This is a rare case of a 53-year-old woman with history of oophorectomy and hysterectomy 3 years prior to presentation admitted for gait abnormality and found to have a basal ganglia stroke. Transthoracic echocardiogram for stroke work up revealed a cardiac mass in the right atrium emanating from Inferior Vena Cava (IVC). Computed Tomography imaging of abdomen and pelvis ruled out malignancy. The mass was surgically removed due to high risk of embolization. Intraoperative, transesophageal echocardiogram was negative for inter-atrial shunt. Pathology report revealed Benign Metastasizing Leiomyoma that was estrogen and progesterone hormone positive.
Benign Metastasizing Leiomyoma (BML) is a rare entity that was first described 80 years ago [1]. Since then, approximately 200 cases have been reported in women with a history of uterine leiomyoma with the lung as the most common site for metastases [2]. The etiology of BML largely remains unexplained. However, several hypotheses have been developed since its first clinical description including spontaneous lymphatic or hematogenous spread, implantation and proliferation by seeding at the time of surgery, and primary endovascular smooth muscle proliferation [2-7]. Here we present a case of cardiac BML discovered in the process of a patient evaluation following a stroke.
A 53-year-old woman presented with several weeks of a gait disturbance and dyspnea. Her past medical history included hypertension, dyslipidemia, type 2 diabetes mellitus, and an abdominal hysterectomy with bilateral salpingo-oophorectomy which was performed three years prior for symptomatic uterine leiomyoma. There was also a history of chronic pulmonary nodules dating back 8 years; prior biopsy of one of the nodules revealed a benign hamartoma.
On her initial presentation, the physical exam was notable for a mild gait disturbance. Otherwise, there were no other abnormalities. Laboratory studies were normal. The electrocardiogram revealed sinus rhythm with 1st degree AV Block. Chest x-ray showed unchanged pulmonary nodules. A magnetic resonance imaging (MRI) of the brain showed a left basal ganglia infarct with extension to the periventricular white matter (Figure 1). Chest computed tomography angiography (CTA) ruled out pulmonary embolism as a cause for the dyspnea. The CTA also demonstrated multiple pulmonary nodules in the right upper and left upper lobes that had a bulky fat-like appearance suggestive of hamartomas or metastatic leiomyosarcoma (Figure 2).
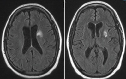 Figure 1: Cardiac MRI: Infarct involving left basal ganglia with extention to periventricular white matter.
View Figure 1
Figure 1: Cardiac MRI: Infarct involving left basal ganglia with extention to periventricular white matter.
View Figure 1
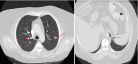 Figure 2: CT Scan of the chest revealing bilateral pulmonary nodules (red arrows). Left inferior pleural surface reveals nodule with bulk fat (blue arrow).
View Figure 2
Figure 2: CT Scan of the chest revealing bilateral pulmonary nodules (red arrows). Left inferior pleural surface reveals nodule with bulk fat (blue arrow).
View Figure 2
As a part of the stroke evaluation, a transthoracic echocardiogram (TTE) was performed. This revealed a multi-lobulated, elongated mobile mass arising from the inferior vena cava, traversing the right atrium and flopping in and out of the tricuspid valve (Figure 3a, Figure 3b and Figure 3c). The remainder of the echocardiogram was normal including the absence of an intra-cardiac shunt as demonstrated with an agitated saline study with Valsalva maneuver. A CT of the abdomen and pelvis ruled out malignancy. Carotid Doppler studies revealed no evidence of hemodynamically significant stenosis. A venous duplex study of the lower extremity veins was negative for venous thrombosis.
 Figure 3: a) Four Chamber apical view. Right atrial mass (white arrow) crossing tricuspid plane during diastole. The mass (blue arrow) is confined to the right atrium during systole; b) Parasternal short axis view at the level of aortic valve. Mobile right atrial mass (white arrow) traversing tricuspid plane during diastole; c) Subcostal view: The mass is attached to Inferior vena cava (orange arrow). Mobile mass in the right atrium (red arrow).
View Figure 3
Figure 3: a) Four Chamber apical view. Right atrial mass (white arrow) crossing tricuspid plane during diastole. The mass (blue arrow) is confined to the right atrium during systole; b) Parasternal short axis view at the level of aortic valve. Mobile right atrial mass (white arrow) traversing tricuspid plane during diastole; c) Subcostal view: The mass is attached to Inferior vena cava (orange arrow). Mobile mass in the right atrium (red arrow).
