Atherosclerotic disease in one arterial site, raise the probability of having other sites affected by about 50% within the vascular axis. Hence once vascular pathology found in one site i.e. coronary artery disease (CAD), other sites i.e. Cerebral and peripheral circulation must be assessed thoroughly, especially in patients with multiple risk factors. Percutaneous intervention (PCI) is a conservative reasonable solution for high risk and inoperable cases; sometimes it supersedes the choice surgery especially with the new era of drug eluting stents (DES) and combined Anti-Ischemic medications.
Coronary artery bypass graft (CABG) rather than PCI was the favored cost-effective treatment for complex multivessel coronary artery disease (MVCAD) in the long term [1]. While the evidence base for the cost-effectiveness of DES compared with CABG is growing [1]. Despite the benefits of Coronary Artery Bypass Graft surgery, 15% to 25% of patients develop graft closure within one year following the procedure [2].
Carotid atherosclerotic disease can lead to ischemic stroke or transient ischemic attack (TIA) from embolization, thrombosis, or hemodynamic compromise [3]. Carotid endarterectomy (CEA) was the initial and sole revascularization method for a significant > 70% stenosis [3-12], followed later by introduction of transcatheter Percutaneous angioplasty and stenting [13-20].
For a selected patients with carotid stenosis of 70 to 99 percent, carotid artery stent (CAS) rather than carotid endarterectomy (CEA) is recommended if any of the following conditions are present: A carotid lesion that is not suitable for surgical access, Radiation-induced stenosis, restenosis after CEA, and clinically significant cardiac, pulmonary, or other disease that greatly increases the risk of anesthesia and surgery [13-24].
We hereby present a case of 78-years-old with severe coronary, carotid and peripheral arterial atherosclerosis who showed a successful example of the solution of Hybrid approach of surgical and stenting approach in such cases.
Coronary artery disease, Peripheral artery disease, Carotid artery stenosis, Percutaneous intervention, Carotid artery stenting, CABG, Iliac artery stenting
This a case report of patient with severe systemic atherosclerosis with severe coronary artery disease (CAD), peripheral arterial disease (PAD), and bilateral carotid disease. Who underwent hybrid approach with surgical (coronary artery bypass grafting-CABG) and endovascular stenting (Coronary, Aorto-iliac, and Carotid stenting).
78-year-old, male, with a history of Hypertension, Diabetes, Dyslipidemia, Chronic Heavy Smoker, Chronic Obstructive Pulmonary Disease (COPD), Coronary Artery Disease (CAD) status post coronary artery bypass graft (CABG) 10-years ago, three grafts left internal mammary artery (LIMA) to left anterior descending artery (LAD), saphenous vein graft (SVG) to obtuse marginal (OM) and saphenous vein graft (SVG) for the right coronary artery (RCA). He was also recently diagnosed with severe Peripheral Artery Disease (PAD) with bilateral lower limb claudication and was found to have bilateral occlusive iliac disease, significant right carotid 80% and moderate 60% left carotid on non-invasive tests during his current admission for recurrent angina of three months duration. The patient stated that he was not complaint on his medications and he was still smoking.
On examination he is conscious, fully oriented, alert and cooperative, his vital signs were within normal limits, he had a prominent right carotid bruit with faint left Carotid bruit Chest is clear to auscultation, cardiac auscultation showed normal regular first and second heart sounds with grade I/VI ejection systolic murmur. Mild lower limbs edema, fiable peripheral pulses and monophasic Doppler signals. No neurological motor or sensory deficit.
His investigations showed GFR 68%, CR 1.2 umol/L, Uric Acid 6.5 mg/dl, Normal TSH, HBA1C 7.49%, TC 140 mg/dl, LDL 98 mg/dl, HDL 42 mg/dl, TG 68 mg/dl, Troponin 0.05 ug/L, CK 100 U/L, CKMB 4.0 ug/L, BNP 226 pg/mL ECG: NSR with old Inferolateral changes.
Echocardiogram: moderate dilation of the left ventricle with severely impaired LV systolic function, LVEF = 30%. Akinesia of basal and mid Inferolateral wall, mid-septum, Septo-basal, mid-lateral, mid-inferior and Infero-basal wall. Grade I abnormal diastolic relaxation, left atrial mild dilated. Normal pulmonary arterial pressure (Figures 1). Lower extremities venous Doppler study was unremarkable.
