentage. Mann Whitey U test was used to compare duration of fasting, duration of ventilation via face mask, and time of first oral intake with PONV. Possible association of the occurrence of PONV and the identified risk factors was performed using chi-square test. Relative risk (95%CI) of PONV was computed for various predictor variables. Adjusted relative risk was also computed after identifying the risk factors found to be significant at univariate level. P ≤ 0.05 was taken as significant value.
There were 185 participants in the ENT ward, 30 didn't give consent, 10 drop out, 20 under workup. Finally 125 participants set for analysis.
A total of 125 participants have done ENT surgeries from December 1, 2017 to February 28, 2018. The median age of the study participants was 12 years (IQR = 28, Min = 1 Max = 75) and 72 (57.6%) were pediatrics and 53 (42.4%) adults. Sixty eight (54.4%) of the participants were males and 57(45.6%) females. The WHO (World Health Organization) classifications of BMI were used for participant's > 15-years-old and were categorized into underweight, normal, overweight, and obese. According to Orrota National Referral Hospital, 15-years-old were treated as paediatric. Out of the paediatrics, 3 (2.4%) participants were underweight, 59 (47.2%) normal, and 10 (6.9%) overweight. Similarly, age > 15-years-old were considered as adults. Out of 53 adults, 15 (12%) participants were underweight, 26 (20.8%) normal, 11(8.8%) over weight and 1(0.8%) obese (Table 1).
Table 1: Socio-demographic characteristics of the study participants (n = 125). View Table 1
Of those 125 enrolled participants, 4 (3.2%) had history of smoking, 13 (10.4%) history of motion sickness and 1 (0.8%) history of previous PONV. The majority 89 (71.2%) of the participants had done throat surgery followed by nose surgery 30(24%) and ear surgery 6 participants (4.8%). Almost four fifth (n = 102) of the participants were classified under ASA classification I, while one fifth (n = 23) were classified under ASA II. Furthermore, 6(4.8%) participants had concurrent medical illness which includes diabetes mellitus, cardiac disease, gastric ulcers, down-syndrome and HIV. The duration of fasting before operation ranged from 4 hours to 24 hours with mean fasting time of 12.7 hours (SD = 3.36). Out of the total 125 participants four (3.2%) participants were given opioids as premedication (Table 2).
Table 2: Pre-operative assessments of the participants (n = 125). View Table 2
Ventilation via face mask was done in 120 participants (96%) and among these participants 57.6%, 34.4%, 3.2%, and 0.8% were ventilated for less than 5 minutes, 5-10 minutes, 10-20 minutes, and greater than 20 minutes respectively. All (100%) participants had received fentanyl during induction and additionally 39 (31.2%) during surgery. Fifty eight (46.4%) of the participants took antiemetics while the remaining didn't. The only type of anti-emetic given was dexamethasone during induction period but not during intraoperative and at the end of surgery.
Those participants who were given propofol and sodium thiopental as induction agents were 82.4% and 17.6% respectively. Thirty (24%) of the participants took Halothane as induction agent. Fifty six (44.8%) participants were given suxamethonium, 69 (55.2%) NDMR (rocuronium), 2 (1.6%) participants were given both suxamethonium and rocuronium, and only 2 (1.6%) participants were not given any muscle relaxant. The duration of fasting period ranged from 4 hours to 24 hours with mean fasting time of 12.7 hours (SD = 3.36) (Table 3).
Table 3: Induction of anesthesia and intraoperative drugs (n = 125). View Table 3
Out of the two inhalational agents available in the ENT department of Orrota National referral hospital 117 (93.6%) of the participants received Isoflurane for maintenance and the remaining 8 (6.4%) tookhalothane. The most frequent mode of ventilation used was IPPV (intermittent positive pressure ventilation) in 117 (93.6%) participants while spontaneous ventilation only in 8 (6.4%) (Table 4).
Table 4: Maintenance of anesthesia (n = 125). View Table 4
Nineteen (15.2%) of the participants took combination of neostigmine and atropine and of which 11 (57.9%) took ≤ 0.04 mg/kg while 8 (42.1%) > 0.04 mg/kg. The median duration of surgery was 30 minutes (IQR = 25). Sixty six (52.8%), 45 (36%), and 14 (11.2%) of the participants had surgery for < 30, 30-60, and > 60 minutes respectively. On the same token, the median duration of anesthesia was 35 minutes (IQR = 33). The percent of participants who took anesthesia < 30, 30-60, and > 60 minutes were 44.8%, 40%, and 15.2% respectively. Nasogastric tube (NGT) was not inserted in to all participants (Table 5).
