Superior vena cava (SVC) obstruction is a recognized complication following cardiac surgery that may result in significant clinical sequelae if not treated early. Transcatheter stenting is rapidly becoming the treatment of choice, considering its reduced post-procedure morbidity and faster recovery time. In early postoperative vascular lesion, primary stenting is preferred over balloon angioplasty to prevent fresh suture line disruption. In paediatric, small patient sizes as well as the need for future vessel growth, complicate the use of stents in this group of patients. We present two cases of successful relief from severe SVC obstruction that occurred early after cardiac surgical repair. Case 1, is a 2-month-old girl with a large perimembranous ventricular septal defect (VSD) and patent ductus arteriosus (PDA), who underwent VSD closure and PDA ligation but was complicated by SVC tear during cannulation. Case 2 is a 35-year-old gentleman with a sinus venosus atrial septal defect, who underwent Warden procedure but developed SVC obstruction at SVC-right atrium anastomosis site. The presentation and management of these patients will be highlighted in these two cases.
Superior vena cava obstruction, Stenting, Balloon angioplasty, Warden procedure
SVC obstruction can be a significant complication in patients undergoing cardiac operation. It is a relatively rare incidence among children and may be associated with previous congenital heart surgery [1]. About two-thirds of reported cases of SVC obstruction in a study among paediatric and young adult population were from the post-cardiac surgery following Mustard/Senning procedures, partial anomalous pulmonary venous repair, cardiac transplant, and arterial switch operation [2]. Currently, with the tremendous technical improvement and new stents design, treatment with stenting is widely accepted and is becoming the modality of choice due to its reduced post-procedure morbidity and faster recovery time. Unlike in adults, the use of stenting to relieve SVC obstruction can be complicated in paediatric age groups due to small patient size and the need for future vessel growth with higher risk of reintervention due to restenosis or stent occlusion. Consent was given by the parents (case 1) and patient (case 2) for this case reports.
A 2-month-old infant girl with a weight of 4.1 kg underwent ventricular septal defect closure and ligation of patent ductus arteriosus. Intraoperatively it was complicated with SVC tear with bleeding and proceeded with SVC repair. The immediate post-operative period was complicated by low cardiac output syndrome and pulmonary hypertension requiring multiple inotropic supports and inhaled nitric oxide. At day three postoperatively, she was noted to have facial congestion, bilateral eyes puffiness and upper limbs edema (Figure 1). Her ventilation requirement was increased with the need for high-frequency oscillatory ventilation. An urgent transthoracic echocardiogram was done which showed restricted flow at mid-SVC with a maximal velocity of > 1.6 m/s with proximal SVC maximal velocity of 1.0 m/s. In view of significant SVC obstruction, she was started on heparin infusion and proceeded with emergency catheter intervention.
 Figure 1: Facial, upper chest and limbs oedema and congestion.
View Figure 1
Figure 1: Facial, upper chest and limbs oedema and congestion.
View Figure 1
Angiogram from internal jugular venous line revealed narrowing at the SVC site immediately distal to connection with the innominate vein (Figure 2). The narrowest diameter was 2.7 mm. SVC diameter post narrowing was 4.9 mm. Using MPA2 4F with straight and J-tip Terumo wire, the catheter was directed to innominate and distal SVC for selective injection. Hemodynamics were taken which showed an SVC mean pressure of 28 mmHg, right atrium (RA) mean pressure 15 mmHg, with an SVC-RA gradient across 13 mmHg. The narrowest segment was inflated with coronary balloon 3.5 mm × 15 mm inflated to 8 atm twice. Post inflation showed angiographic improvement but no gradient reduction. Open surgical repair was discussed with the surgeon but the surgeon's thought that SVC obstruction is not amenable for redo or further SVC repair. Furthermore, her condition was very ill and hemodynamically very unstable that lead to decision for SVC stenting to avoid high risk open surgical repair. Emergency stenting with Advanta V12 covered stent (Atrium Medical Corp, Hudson, NH) with the only available stent's size of 5 mm × 16 mm and inflated to 10 atm. Post-stenting angiogram showed good flow across the stent with good stent position (Figure 3). The CVP monitoring in the intensive care unit went down from 28 cm H20 to 13 cm H20.