View Figure 3
Due to the size and mobility of the right atrial mass, and concern that it represented either a thrombus in transit or a cardiac tumor, either entity with the potential for a massive pulmonary embolism, the patient underwent urgent cardiac surgery to remove the mass. An intraoperative Transesophageal Echocardiogram (TEE) was also done to confirm position of the mass and rule out inter-atrial shunt. (Figure 4a, Figure 4b, Figure 4c, and Figure 4d).
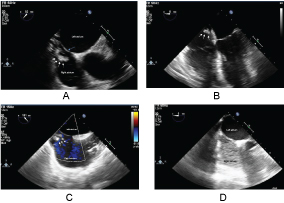 Figure 4: a) Mid-esophageal TEE revealing the mass (white arrow) in the right atrium. Interatrial septum (Blue arrow); b) TEE 4 chamber view: The mass (white arrow) in the right atrium; c) TEE Bi-caval view: The mass (white arrow) emanating from Inferior Vena Cava; d) TEE with agitated saline was negative for inter-atrial shunt.
View Figure 4
Figure 4: a) Mid-esophageal TEE revealing the mass (white arrow) in the right atrium. Interatrial septum (Blue arrow); b) TEE 4 chamber view: The mass (white arrow) in the right atrium; c) TEE Bi-caval view: The mass (white arrow) emanating from Inferior Vena Cava; d) TEE with agitated saline was negative for inter-atrial shunt.
View Figure 4
After the patient was placed on cardiopulmonary bypass, a right atriotomy was performed revealing an elongated, yellow, rubbery mass emanating from the IVC attached by a fibrous tether. The mass was excised in its entirety (Figure 5). The patient recovered well from the surgery and without complication.
 Figure 5: Elongated portion of rubbery gray-tan tissue measuring 8.4 × 1.6 × 0.9 cm.
View Figure 5
Figure 5: Elongated portion of rubbery gray-tan tissue measuring 8.4 × 1.6 × 0.9 cm.
View Figure 5
Gross pathology showed an elongated portion of rubbery gray-tan tissue measuring 8.4 × 1.6 × 0.9 cm. Microscopic pathology revealed markedly hyalinized and focally calcified fibrous tissue with associated smooth muscle (Figure 6). It contained hyalinized fibro-adipose tissue and focally calcified smooth muscle cells (Figure 7a and Figure 7b). Immunohistochemical stain was positive for desmin and muscle actin. The specimen was negative for calretinin, WT-1, CD-34, CD-31, S100, Myogenin, HMB-45 and Melan-A. Staining for estrogen and progesterone was strongly positive (Figure 8). These findings were consistent with the diagnosis of a benign metastasizing leiomyoma. A follow-up TTE one month after discharge showed no evidence of early regrowth of the cardiac mass. With no inter-artrial shunt found on TEE, the stroke may be a separate entity due to high risk factors of diabetes, hypertension, and hyperlipidemia for cerebrovascular disease.
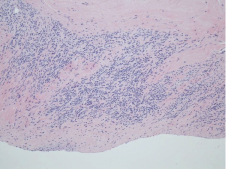 Figure 6: Smooth Muscle Microscopic Section.
View Figure 6
Figure 6: Smooth Muscle Microscopic Section.
View Figure 6
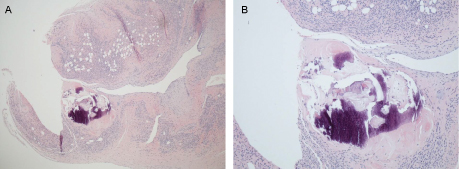 Figure 7: a) Markedly hyalinized and focally calcified fibrous tissue with associated smooth muscle; b) Fibro-adipose tissue which was markedly hyalinized and focally calcified containing smooth muscle.
View Figure 7
Figure 7: a) Markedly hyalinized and focally calcified fibrous tissue with associated smooth muscle; b) Fibro-adipose tissue which was markedly hyalinized and focally calcified containing smooth muscle.
View Figure 7
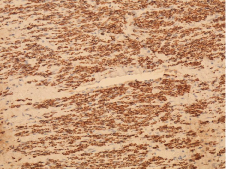 Figure 8: Immunohistochemical stain was positive for desmin and muscle actin. Staining for estrogen and progesterone was done which revealed 95% and 20% immuno-reactivity, respectively.