Table 5: Reversal of anesthesia and emergency of the participants (n = 125). View Table 5
In the postoperative period only 6 (4.8%) participants were given a rescue anti-emetic while119 (95.2%) none. The only anti-emetic drug given was metoclopramide. During post-operative period 63 (50.4%) of the participants had pain while 62 (49.6%) had no pain. Eighty two (65.5%) of the participants took their first oral intake between 30 minutes and 1 hour while the remaining 13.6%, 6.4%, and 14.4% between 1.1 hours to 2 hours, 2.1 hours to 3 hours, and 3.1 hours and above, respectively. Antibiotics were given postoperatively to 112 (89.6%) participants. The types of antibiotics given were Amoxicillin (n = 77, 61.6%), Metronidazole (n = 6, 4.8%), Co-trimoxazole (n = 2, 1.6%), and others (n = 34, 27.2%) (Table 6).
Table 6: Post-operative evaluation of the participants (n = 125). View Table 6
The overall incidence of PONV after ENT surgery with in a period of 24 hours was 32.8%. Out of the occurrence of PONVs, the highest percentage was observed in vomiting (n = 20, 48.8%) while nausea, retching as well as nausea and vomiting together had 17.1% (Figure 1).
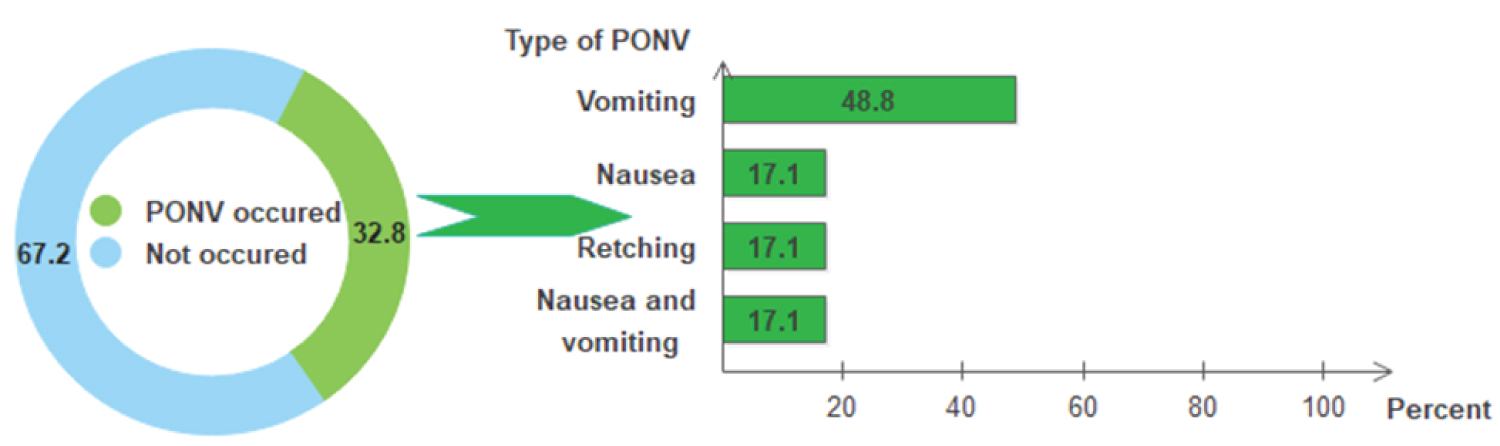 Figure 1: The incidence of PONV and its types (n = 125).
View Figure 1
Figure 1: The incidence of PONV and its types (n = 125).
View Figure 1
In order to observe the presence of PONV, participants were followed for 24 hours postoperatively. The follow up period was divided in to three periods; 0-2, 2.01-12 and 12.01-24 hrs for each outcome. Six (85.7%) of the ‘only nausea' events occurred between 0-2 hours while only 1 (14.3%) had experienced between 2.01 and 12 hours. None of the participants suffered retching and nausea (during nausea and vomiting) after 2 hours. The occurrence of ‘only vomiting' during 0 to 2 hours, 2.01 to 12, as well as 12.01 to 24 hours was 65%, 30%, and 5% respectively. During the presence of PONV, initial symptom of nausea was observed in the first 2 hrs among 7 (100%) participants. In a similar way, the occurrence of vomiting in the immediate 2 hrs was 85.7%. The remaining 14.3% had vomiting with in the period of 2.1 to 12 hrs (Table 7).