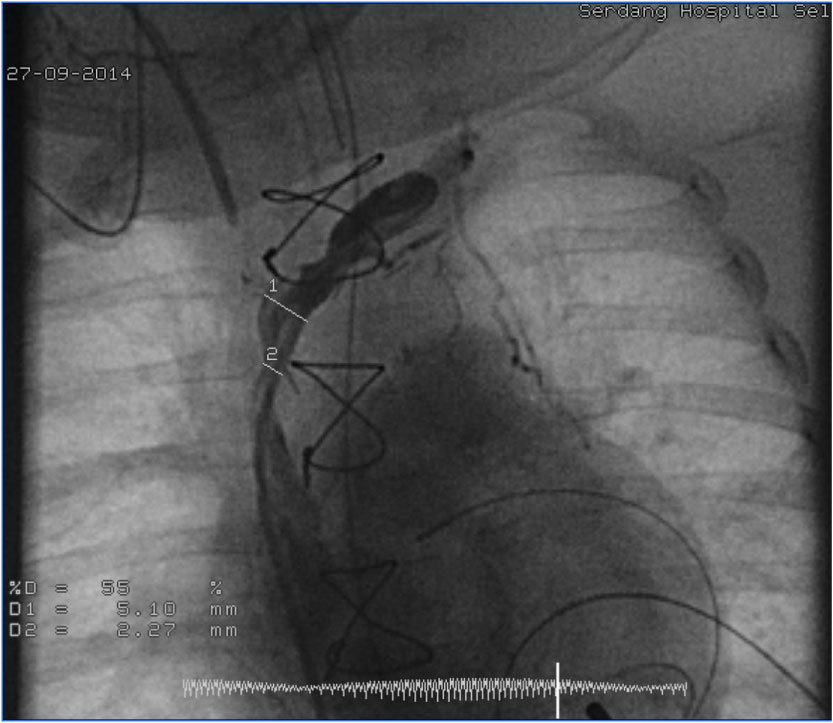 Figure 2: Angiogram showing a narrowing at the SVC site immediately distal to connection with the innominate vein (white arrow).
View Figure 2
Figure 2: Angiogram showing a narrowing at the SVC site immediately distal to connection with the innominate vein (white arrow).
View Figure 2
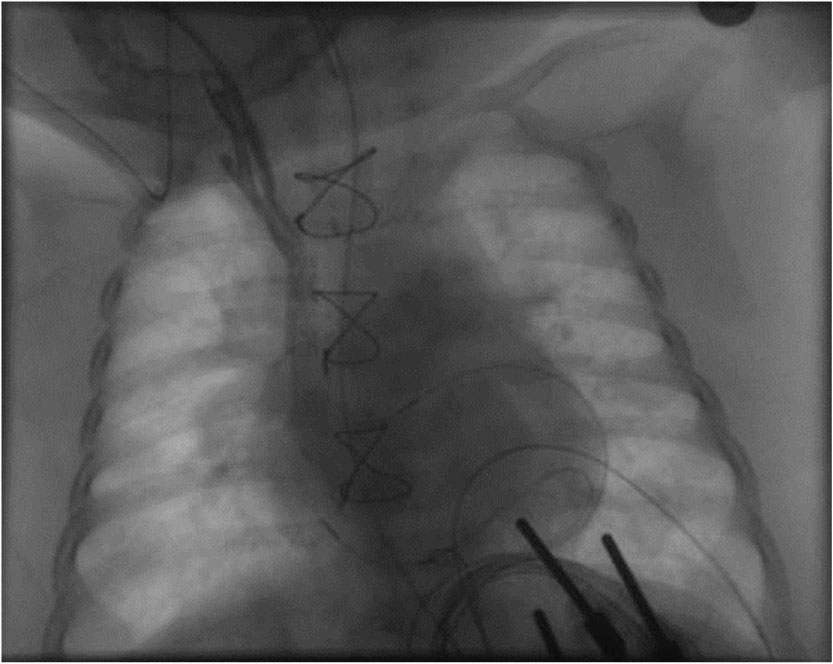 Figure 3: Angiogram post-SVC stenting, showing good flow across the stent and good stent position.
