Coronary angiography, Acute coronary syndrome, Atherosclerosis, Wellens' syndrome
ECG: Electrocardiogram; CCU: Cardiac Care Unit; LCx: Left Circumflex; RCA: Right Coronary Artery; LAD: Left Anterior Descending; PCI: Percutaneous Coronary Intervention
The abnormal electrocardiogram findings of Wellens' sign that occur in the context of unstable angina are typically associated with significant stenosis in the proximal left anterior descending (LAD) coronary artery. We report an unusual case of a patient who had unstable angina and Wellens' sign, without significant LAD stenosis.
An 81-year-old man with moderate to severe aortic stenosis, hypertension, mild left ventricular hypertrophy, hyperlipidemia, and history of tobacco use presented to the emergency department with subacute-onset intermittent chest pressure at rest, decreased exercise tolerance, and occasional presyncope. At the time of presentation, he was free of symptoms, including chest pain. His blood pressure was 190/91 and he had a grade 3/6 systolic murmur best heard at the right sternal border of the 2nd intercostal space. His presenting electrocardiogram (ECG) showed biphasic T-waves in lead V2 and deeply inverted T-waves in V3 to V6 (Figure 1). These were markedly different from his ECG two years earlier, when his T-waves were upright in these leads (Figure 2 and Figure 3). Serum troponin was negative. A transthoracic echocardiogram re-demonstrated known moderate to severe aortic stenosis and mild concentric left ventricular hypertrophy without evidence of apical