

International Journal of Clinical Cardiology
Parameters of Mitral Deformability in Patients with Functional Mitral Regurgitation
Kammoun I*, Marrakchi S, Zouari F, Fersi I, Ibn Elhaj Z, Mokrani S, Added F and Kachboura S
Department of Cardiology, Ariana Hospital, Tunisia
*Corresponding author: Ikram Kammoun, Professor, Department of Cardiology, Ariana Hospital, Tunisia, Tel: 0021698644048; E-mail: kammounikram@yahoo.fr.
Int J Clin Cardiol, IJCC-1-008, (Volume 1, Issue 2), Research Article; ISSN: 2378-2951
Received: October 21, 2014 | Accepted: November 19, 2014 | Published: November 21, 2014
Citation: Kammoun I, Marrakchi S, Zouari F, Fersi I, Ibn Elhaj Z, et al. (2014) Parameters of Mitral Deformability in Patients with Functional Mitral Regurgitation.Int J Clin Cardiol 1:008. 10.23937/2378-2951/1410008
Copyright: © 2014 Kammoun I, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Functional mitral regurgitation (FMR) is one of the common and severe complications in patients with dilated cardiomyopathy. Then determinants of degree of FMR must be more defined.
Purpose: We sought to determine a cut off value of the tenting area and the coaptation depth which correlate with the severity of the FMR.
Methods and results: We enrolled prospectively 96 patients (71 males; age 57 + 13 years) with left ventricular (LV) dilation and systolic dysfunction (LV ejection fraction =40%) in sinus rhythm.
The severity of the FMR was determined by the proximal isovelocity surface area method allowing calculation of the effective regurgitant orifice (ERO) and regurgitant volume (RV). An ERO = 20mm2 and a RV =30ml/beat defined significant FMR.
We evaluate mitral deformity by measuring tenting area (TA) and coaptation depth (CD) from apical 4-chamber view at mid-systole. FMR was significant in 26 cases.
TA correlated positively with ERO (r=0,58; p< 0.01) and with RV (r=0,87; p< 0,01). Cut off value of TA at 1,5cm2 diagnosed significant FMR with a sensitivity of 84% and a specificity of 61%.
Coaptation depth correlated positively with tenting area (r=0,4, p< 0,01). However, there is no correlation between CD and the severity of mitral regurgitation.
Conclusions: Tenting area, an echocardiographic parameter of mitral deformability, is correlated positively with the severity of FMR. Minimal TA of 1,5cm2 identified significant FMR with a sensitivity of 84% and a specificity of 61%.
Introduction
The negative impact of FMR on survival has been well documented, and a graded relationship between the severity of MR and mortality has been repeatedly demonstrated [1,2].
Although global LV dilation and sphericity has been attributed to FMR by alteration in mitral annulus and subvalvular apparatus, and ultimately incomplete coaptation, but local LV remodeling and mitral valve deformation seems to be more important determinants of FMR severity.
It is useful then to determine echocardiographic determinants of FMR severity in patients with LV dysfunction.
Methods
Patients: Inclusion criteria were: dilated cardiomyopathy with systolic LV dysfunction (LVEF less than 40%), structurally normal cardiac valves and sinus rhythm. Criteria of non inclusion were organic valvular disease, acute myocardial infarction and atrial fibrillation or flutter.
Echocardiographic measurements: All patients underwent complete transthoracic echocardiography for assessing MR severity and measuring the indices of global and local LV remodelling as well as mitral deformation indexes. Exams were performed by the same operator using Aloca 5000 or VIVID E9 (GE).
Complete 2D and colour Doppler flow imaging were performed according to guidelines of the ASE, to determine severity of the mitral regurgitation [3].
ERO and MR volume assessed by PISA method (Figure 1). ERO = 0,2cm2 and RV =30ml/beat defined as significant FMR.
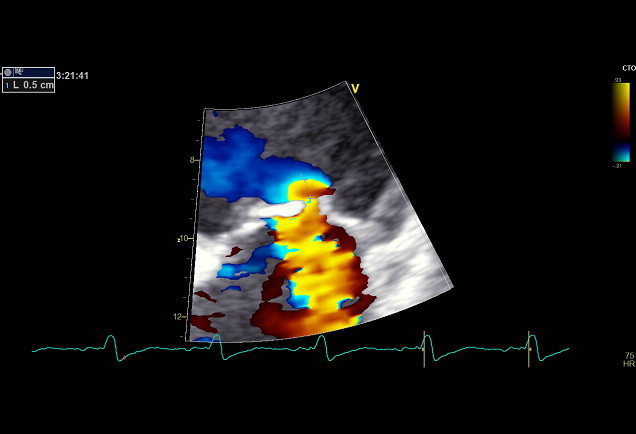
Figure 1: ERO and MR volume assessed by PISA method.