View Figure 3
Figure 3: Angiogram post-SVC stenting, showing good flow across the stent and good stent position.
View Figure 3
Facial congestion and edema resolved after three days of stenting (Figure 4) and she was extubated after 5 days. She was discharged well with aspirin after 13 days of hospitalisation. Her initial follow up suggested a good functioning SVC stent.
 Figure 4: Day-1 post-stenting, less facial oedema and congestion.
View Figure 4
Figure 4: Day-1 post-stenting, less facial oedema and congestion.
View Figure 4
Even though this covered stent can be redilated to accommodate the vessel growth, potential stent mismatch was anticipated due to a small stent's size being used. Her subsequent serial follow up later detected a partial SVC obstruction with the restricted flow at mid-SVC with a peak gradient of 6 mmHg from the age of 7 months. She was however managed conservatively as she was asymptomatic. The SVC obstruction noted to be worsened with no flow across the SVC at the age of 2 years and 3-months-old. She was planned for CT - angiogram for suspected total SVC occlusion and referred for surgical intervention. Unfortunately her parents decided to go to another hospital.
A 35-year-old gentleman, was diagnosed to have sinus venosus atrial septal defect. He was in NYHA class I and there was no history of previous intervention before. He underwent Warden procedure but at 2 hours postoperatively, he was noted to have increasing central venous pressure up to 30 cm H2O. He was then referred to us for urgent SVC catheter intervention on the same day for suspected SVC obstruction at the level SVC-RA junction. The SVC angiogram revealed a significant narrowing at distal SVC (Figure 5). The SVC mean pressure was measured at 37 mmHg and RA mean pressure at 13 mmHg, with pressure gradient of 24 mmHg. The SVC was stented with Atrium V12 covered stent (Atrium Medical Corp, Hudson, NH) 10 mm × 38 mm inflated to 12 atm. The stent was then post dilated with Mullin- X balloon Numed Inc, Hopkinton, NY) 12 mm × 40 mm inflated to 12 atm. The post-stenting SVC angiogram showed that the stent was in the intended position with good SVC flow to RA (Figure 6), and the recorded SVC pressure went down to 13 mmHg. The operation was complicated by pneumonia and pericardial effusion requiring open pericardial drainage. He was discharged well with aspirin after 3 weeks. On his last follow-up about three years post-SVC stenting, he was asymptomatic and the echocardiography revealed a good functioning stent.
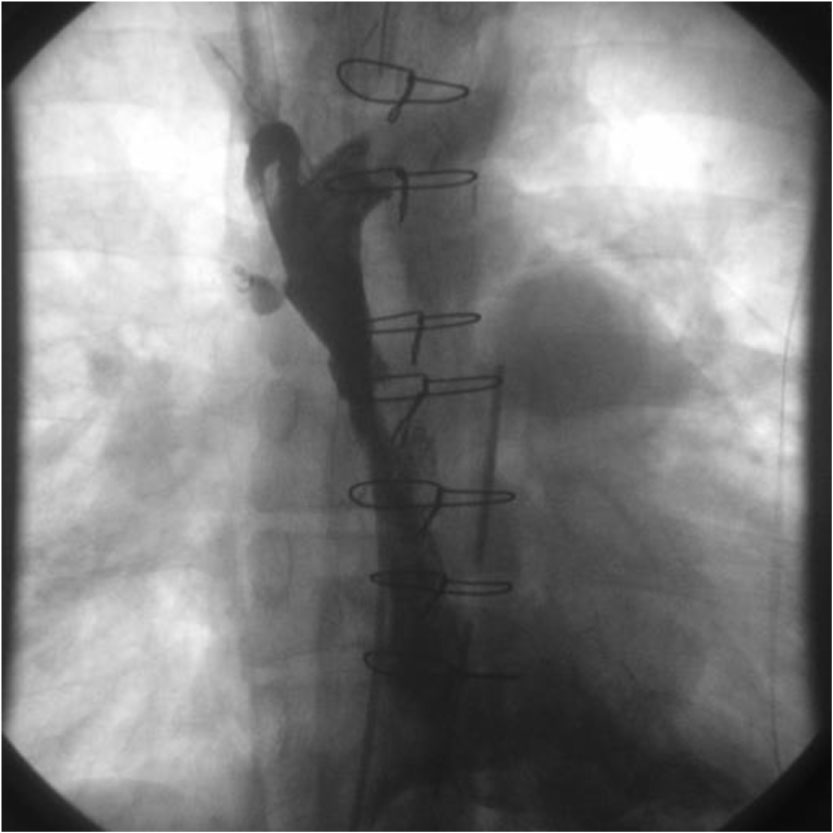 Figure 5: Angiogram showing a significant narrowing at the distal SVC (SVC-RA junction, white arrow) with dilated proximal SCV and innominate vein.