hypertrophic cardiomyopathy. Given the concern for hypertensive emergency and unstable angina, he was admitted to the cardiac care unit (CCU), where his blood pressure was lowered with intravenous nitroglycerin and carvedilol, in addition to his outpatient medication, lisinopril. He was also started on other medications for acute coronary syndrome, including aspirin, intravenous heparin, and atorvastatin. The following day, coronary angiography was performed and revealed a 30% distal left main coronary artery stenosis, 95% ostial and 70% mid left circumflex (LCx) artery stenoses (Figure 4), and a 99% ostial right coronary artery (RCA) stenosis (Figure 5). The left anterior descending (LAD) artery had no significant stenosis. Left heart catheterization measurements showed an aortic valve area of 1.1 cm2. After careful consideration of percutaneous and surgical coronary revascularization strategies, the patient was deemed a more suitable candidate for percutaneous coronary intervention (PCI) and underwent successful PCI, with deployment of drug-eluting stents to the LCx and RCA. The T-wave abnormalities on ECG persisted at time of discharge, but the patient's symptoms improved significantly. The T-wave abnormalities ultimately resolved and returned to baseline on his 4 month follow up ECG (Figure 6).
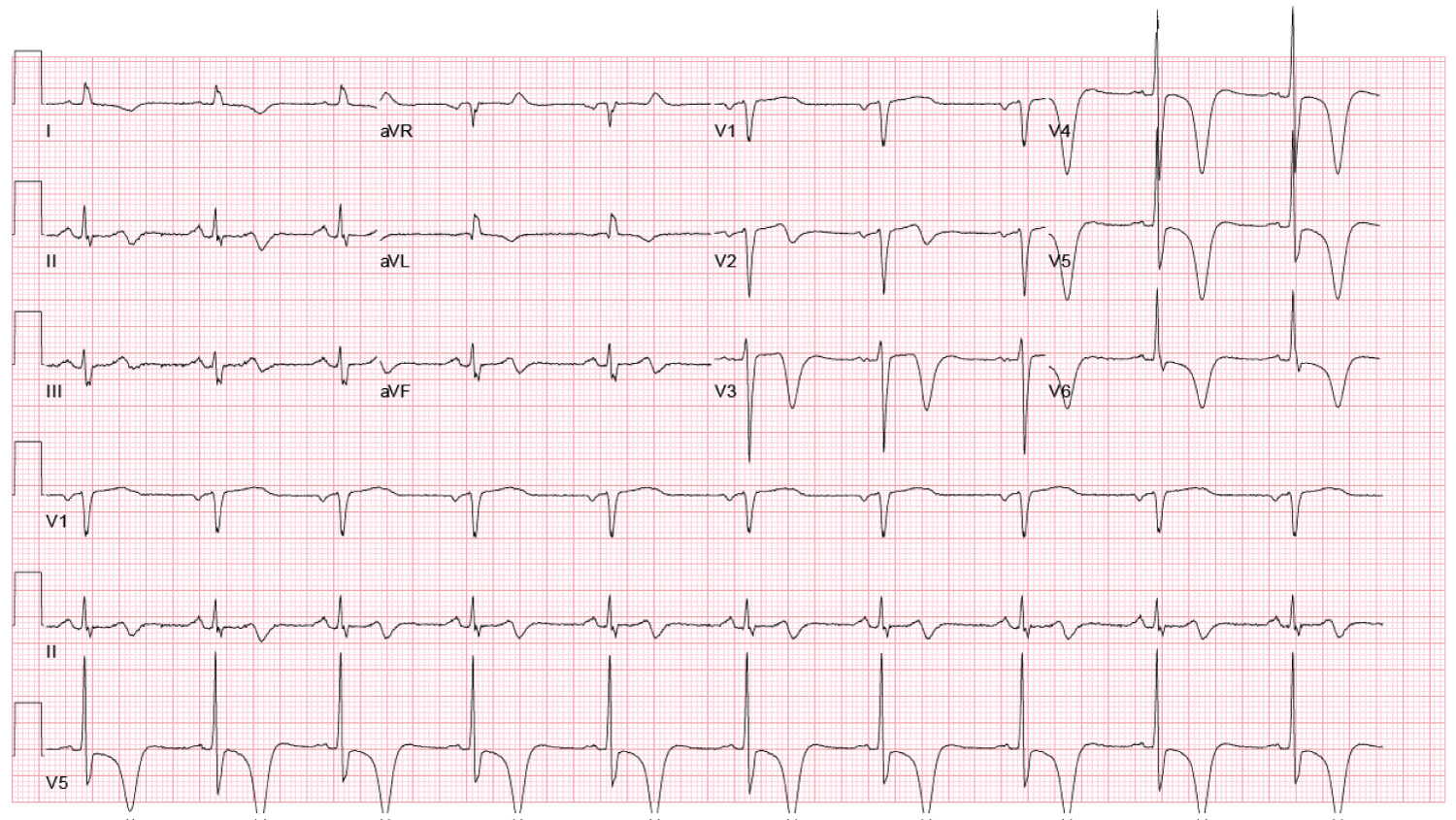 Figure 1: Presenting ECG showing biphasic T-waves in V2 and deep inverted T-waves in V3.
View Figure 1
Figure 1: Presenting ECG showing biphasic T-waves in V2 and deep inverted T-waves in V3.