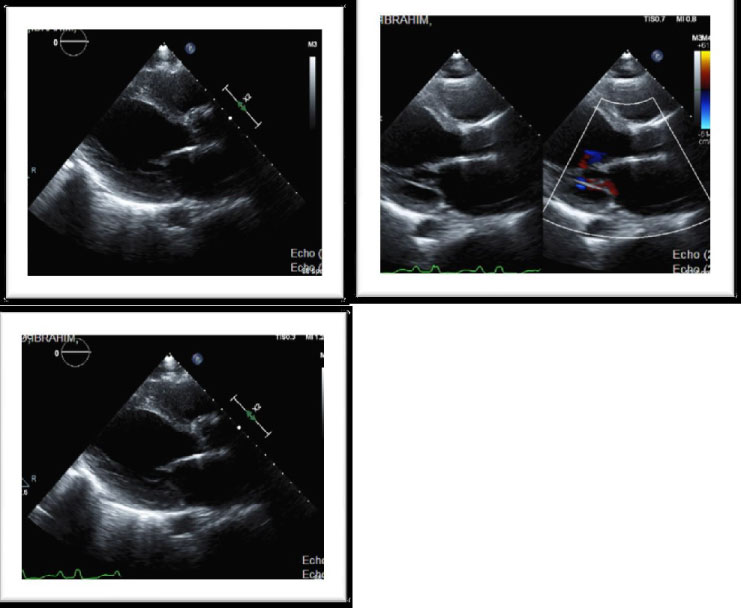 Figure 1: Moderate dilation of the left ventricle with severely impaired LV systolic function LVEF = 30%. Akinesia of basal and mid Inferolateral wall, mid-septum, Septo-basal, mid-lateral, mid-inferior and Infero-basal wall GIDD.
View Figure 1
Figure 1: Moderate dilation of the left ventricle with severely impaired LV systolic function LVEF = 30%. Akinesia of basal and mid Inferolateral wall, mid-septum, Septo-basal, mid-lateral, mid-inferior and Infero-basal wall GIDD.
View Figure 1
The patient underwent peripheral, coronary/grafts, and carotid angiography after obtaining high risk consent. Lower extremities angiography was done first showed bilateral iliac occlusion and underwent successful bilateral iliac angioplasty and stenting (as he was deemed not a surgical candidate) with balloon expandable 10 × 59 mm stents with excellent patency and flow (Figures 2).
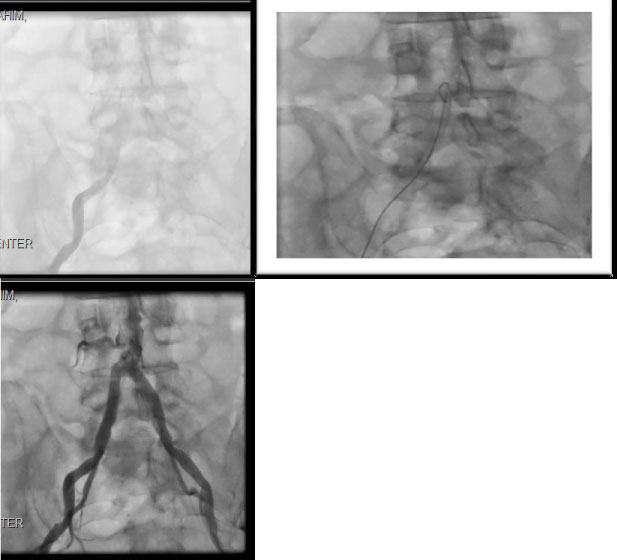 Figure 2: Showing bilateral iliac calcific occlusion (pre) and post Iliac Artery Stents Bilaterally.
View Figure 2
Figure 2: Showing bilateral iliac calcific occlusion (pre) and post Iliac Artery Stents Bilaterally.
View Figure 2
Then we proceeded with diagnostic coronary and graft angiography which showed occlusion of native vessel LAD, RCA, subtotal distal left main (LMN) and ostial left circumflex (LCX) as well as occluded SVG to OM & occluded SVG to RCA, he had patent LIMA to LAD supplying Collateral to posterior descending artery, moderate left Subclavian artery 40%-50% disease (Figures 3). So ad hoc PCI was done to distal LMN into LCX angioplasty and stenting using drug eluting stent (DES) 3.5 × 18 mm with excellent result and TIMI III flow and with improved collateral flow to distal RCA posterior and lateral ventricle circulation (Figures 3).