View Figure 5
Figure 5: Angiogram showing a significant narrowing at the distal SVC (SVC-RA junction, white arrow) with dilated proximal SCV and innominate vein.
View Figure 5
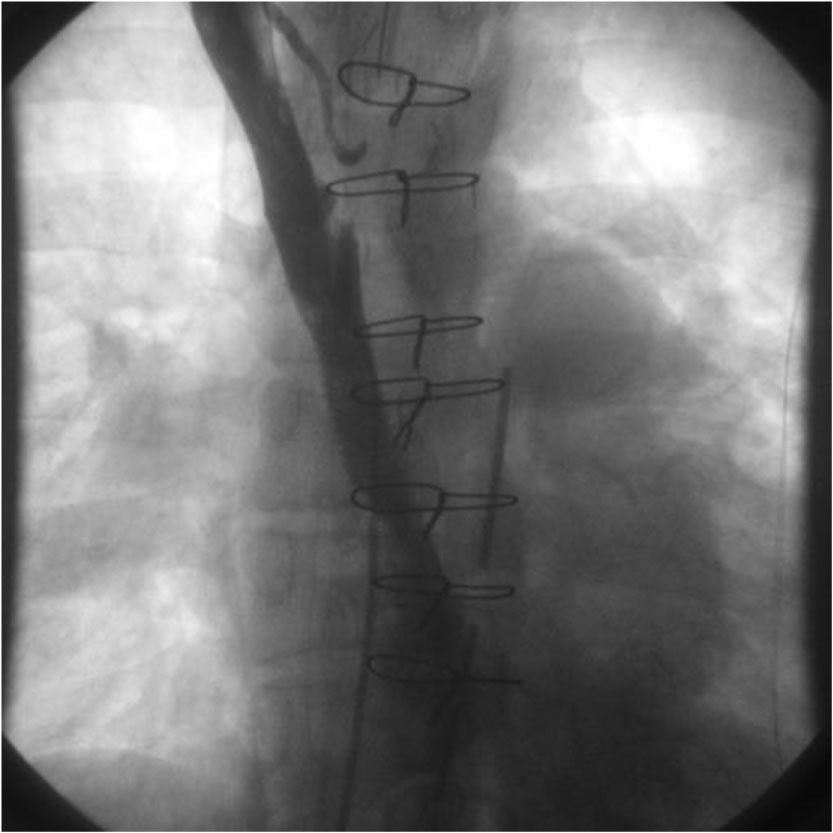 Figure 6: Post-stenting SVC angiogram showed that the stent in a good position with good SVC flow to RA.
View Figure 6
Figure 6: Post-stenting SVC angiogram showed that the stent in a good position with good SVC flow to RA.
View Figure 6
SVC syndrome occurs when SVC obstruction compromises normal venous flow from the head, upper extremities, and thorax, resulting in blood directed from deep veins to collateral pathways [3,4]. Symptomatic SVC obstruction may increase venous pressure, depicted as swelling and distention of the head, neck, and arms with erythrocyanotic appearance and engorgement of superficial veins in these territories. The degree and severity of symptoms depend on the extent and speed of narrowing of the SVC.