View Figure 1
LV dimensions were measured at diastole and systole (LVEDD, LVESD) in parasternal long axis view. LV volumes and EF were obtained by biplane Simpson's method.
To quantify the mitral deformity, we measured the tenting area and the coaptation depth. TA was defined as the area enclosed between mitral leaflets and annular plane (Figure 2). CD was defined as the distance between leaflet coaptation and the mitral annulus plane (Figure 3).
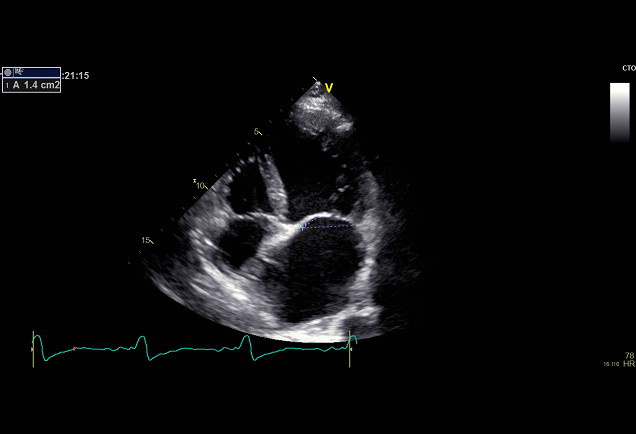 Figure 2: Tenting Area (TA)- Area enclosed between mitral leaflets and
annular plane.
View Figure 2
Figure 2: Tenting Area (TA)- Area enclosed between mitral leaflets and
annular plane.
View Figure 2
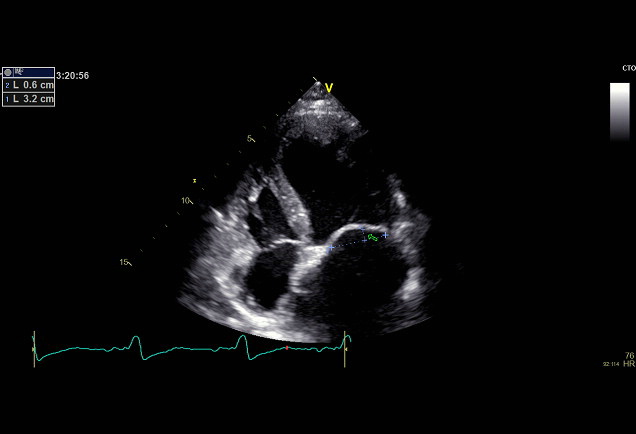 Figure 3: Coaptation Depth (CD)- Distance between leaflet coaptation and
the mitral annulus plane.
View Figure 3
Figure 3: Coaptation Depth (CD)- Distance between leaflet coaptation and
the mitral annulus plane.
View Figure 3
These parameters were obtained at mid-systole in the apical 4-chamber view.
Statistical analysis: Data was expressed as mean + SD. A value of p = 0,05 was considered significant. Group comparison of continuous variables was performed by Pearson's t-test.
Ta values were categorized according to the cut-off ROC analysis as a predictor of significant FMR.
Results
Of total 96 patients enrolled in this study, 71 (74%) were male. Mean age was 57 + 13 years. 17 patients were categorized as having an ischemic cardiomyopathy (ICM) by documented history of infarction and/or coronary angiography.
Left ventricular dysfunction was severe (EF 31 % + 8 %, range 10 % to 40 %). Mean end-diastolic diameter (EDD), end-diastolic volume (EDV), end-systolic diameter (ESD) and end-systolic volume (ESV) of LV were: 68 + 8mm, 161 + 52ml, 57 + 9mm and 111 + 42ml, respectively.
70 patients (73%) presented with mild regurgitation, 26 patients (27%) with moderate to severe functional mitral regurgitation. Mean ERO and RV were respectively 16 + 9mm2 and 23 + 11ml/beat.
Tenting area, as mitral deformation indice, increased significantly with higher degree of FMR (P< 0.001) (Figure 4).
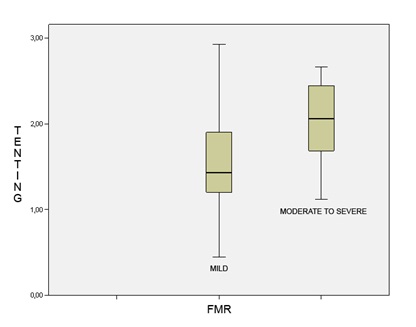
Figure 4: Tenting area and severity of mitral.
