COVID-19 is an emergent disease with reported neurotropism and neuroinvasion, although its pathophysiology is not yet understood. We present the newly discoveries and hypothesis for SARS-Cov-2 neurological infection.
SARS-Cov-2, COVID-19, Anosmia, Hypogeusia, ACE2
Neurotropism is a well established characteristic in coronaviruses infections in humans and animals [1-3]. With the emergence of the new coronavirus SARS-CoV-2, its neurotrophic activities begin to attract attention, with a study proposing an effect in the respiratory distress caused by neuroinvasion [4].
A study proposed two possible neurotrophic paths for the SARS-CoV-2 -- gaining access to the central neural system (CNS) via general circulation disrupting the blood brain barrier [5] or via the olfactory bulb that intimately related with the cribriform plate and so giving the virus access to the CNS [5]. The last one is a common route for respiratory virus to enter the CNS [2] and is possibly related to hyposmia in an early state of the disease (Figure 1) [5].
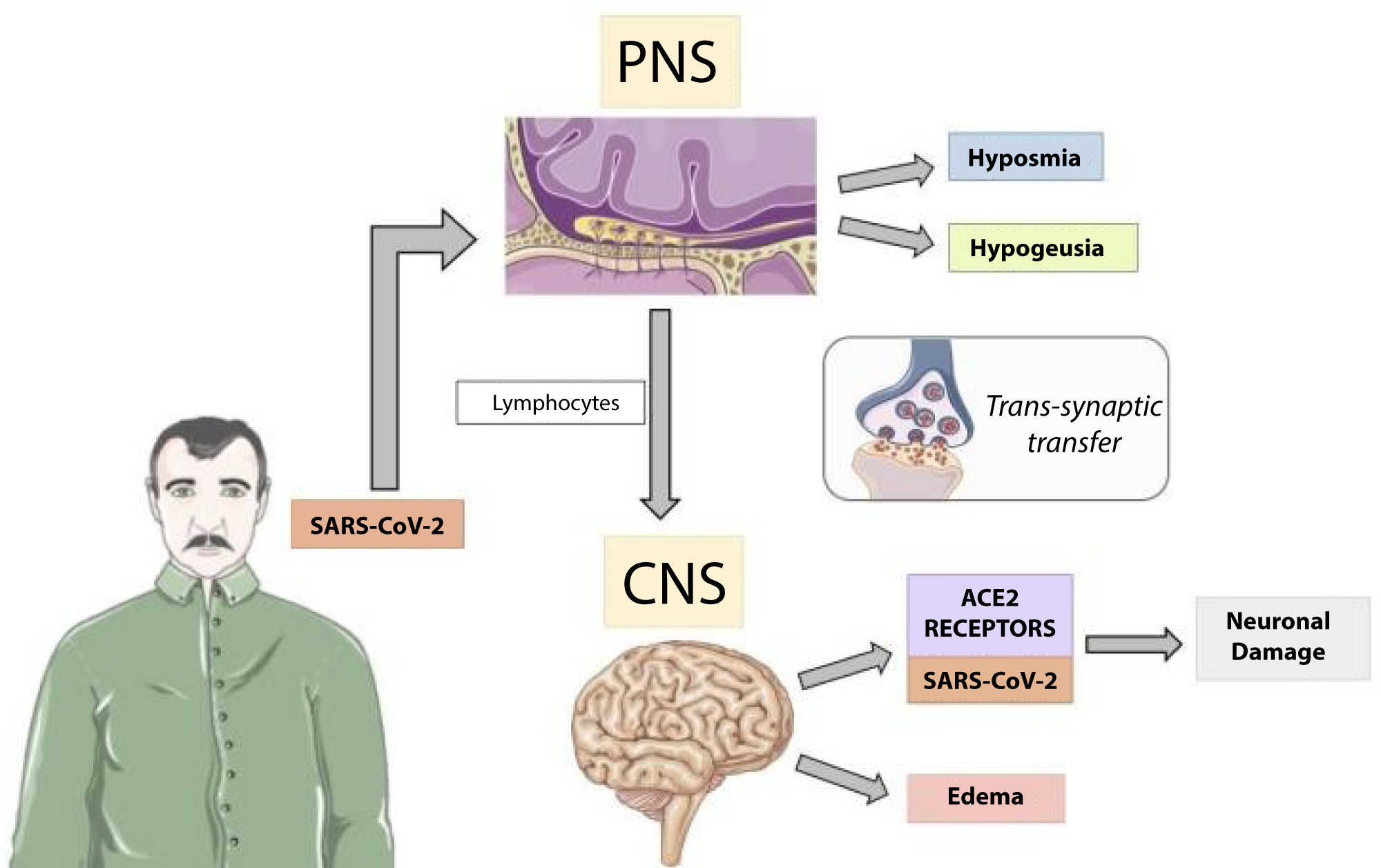 Figure 1: The image represents the SARS-CoV-2 gaining access to the olfactory bulb and then, via transsynaptic transfer, accessing the Central Nervous System (CNS), especially in patients with lower lymphocytes count [4,6]. It progresses with CNS symptoms, infecting neurons by binding in Angiotensin conversion enzyme 2 receptor (ACE2) [5]. Images acquired at: http://smart.servier.com/. View Figure 1
Figure 1: The image represents the SARS-CoV-2 gaining access to the olfactory bulb and then, via transsynaptic transfer, accessing the Central Nervous System (CNS), especially in patients with lower lymphocytes count [4,6]. It progresses with CNS symptoms, infecting neurons by binding in Angiotensin conversion enzyme 2 receptor (ACE2) [5]. Images acquired at: http://smart.servier.com/. View Figure 1
These assumption correlates with clinical findings in a study conducted by Mao, et al. that presents 218 confirmed patients with SARS-CoV-2 infection - 53 (24.8%) of those who had CNS involvement were related to more severe disease and laboratory differences, especially lower lymphocytes count, compared to patients without CNS involvement [6]. A similar correlation showing lower lymphocytes count was found in children with neurological human CoV infection compared to respiratory human CoV patients [7].
Patients with peripheral nervous system (PNS) symptoms had hyposmia and hypogeusia and presented no laboratory differences compared to patients without PNS involvement [6], indicating that these symptoms can be prodrome of a more serious neurological involvement - although more data is needed - or the low lymphocytes and immune dysfunction are needed for a CNS infection.
Recently, the first case of encephalopathy associated with SARS-COV2 infection described was published. The patient rapidly progressed from fever and cough to an altered mental status, headache and unresponsive to verbal commands, with no alterations in the liquor, suggesting that the blood brain barrier was not affected in the patient [8].
In conclusion, SARS-Cov-2 infection is an emergent disease whose pathophysiology is not yet understood, but neurological involvement is already established. Hyposmia and hypogeusia have been related in patients with COVID-19 and must be considered as symptoms of SARS-Cov-2 infection, even if patients with those symptoms were previously considered asymptomatics.
No financial support.
No material support.
All authors declare that there are no conflicts of interest.