Table 7: Time period for occurrence of PONV (n = 125). View Table 7
Socio-demographic characteristics of the participants as risk factors: Regarding the socio-demographic characteristics of participants, Gender and BMI were not a risk factors for the occurrence of PONV (p > 0.05). However, age (RR = 1.71, 95%CI: 1.00-2.90) was significantly associated with the risk of occurrence of PONV (Table 8).
Table 8: Socio-demographic characteristics of the participants as risk factors (n = 125). View Table 8
Preoperative assessment of the participants as a risk factor: History of smoking, history of previous PONV, type of surgery, ASA classification,Fasting time, opioids given as pre-medication and presence of concurrent medical illness were not found as risk factors for the occurrence of PONV (p > 0.05). However history of motion sickness (RR = 2.78, 95%CI: 1.82-4.24) were significantly associated with the risk of occurrence of PONV. Participants with history of motion sickness had 2.78 times higher risk than those without previous history (Table 9).
Table 9: Preoperative assessment as a risk factor (n = 125). View Table 9
Induction of anesthesia and intraoperative drugs as risk factors: The induction agents of anesthesia and intraoperative drugs as risk factors namely, usage of inhalational induction (RR = 1.02, 95%CI: 0.57-1.83), ventilation via face mask (RR = 0.81, 95%CI: 0.27-2.45), muscle relaxants (RR = 1.12, 95%CI: 0.68-1.86), anti-emetic (RR = 1.48, 95%CI: 0.89-2.45) and fentanyl administration period (RR = 1.27, 95%CI: 0.76-2.12) were not contributors to the risk of PONV. However, the study found out that the type of hypnotic agent used (RR = 1.72, 95% CI: 1.03-2.87) was a risk factor of PONV. The proportion of participants who had PONV after taking sodium thiopentone (50%) was significantly higher than the proportion of participants who had PONV after taking Propofol (29.1%) (Table 10).
Table 10: Induction of anesthesia and intraoperative drugs (n = 125). View Table 10
Maintenance of anesthesia as risk factors: Maintenance of anesthesia namely types of inhalational agent and mode of ventilation was investigated and they were found to be insignificant to contribute as risk factor for PONV (Table 11).
Table 11: Maintenance of anesthesia (n = 125). View Table 11
The duration of surgery and anesthesia were investigated and had no significant impact on the occurrence of PONV (p > 0.05). Dose of neostigmine and atropine (RR = 1.09, 95%CI: 0.45-2.63) were not risk factors for PONV. However, administration of drugs such as neostigmine and atropine (RR = 1.80, 95%CI: 1.07-3.03) were a risk factor for causing PONV. The proportion of participants who received neostigmine and atropine (52.6%) were significantly higher than those who did not (29.2%) (Table 12).
Table 12: Reversal of anesthesia and usage of antagonists for muscle relaxation (n = 125). View Table 12
The risk for PONV was found to be higher (RR = 2.38, 95%CI: 1.34-4.22) in those participants who had pain during the post-operative period than in those who had not. However, the duration of time until the first oral intake (RR = 1.13, 95%CI: 0.66-1.95), the fact that antibiotics were given or not (RR = 1.47, 95%CI = 0.53-4.10), and the type of antibiotic (RR = 1.56, 95%CI: 0.77-3.14) were not significant risk factors for the occurrence of PONV (Table 13).
Table 13: Post-operative evaluation as risk factors (n = 125). View Table 13
The comparison of the time of onset of PONV have revealed that there was significantly higher presence of PONV at the time period 0-2 hours after anaesthesia had ended than 2-24 hours (p < 0.001) (Table 14).
Table 14: Time of onset of PONV (n = 40). View Table 14
Postoperative nausea and vomiting are among the adverse events following surgery, anesthesia and opioid analgesia which leads to participant distress, prolonged hospitalstay and increased cost [12]. The incidence of PONV remains still high despite the presence of advanced multimodal approach such as new antiemetic medications, less emetogenic anesthetic techniques, intravenous hydration and adequate painkillers [5]. Similarly, in this study the overall incidence rate of PONV after ENT surgery is 32.8%. This can be explained by the large number of paediatric participants, as the incidence of vomiting after tonsillectomy may approach 81% [5]. However, a low incidence rate of PONV after ENT surgeries was reported [13], which was associated to small sample size of the participants.
Although a large number of participant-related factors have been evaluated, the actual influence of specific surgical procedures on the risk for PONV continues to be a highly debated topic. So, it is a multifactorial distressing event following surgery and anesthesia second to postoperative pain. The main causes of PONV are classified as participant, preoperative, intraoperative, anesthetic, surgical and postoperative factors.