View Figure 4
A cut off value of Ta 1,5cm2 diagnosed significant FMR with a sensitivity of 84% and a specificity of 61%.
Coaptation depth was positively correlated to Ta (r=0,4, p< 0,01). (Figure 5) However, there was no correlation between coaptation depth and the severity of FMR (r=0, 13; p=0,214).
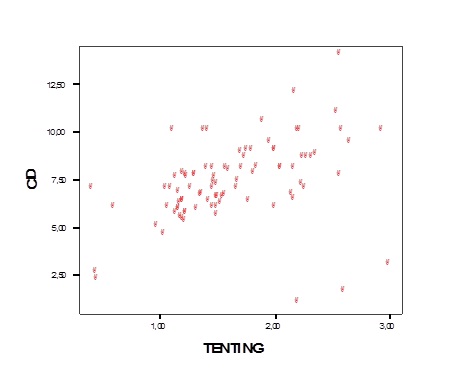
Figure 5: Correlation between tenting area (Ta) and coaptation depth (CD).
View Figure 5
In addition, there was no significant relationship between FMR severity and LVEF (r=-0,08; p=0,47 with ERO and r=0,03, p=0,78 with RV).
Discussion
The papillary muscle displacement stretches the body of the leaflet by pulling the stay cord, and apical displacement of the leaflets (i.e., incomplete mitral leaflet closure) induces mitral deformity and functional MR.
The lack of correlation between EF and the severity of the FMR indicates that systolic dysfunction is not mainly responsible for functional MR.
This data was found in our study with no significant relationship between FMR severity and LVEF.
In the previous reports using echocardiogram, several factors were known to cause FMR independently, including LV dilation, LV sphericity, apical and posterior displacement of papillary muscle, and LV dysfunction [4-9].
In early experimental studies, FMR has been attributed to global LV dilatation or sphericity. Later, animal studies have suggested complex alterations of spatial relationship between left ventricle and mitral apparatus to induce functional MR [6,7].
A previous report, using by trans-esophageal echocardiography, noted the importance of CD for determining surgical strategy (mitral repair or replacement) in patients with dilated cardiomyopathy [10]. Although the strong correlation between TA and CD, TA may be affected by annular dilation, but not for CD. Therefore, we used CD in addition to TA to estimate mitral deformity.
Few studies have defined a cut off of tenting area correlated with the severity of FMR.
A recent study [11] has defined a cut off of tenting distance at 0,45cm to predict mild FMR and 2,35 cm to predict severe FMR with 80% probability.
A more recent study [12] concluded that Tenting area accurately reflects the degree of FMR at a cut-off value of 3.4cm 2 with 82% sensitivity and 77% specificity.
In our study, a lower cut-off value of Ta 1,5cm2 was found which diagnosed significant FMR with a sensitivity of 84% and a specificity of 61%.
This difference between our study and Karaca's study [12] may be explained by:
i, The differences in methodology: We have used apical 4-chamber view to evaluate Ta and CD as Nagasaki'ss study and in 3D studies [13], whereas in Karaca's study, these parameters were measured in parasternal long axis view.
ii, And by the proportion of ischemic cardiomyopathy included in our study, but all patients in Karaca's study [12] had non ischemic cardiomyopathy.
Some studies [14,15] demonstrated differences between ICM and non-ICM in echocardiographic parameters determining MR severity.
Kwan' study [15], a real-time three-dimensional echocardiography study, showed that tenting area was larger in patients with DCM.
More recently, 3D echocardiography was used to evaluate mitral valve tenting volume (TnV) as a clinical parameter of FMR. Yu's study [16] found in 31 patients with LV systolic dysfunction, that minimal TnV was the only independent determinant of ERO. The cut off value of 3.9 ml diagnosed significant FMR with high sensitivity and specificity.
When compared with 2D TEE, 3D offline reconstructions of the mitral valve provide almost similar values for the tenting area and the coaptation depth [17].
Study limitations
We could not estimate the association of parameters of mitral deformability (Ta and CD) and cardiac events because no follow-up was available.
Conclusion
Degree of LV enlargement and dysfunction were not primary determinants of FMR severity, therefore a tenting area>1.5cm2, a parameter of mitral valve apparatus deformation, predict a significant FMR with a good sensitivity.