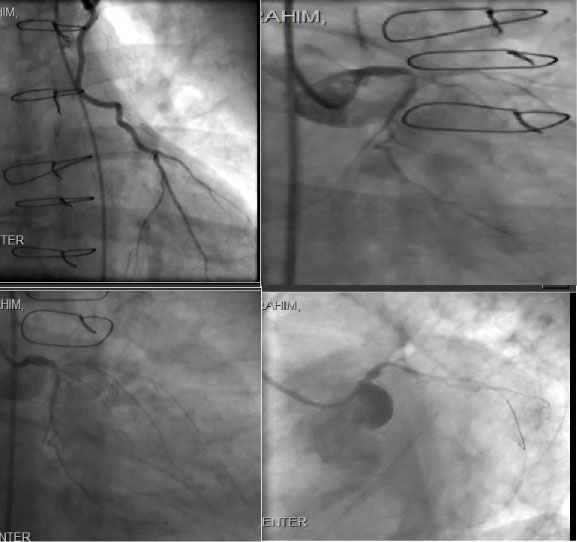 Figure 3: Patent LIMA to LAD, Subtotal distal LMN and ostial LCX, Left Main and Circumflex Coronary Artery Post Angioplasty/stent.
View Figure 3
Figure 3: Patent LIMA to LAD, Subtotal distal LMN and ostial LCX, Left Main and Circumflex Coronary Artery Post Angioplasty/stent.
View Figure 3
On the same setting Carotid Angiogram showed significant > 80% right ICA, with left carotid artery 60% stenosis. We proceeded with intervention also in the same setting, Successful right internal carotid artery angioplasty and stenting using 6 × 8 × 30 mm XACT self-expandable stent with Emboshield NAV 6 distal protection filter device, achieving excellent angiographic result with improved right cerebral perfusion on post stent angiogram (Figures 4).
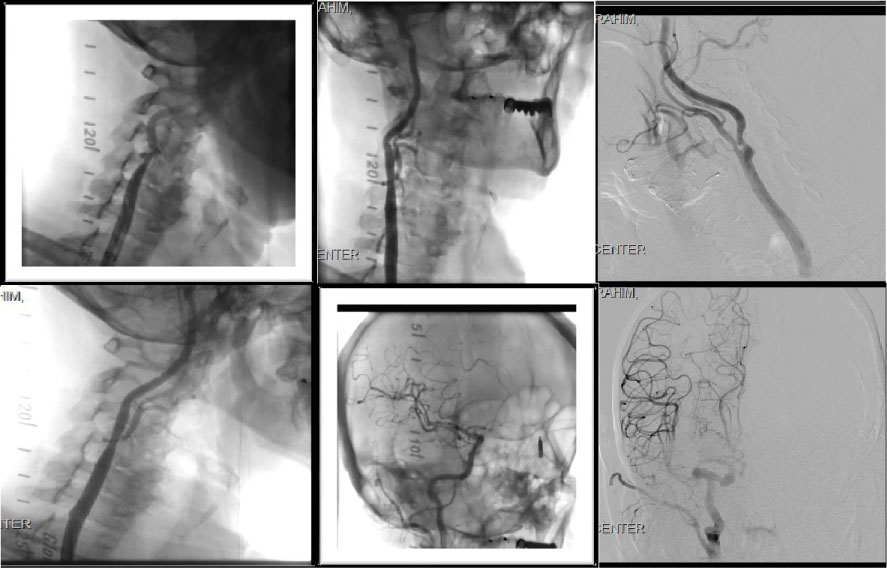 Figure 4: Showing the R Carotid artery stenosis (pre-angioplasty) showing the R Carotid artery stenosis (Post-angioplasty) Cerebral Angiogram Post stenting of the R.T carotid artery showing improved right hemispheric circulation.
View Figure 4
Figure 4: Showing the R Carotid artery stenosis (pre-angioplasty) showing the R Carotid artery stenosis (Post-angioplasty) Cerebral Angiogram Post stenting of the R.T carotid artery showing improved right hemispheric circulation.
View Figure 4
The patient was stable clinically post all these intervention procedures and no early or late complications. The patient was advised to comply on full Anti-Ischemic, anti-platelet, heart failure medications, lifestyle modification and he was referred to the smoking cessation clinic. He has been followed in outpatient clinic and reports no further symptoms and leading a routine and stable life with regular activities.
Atherosclerotic disease in one arterial site, raise the probability of having other sites affected by about 50% within the vascular axis. Hence once vascular pathology found in one site i.e. CAD, other sites i.e. Cerebral and peripheral circulation must be assessed thoroughly, especially in patients with multiple risk factors. Percutaneous intervention is a conservative reasonable solution for high risk and inoperable cases; sometimes it supersedes the choice surgery especially with the new era of DES and combined Anti-Ischemic medications.
Coronary artery bypass graft rather than PCI was the favored cost-effective treatment for complex multivessel CAD in the long term [1]. While the evidence base for the cost-effectiveness of DES compared with CABG is growing [1]. Despite the benefits of bypass graft surgery, 15% to 25% of patients develop graft closure within one year following the procedure [2].