Regarding the participants risk factor the paediatric age group which encompasses 57.6% of the total participants had statistically significant increase in the incidence of PONV (RR = 1.78, 95% CI 1.00-3.15). These results are supported with other study done in Thailand, India, and USA [14-16].
In regard to gender as a factor, this study reveals opposite results to the most literature carried out at various times in which males were found out to have higher risk of PONV (M = 39.7% versus F = 24.6%). However, the study done by Lubis and Kristiantian [17] shows similar results in which male participants had higher percentage of PONV which was 62.3% to 37.7%. The reason why male participants in this study had higher percentage of PONV may be due to the majortiy of the participants were paedatric (57.6%) and more than 60 years [3,18-21]. However, in this study BMI, cigarette smoking, history of previous PONV, history of concurrent medical illnesses, use of muscle relaxants and administration of antibiotics were not risk factors for PONV.
But, the participants with history of motion sickness had strong statistically significance for the occurence of PONV which was almost three times higher than participants with no history of motion sickness (RR = 2.78, 95%CI: 1.82-4.24). This study correlates with previous studies in which participants with history of motion sickness are reported to have low threshhold for nausea or vomiting and have a higher occurrence of PONV [3,6].
Even though the types of surgery were not statistically significant for the occurrence of PONV, participants who had to undergo throat surgery had higher risk for PONV (37.1%), followed by nasal surgery (23.3%) and ear surgery (16.7%). Since the throat surgery was done mostly in the paediatrics, this may be the reason why it had higher percentage of PONV than the other surgeries.
Our study did not show any significance in the incidence of PONV with the duration of fasting.
However, other studies reported that prolonged duration of fasting led to dehydration which may be a precipitating factor for PONV [7,22].
In this study most of the participants (57.6%) were ventilated for less than 5 minutes, and it was not significant factor for the occurrence of PONV. These results are unsatisfying as the most participants were ventilated for less than 5 minutes, which was not enough to cause gastric dilation, which would increase PONV. However, the longer time of ventilation via face mask is the higher the risk of PONV [23,24].
The use of sodium thiopental as induction agents had significant increase in the incidence of PONV (RR = 1.72, 95% CI 1.03-2.87) as compared to propofol. Propofol has been recommended for day care procedures, because it promotes fast recovery and has anti-emetic property [11,20]. In the study done in India by Abhijeet Rajan [11], the incidence of PONV during the first 24 hours was recorded to be less after propofol administration than metoclopramide, 50% to 70%, respectively. Therefore, sodium thiopental induction was associated with a greater incidence of PONV than induction using Ketamine hydrochloride (p = 0.04) [20].
Participants who received fentanyl at induction, as well as additional use intraoperatively were not statistically significant for the incidence of PONV. However, other study showed that intraoperative and post-operative opioid administration increases the risk of PONV in a dose dependent manner. Opioid reduce muscle tone peristaltic activity, there by delay gastric empting, induce distention and triggering the vomiting reflex [3,18,22].
Interestingly participants who received dexamethasone, had higher risk for PONV (39.7% versus 26.9%) than who did not receive. This study showed similar results with study done in Singapore (OR = 1.465, p = 0.042) [25]. But these results are also contrary to the other studies which stated that dexamethasone may be beneficial because of direct anti emetic effects, reducing post-operative pain as well as the need for pain relief. “It's true that low dose dexamethasone may be required for PONV prophylaxis than for pain relief” [11,26-28].
The possible explanation that the participants who received dexamethasone had higher percentage for PONV, is that the majority of the participants were exposed to more risk factors than the others. The majority of the participants who received dexamethasone were paediatrics. According to this study the group of participants who had to undergo throat surgery such as; Adenoidectomy, Tonsillectomy & Adenotonsillectomy were having higher risk for the occurrences of PONV.
Volatile agents may increase PONV by decreasing serum level of cannabinoids neurotransmitters that act on cannabinoid-1 and transient receptor potential vanilloid-1 receptor to suppress nausea and vomiting [3,18]. Likewise, isoflurane was the commonest inhalational agents (93.6%) used for maintenance of anesthesia. It was found to be a risk factor for PONV compared to halothane (34.2% versus 12.5%), even though it was not statistically significant. The use of volatile anesthetics is the single most important factors for predicting emesis in the first 2 post-operative hours.