View Figure 1
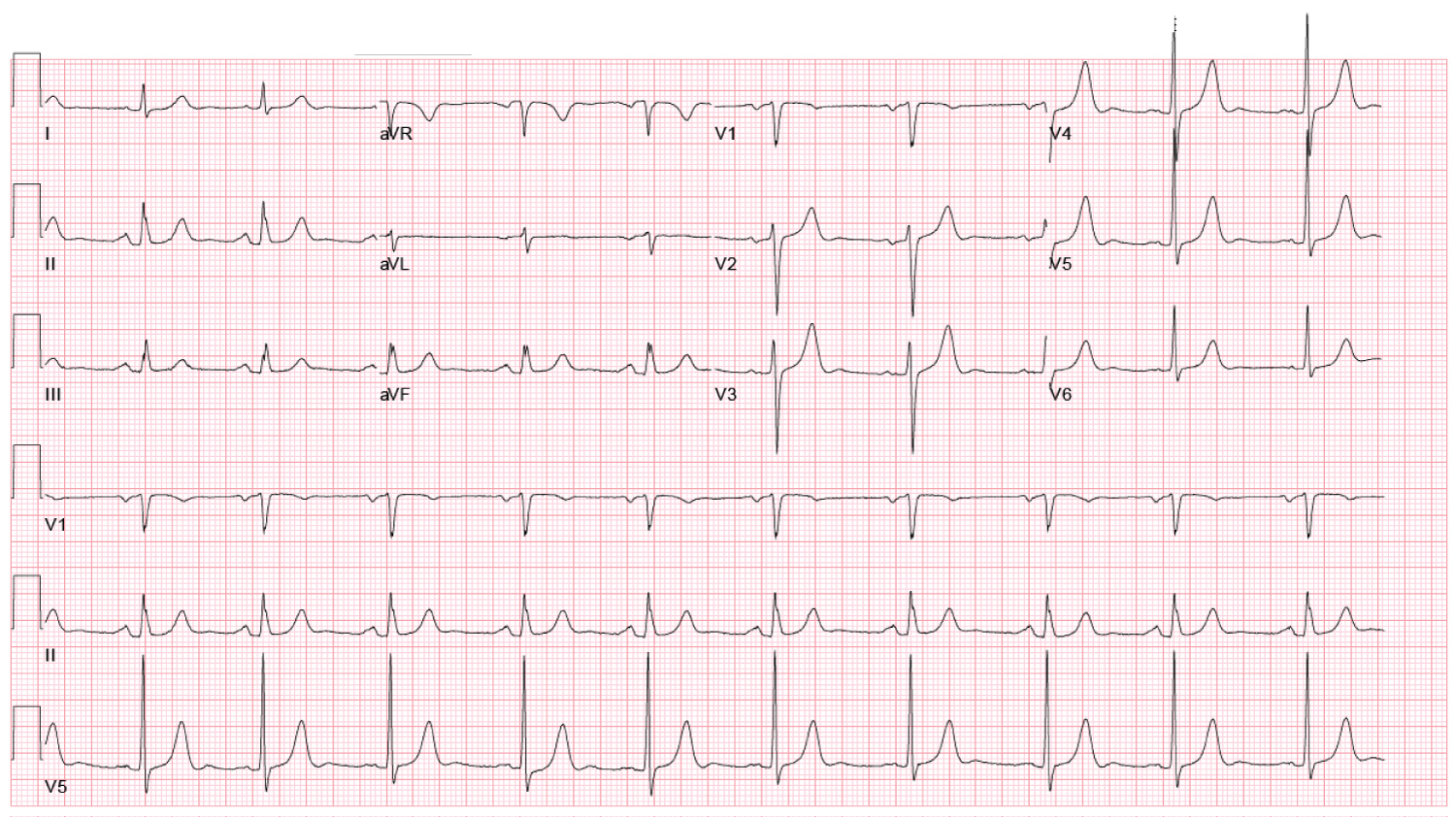 Figure 2: Baseline ECG showing upright T-waves in leads V2-6. View Figure 2
Figure 2: Baseline ECG showing upright T-waves in leads V2-6. View Figure 2
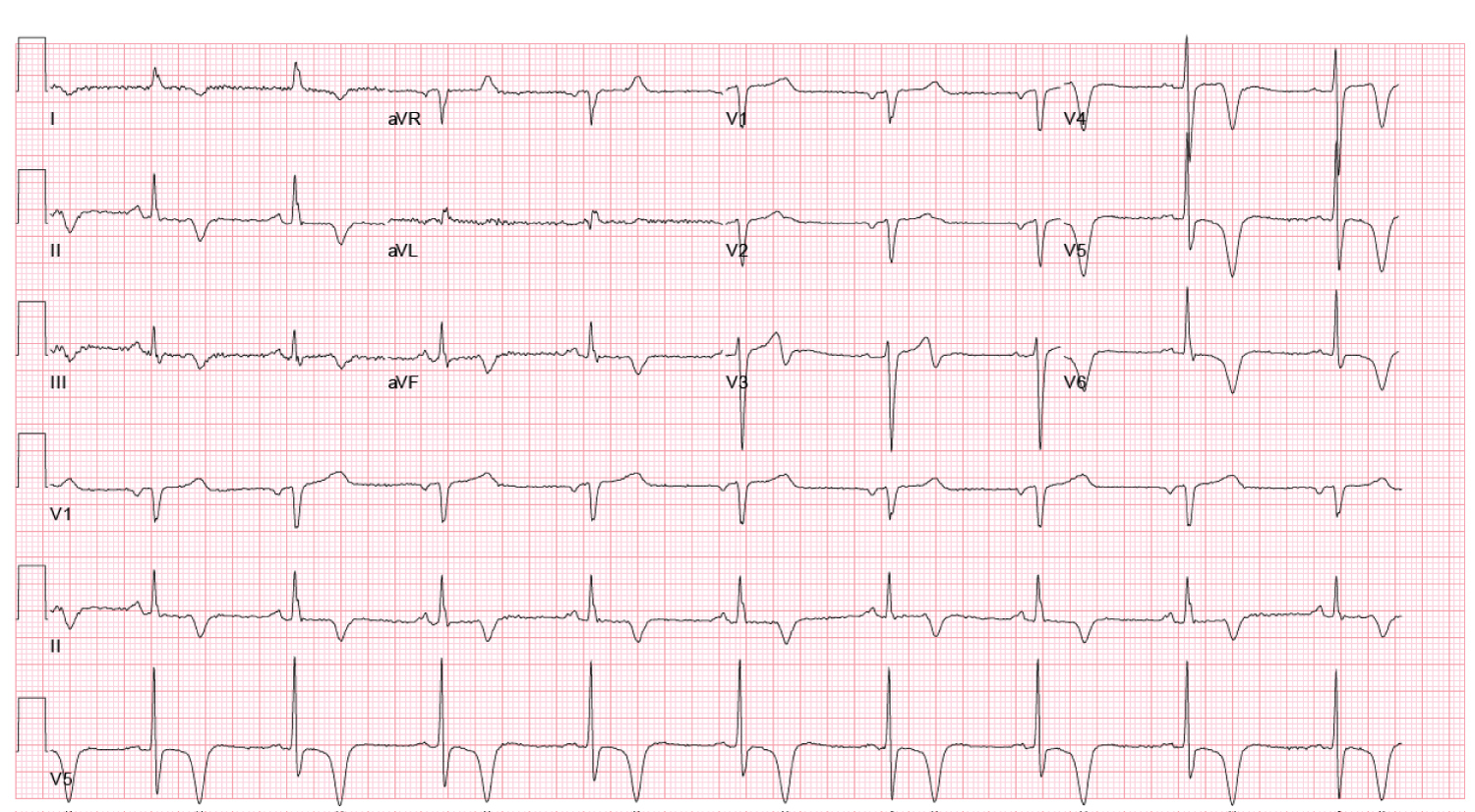 Figure 3: Follow-up ECG 10 day's post-PCI showing interval changes compared