References
-
Levine RA, Schwammenthal E (2005) Ischemic mitral regurgitation on the threshold of a solution: from paradoxes to unifying concepts. Circulation 112: 745-758.
-
Trichon BH, Felker GM, Shaw LK, Cabell CH, O'Connor CM (2003) Relation of frequency and severity of mitral regurgitation to survivalamong patients withleftventricularsystolicdysfunction and heartfailure. Am J Cardiol 91: 538-543.
-
Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, et al. (2003) Recommendations for evaluation of the severity of native valvularregurgitationwithtwo-dimensional and Doppler echocardiography. J Am Soc Echocardiogr 16: 777-802.
-
Otsuji Y, Kumanohoso T, Yoshifuku S, Matsukida K, Koriyama C, et al. (2002) Isolatedannular dilation does not usually cause important functional mitral regurgitation: comparisonbetween patients withlone atrial fibrillation and thosewithidiopathic or ischemiccardiomyopathy. J Am CollCardiol 39: 1651-1656.
-
He S, Fontaine AA, Schwammenthal E, Yoganathan AP, Levine RA (1997) Integratedmechanism for functional mitral regurgitation: leaflet restriction versus coapting force: in vitro studies. Circulation 96: 1826-1834.
-
Otsuji Y, Handschumacher MD, Schwammenthal E, Jiang L, Song JK, et al. (1997) Insights fromthree-dimensionalechocardiographyinto the mechanism of functional mitral regurgitation: direct in vivo demonstration of alteredleaflettetheringgeometry. Circulation 96:1999- 2008.
-
Yiu SF, Enriquez-Sarano M, Tribouilloy C, Seward JB, Tajik AJ (2000) Determinants of the degree of functional mitral regurgitation in patients withsystolicleftventriculardysfunction: A quantitative clinicalstudy. Circulation 102: 1400-1406.
-
Lachmann J, Shirani J, Plestis KA, Frater RW, LeJemtel TH (2001) Mitral ring annuloplasty: an incomplete correction of functional mitral regurgitationassociatedwithleftventricularremodeling. CurrCardiolRep 3: 241-246.
-
Agricola E, Oppizzi M, Maisano F, De Bonis M, Schinkel AF, et al. (2004) Echocardiographic classification of chronicischemic mitral regurgitationcaused by restricted motion according to tethering pattern. Eur J Echocardiogr 5: 326-334.
-
Calafiore AM, Gallina S, Di Mauro M, Gaeta F, Iaco AL, et al. (2001) Mitral valve procedure in dilatedcardiomyopathy: repair or replacement? Ann ThoracSurg 71: 1146-1152.
-
Sadeghpour A, Abtahi F, Kiavar M, Esmaeilzadeh M, Samiei N, et al. (2008) Echocardiographicevaluation of mitral geometry in functional mitral regurgitation. J CardiothoracSurg 3: 54.
-
Karaca O, Avci A, Guler GB, Alizade E, Guler E, et al. (2011) Tenting area reflectsdiseaseseverity and prognosis in patients with non-ischaemicdilatedcardiomyopathy and functional mitral regurgitation. Eur J Heart Fail 13: 284-291.
-
yan L, Jackson B, Parish L, Sakamoto H, Plappert T, et al. (2007) Quantification and localization of mitral valve tenting in ischemic mitral regurgitationusing real-time three-dimensionalechocardiography. Eur J CardiothoracSurg. 31: 839-844.
-
Nagasaki M, Nishimura S, Ohtaki E, Kasegawa H, Matsumura T, E et al. (2006) The echocardiographicdeterminants of functional mitral regurgitationdiffer in ischemic and non-ischemiccardiomyopathy. Int J Cardiol. 108 171- 76.
-
Kwan J1, Shiota T, Agler DA, Popovic ZB, Qin JX, et al. (2003) Geometricdifferences of the mitral apparatusbetweenischemic and dilatedcardiomyopathywithsignificant mitral regurgitation: real-time three-dimensionalechocardiographystudy. Circulation 107: 1135-1140.
-
Yu HY, Su MY, Liao TY, Peng HH, Lin FY, et al. (2004) Functional mitral regurgitation in chronicischemiccoronaryarterydisease: Analysis of geometricalterations of mitral apparatuswithmagneticresonanceimaging. J ThoracCardiovascSurg128: 543-551.
-
Fattouch K, Castrovinci S, Murana G, Novo G, Caccamo G, et al. (2011) Multiplanetwo-dimensional versus real time three-dimensionaltransesophagealechocardiography in ischemic mitral regurgitation. Echocardiography 28: 1125-1132.