In this study intermittent positive pressure ventilation was the common mode of ventilation (93.6%) used for maintenance of anesthesia and had a higher occurrence of PONV (33.3% versus 25%) than spontaneous mode of ventilation. In contrary to our study, a study done by McCracken, et al. (2008), showed that the use of spontaneous ventilation had a higher incidence of PONV. The plausible reason could be that a higher minimum alveolar concentration (MAC) of volatile agents is needed with application of spontaneous ventilation than IPPV (Intermittent positive pressure ventilation) so creates gastric dilation.
In our study administration of neostigmine and atropine was statistically significant for the incidence of PONV (RR = 1.80, 95%CI 1.07-3.03). Similarly in another study, antagonism of residual neuromuscular block with a mixture of neostigmine and atropine increase emesis despite the anti-emetic action of atropine [20]. The use of neostigmine had higher incidence of PONV in the post-operative period and high anti-emetic uses in 24 hours of monitoring [29]. In the contrary neostigmine does not increase the risk of vomiting in the early, late or over all post-operative period and there is insufficient evidence to conclude that it leads to a clinically important increase in the risk of post-operative nausea [30,31]. In the same token, higher dose more than 0.04 mg/kg of neostigmine and atropine drugs does not associated to the risk of PONV. While in other studies the use of high doses of antagonist of muscle relaxants (more than 0.04 mg/kg) had been shown to increase the risk of PONV [20,29].
The duration of anesthesia which is closely linked to the duration of surgery, can help to predict the participants risk of PONV, since the duration of anesthesia describes the participants exposure to emetogenic stimuli like volatile anesthetic and intraoperative opioids [3]. Thus, the longer the surgical stimulation is the higher the risk of PONV. This is also corresponds to the duration of anesthesia. Each 30 minutes increase in duration of surgery lead to increases risk of PONV by about 18%. Surgeries with duration of more than 60 min are associated with higher outcome of PONV [15,16,21].
Most of the participants (50.4%) experienced postoperative pain. The presence of PONV in relation to the experience of pain revealed to be statistically significant. The risk of PONV in those participants who had pain was 2.38 times higher than those without. This study is supported by the results reported in Kenyatta Hospital that 60% of the participant's encountered pain and showed statistically significant association toward the outcome of PONV [32]. The untreated pain happening intraoperative and post-operative increases the chance of PONV incidence. Relief of pain is often associated with the release of nausea, though the use of opioid analgesics may exacerbate the risk because of their known emetic potential. If pain is not effectively managed nociceptor activation may produce similar change in the area postrema and chemoreceptor trigger zone (CTZ) thereby lowering the threshold for vomiting [33,34].
Time of first oral intake as a contributor factor of PONV revealed slight difference. However, first oral intake less or equal to 60 minutes (34.1%) had a higher incidence of PONV than those who ate after 60 minutes (30.2%). Kovac, et al., [22] also found out that first oral intake has strong associations with PONV. Therefore, the presence of PONV in the earlier period of postoperative was strongly significant than late occurrences.
Presence of nausea in the paediatric participants is difficult to measure so instead retching and vomiting were taken as parameters of measurement.
The study concluded that the overall incidence of PONV in ENT Orrota National Referral Hospital was 32.8%. The risk factors that have been shown increased incidence of PONV were age less than 15-years-old, history of motion sickness, use of thiopental as induction agent, administration of combined neostigmine and atropine as agents, and presence of pain postoperatively.
Ethical permission was obtained from the research ethical committee of the College of Health Sciences and Ministry of Health of Eritrea. The purpose, the process, potential benefit and harm of the study was explained to the participants clearly. They were guaranteed to participate or to withdraw from the study at any time during the process of the study. They were assured that confidentiality was strictly maintained and that all data obtained was tightly kept and that there was no extra price involved if they agreed to participate. The study did not negotiate the standards of care of ENT surgical participants in regards to treatment and prevention of PONV as this study did not forbid usage of antiemetic. Refusal of consent did not lead to discrimination in care.
The authors would like to thank to the staff of Asmara College of Health Sciences and the Ministry of Health office for their cooperation and support in conducting the study. Special thanks goes to Mr. Amanuel Hadgu, Dr. Simon Habte and staff of the ENT department for their valuable contribution throughout the study and above all our appreciation goes to the study participants who gave their consent to participate in the study.
Not applicable.
All the data are kept properly and can be retrieved if needed.
All the authors (PKY, GGB, SM, MBM, and EHT) involved in designing and coordination of the study, analysis and interpretation of data, revising the manuscript critically for important intellectual content, drafting and submission of manuscript. The data was collected by the hospital anesthetists under supervision of the PKY. All authors read and approved the final manuscript.
Not applicable.
The authors declare that they have no any competing interests.