View Figure 8
Figure 8: Immunohistochemical stain was positive for desmin and muscle actin. Staining for estrogen and progesterone was done which revealed 95% and 20% immuno-reactivity, respectively.
View Figure 8
In 1939, Dr. Paul Steiner first coined the term "metastasizing fibroleiomyoma". He published a report of a patient who died from pulmonary metastases of benign-appearing leiomyomas, which caused chronic pulmonary arterial obstruction with cor pulmonale, polycythemia and right sided heart failure [1]. The findings were histologically identical to the multiple leiomyomas in the uterus. It was hypothesized that the tumor spread through the venous system from uterus to heart to lungs and through lymphatic channels from lungs to tracheal lymph nodes [1]. An alternative theory of cardiac BML is that the tumor embolizes through the venous system at the time of hysterectomy or uterine myomectomy [2].
Joo, et al. described a case report of a patient who presented with blurred vision, diplopia and tinnitus and was found to have a solid epidural tumor and a pelvic mass. The histopathology of the epidural tumor was found to be leiomyoma, with a characteristic of benign smooth muscle without pleomorphism, atypia or necrosis. The pelvic mass histopathology was consistent with ovarian leiomyoma. This brought to light a metaplasia theory for BML, which entails metaplastic transformation of the coelomic epithelium in any location where mesothelial meschenchymal cells exist as a cause of BML [5].
The final theory involves peritoneal seeding after myomectomy or hysterectomy [5]. This is thought to occur by fragments of uterine leiomyoma implanting inside the peritoneum after laparotomy or laparoscopic morcellation [2-7].
In April 2017, Barnas, et al. published a literature review of 161 cases published from 1965 to 2016 and showed that BML is usually identified in the perimenopausal period [2]. The mean age of primary surgery (myomectomy and hysterectomy) was 38.5 years, whereas the mean age of symptomatic BML diagnosis was 47.3 years, roughly 9 years after surgery [2]. Our patient had a hysterectomy three years prior to presentation. However, this study found no significant relationship between the type of primary surgery and BML diagnosis with respect to timing of surgery or site of metastasis. Three out of the four other recorded cases of BML to the heart had multiple lung metastases [7-12]. In these case reports, BML was found in the right atrium, interventricular septum, tricuspid valve and right ventricle [8].
A number of studies have tried to discern the cytogenetic background of BML. Nucci, et al. described consistent chromosomal aberrations in 19q and terminal deletions in 22q in all BML cases and suggested that BML is a genetically distinct entity [13]. Lee, et al. also concluded that BML may comprise a heterogenous group of tumors in terms of their malignant potential and pathogenetic mechanisms. However, in their described case, significant genetic abnormalities were shared by both lesions from the uterus and lungs [14].
Previous studies have reported these tumors often stain positively for both estrogen and progesterone receptors [8-12]. Our patient's cardiac mass was 95% and 20% immuno-reactive for estrogen and progesterone, respectively, consistent with a uterine origin.
There have been case reports of recurrent BML, pointing out the need for surveillance. As per Awongua, et al., two patients on estrogen therapy after tumor resection experienced recurrence [15]. In one case, imaging of the abdomen revealed multiple masses in the abdomen and pelvis. The second case revealed a left lung nodule and multi-lobulated masses within the pelvis [15]. The recurrence of BML may support the presence of karyotypic aberrations in 56% of cases of benign leiomyomas [13]. This is thought to occur from the metaplastic transformation that occurs under hormonal influences, such as estrogen's effect on myofibroblasts [16]. Our patient was not on estrogen replacement therapy, and has been followed for continued surveillance of recurrence. Treatments with aromatase inhibitors, anti-estrogens, and luteinizing hormone releasing hormone (LHRH) agonists are effective in both the regression of the leiomyomatous tumors and prophylaxis against recurrence [12-17].
Benign Metastasizing Leiomyoma (BML) should be included in the differential diagnosis when a patient presents with an intra-cardiac mass and has a history of uterine fibroids, myomectomy or hysterectomy. To date, the prognosis for BML has been favorable. More data is required to determine the optimal diagnostic imaging techniques, therapeutic strategies, and frequency of post-surgical surveillance for evaluating recurrence.