Several multicenter, randomized clinical trials of carotid endarterectomy have provided data showing the usefulness of surgical revascularization for the treatment of patients with asymptomatic carotid stenosis. The results of these pivotal studies established the indications for endarterectomy in selected patients with asymptomatic stenosis of 60% or greater [3-6] and symptomatic carotid stenosis [9-13]. Since 1995 the recommendation for patients with asymptomatic carotid artery stenosis of 60% or greater reduction in diameter and whose general health makes them good candidates for elective surgery will have a reduced 5-year risk of ipsilateral stroke if carotid endarterectomy performed with less than 3% perioperative morbidity and mortality is added to aggressive management of modifiable risk factors [3-6].
Carotid-artery stenting has emerged as a therapeutic alternative to endarterectomy for the treatment of severe cervical carotid-artery stenosis. The results of randomized trials comparing stenting and endarterectomy in symptomatic patients have been conflicting, and till recently, no completed multicenter randomized trials have focused exclusively on asymptomatic patients, which is the largest group of patients undergoing carotid procedures in the United States [14]. In the Randomized Trial of Stent versus Surgery for Asymptomatic Carotid Stenosis trial, with regard to the primary composite end point of death, stroke, or myocardial infarction (MI) by 30-days after the procedure or ipsilateral stroke by 1-year, stenting was noninferior to endarterectomy (event rates, 3.8% and 3.4%, respectively) [17]. The 30-day rate of stroke was numerically higher in the stenting group than in the endarterectomy group (2.8 vs. 1.4%, P = 0.23), and the 30-day rate of death or stroke was 2.9% in the stenting group and 1.7% in the endarterectomy group [17].
Current guidelines state that it is reasonable to perform revascularization in asymptomatic patients with stenosis greater than 70% of the diameter of the artery �if the risk of perioperative stroke, MI, and death is low [18]. Similarly, CREST, a randomized trial of stenting versus endarterectomy in a combined cohort of symptomatic and asymptomatic patients with severe carotid stenosis, showed no significant difference in the rate of the primary end point between the stenting group and the endarterectomy group either over 4-years (hazard ratio, 1.11; 95% confidence interval [CI], 0.81 to 1.51) [21] or, in long term outcomes reported over 10-years (hazard ratio, 1.10; 95% CI, 0.83 to 1.45) [22]. ACT I used a qualification path for physician investigators that was similar to that used in CREST and, as in CREST, did not include specific subgroups of patients who were at high risk for complications from endarterectomy or stenting. At the time of the inception and initiation of ACT I, CREST was designed to evaluate only symptomatic patients. ACT I was designed to complement CREST by comparing stenting and endarterectomy in asymptomatic patients who were not older than 79-years of age and who were at standard risk for complications from both procedures, when the procedures were performed by interventionists and surgeons with adequate skill and experience and when routine embolic protection and dual antiplatelet therapy were used. CREST was later modified to include asymptomatic patients. It is widely recognized that the skill and experience of the physician is important in achieving acceptable outcomes both with endarterectomy and with stenting, particularly in asymptomatic patients, for whom the absolute risk reduction associated with the intervention is small [17-26]. The results of our study reinforce the findings of CREST, again suggesting that short-term and long-term outcomes with respect to the prevention of stroke are similar with stenting and endarterectomy. Furthermore, as in CREST, the rates of stroke, death, and MI overall were low with each intervention [17].
In our case our patient had severe systemic atherosclerotic disease, he was initially treated with surgical coronary bypass grafting and later hybrid endovascular transcatheter multiple interventions for native coronary, bilateral iliac arteries and right carotid stenting. Regarding his asymptomatic carotid stenosis (RIGHT 80%, LEFT 60%), and as he was a high risk patient for surgical endarterectomy being elderly with multiple co morbidity being post CABG, severe COPD and systemic atherosclerosis, stenting of his right carotid artery was an acceptable intervention with great outcome.
Our case management and outcomes are in agreement with the ACT I trial, the multicenter trial involving patients 79-years of age or younger with asymptomatic severe carotid stenosis, where carotid-artery stenting was noninferior to carotid endarterectomy at 1-year with regard to the primary composite end point of death, stroke, and myocardial infarction within 30-days or ipsilateral stroke within 365-days after the procedure. The rates of stroke and survival after the procedure did not differ significantly between the two study groups over a period of 5-years [17].
Percutaneous intervention with stenting is continuously growing solution for surgical high risk cases and it's becoming more and more cost effective, in our case we had satisfying outcomes from systemic PCI for systemic atherosclerosis.
No Conflict of Interest.