SVC obstruction following cardiac surgery is credibly related to the reconstructed anatomy, the presence of surgical anastomosis, or even caval cannulation sites for cardiopulmonary bypass [2]. Jayakumar, et al. attribute the causes of SVC obstruction at sites of surgical anastomoses to several factors including a mismatch in vessel size, intimal hyperplasia, constriction by sutures, thrombosis, and strictures formation [5]. Whereas, tremendous use of indwelling catheters and devices accounts to be the most common benign cause of SVC syndrome in both adults and children [3,4]. Cancer leads to extrinsic compression, whereas indwelling catheters lead to intrinsic fibrosis and thrombosis [4]. In both our cases, the SVC obstruction occurred early, and this could be due to the constriction by surgical sutures. There was no visible thrombus noted from the echocardiography to suggest obstruction secondary to thrombosis.
The management of SVC obstruction must be tailored to the underlying etiology with the primary goal of relieving the anatomic obstruction [3]. Treatment options include open surgical bypass and transcatheter stenting. Many studies reveal that balloon dilatation or SVC stent implantation is safe and effective to relieve SVC obstruction [3,6,7]. In general, stenting increases the efficacy of balloon angioplasty, maintains shunt patency and also increases the safety of balloon angioplasty as intravascular stenting enables scaffolding and provides a smooth neo-intimal growth [8]. Transcatheter stenting is fast becoming the treatment of choice, considering its minimally invasive non-surgical procedure with rapid recovery time compared to surgery [9]. It is also preferred over balloon angioplasty in early postoperative vascular lesion to prevent fresh suture line disruption [10].
In paediatric patients, an expandable stent has the critical feature of allowing post-dilatation, which is essential taking into consideration their somatic growth [8]. Stanfill, et al. reported that stent implantation is safe and effective in infants but need serial dilatation to keep pace with somatic growth and they recommended that efforts should be made to implant stents with potential adult size diameter to avoid future surgery [11]. Whereas Alias, et al. recommended iliac stents (Johnson & Johnson P188 and P308) due to its ability to redilate to achieve a diameter of 18 mm, which is adequate for adult size [1]. In our case, even though this covered stent can be redilated to accommodate the vessel growth later, potential stent mismatch was anticipated due to a small stent's size. The risk of restenosis seen in case 1 can also be related to overdilation of the stent on attempting to gain a maximal vessel diameter. Mc Mahon, et al. reported that awareness of specific risk factors and modification of the stent implantation technique, including avoidance of minimal stent overlap and sharp angulation of the stent to the vessel wall and avoidance of overdilation able to decrease the incidence of neointimal proliferation and restenosis [12].
Unlike case 1, the outcome of SVC stenting in case 2 is quite good with very low-risk for reintervention. A study by Tzifa, et al. demonstrated that freedom from re-intervention was longer in patients aged more than five years at the time of intervention [2].
Other possible complications of SVC stenting ranged from minor complications such as groin hematoma and infection at the puncture site, to significant complications including stent embolization, reocclusion of stents, stent malposition, migration, early embolization, neointimal proliferation, and restenosis, bleeding, cardiac injury, pulmonary embolism, pulmonary edema, and pericardial tamponade [6,7,13].
This group of patients will undoubtedly require continued follow-up with further intervention from time to time based on their condition. It is adequate to follow up the patients based on their clinical examination and transthoracic echocardiogram solely. However further imaging by CT angiography or venography can be done in those who require reintervention.
SVC obstruction that occurs early following cardiac surgery can be safely managed with transcatheter stenting. Stenting is becoming the modality of choice compared to surgery due to its reduced post-procedure morbidity and faster recovery time. The stent of choice in these group of patients is limited to covered stent considering the fact that SVC obstruction is related to post-repair with freshly-sutured anastomosis. An essential consideration in placing a stent in an infant or child is the need for redilation to accommodate physical growth and ability to achieve adult size diameter.