to presenting ECG; T-waves are now upright in V2 and biphasic in V3, with persistent inversion in V4-6. View Figure 3
Figure 3: Follow-up ECG 10 day's post-PCI showing interval changes compared to presenting ECG; T-waves are now upright in V2 and biphasic in V3, with persistent inversion in V4-6. View Figure 3
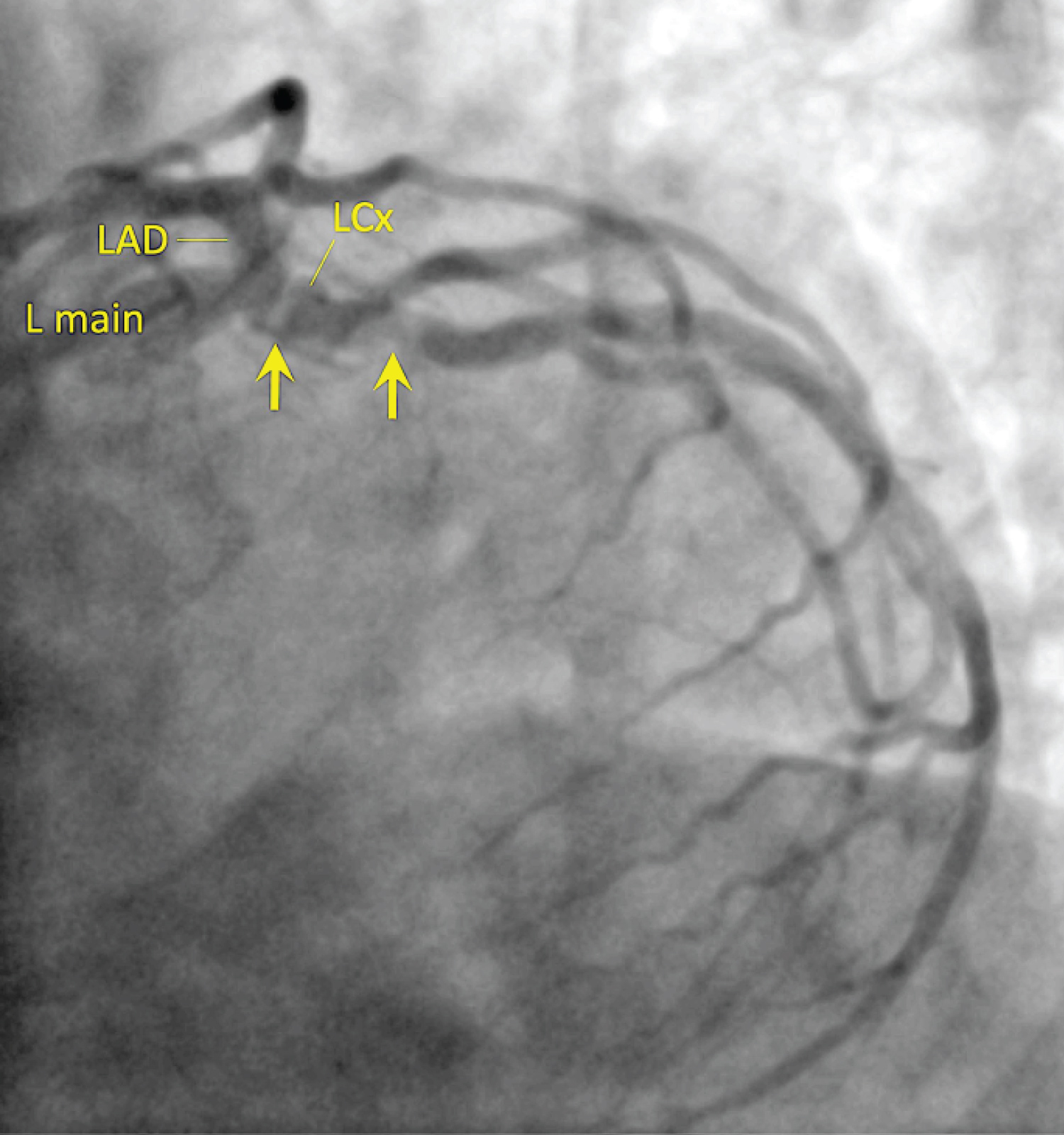 Figure 4: LAO-caudal (extreme "spider") projection showing 95% eccentric, ostial and 70% mid left circumflex (LCx) artery stenoses. View Figure 4
Figure 4: LAO-caudal (extreme "spider") projection showing 95% eccentric, ostial and 70% mid left circumflex (LCx) artery stenoses. View Figure 4
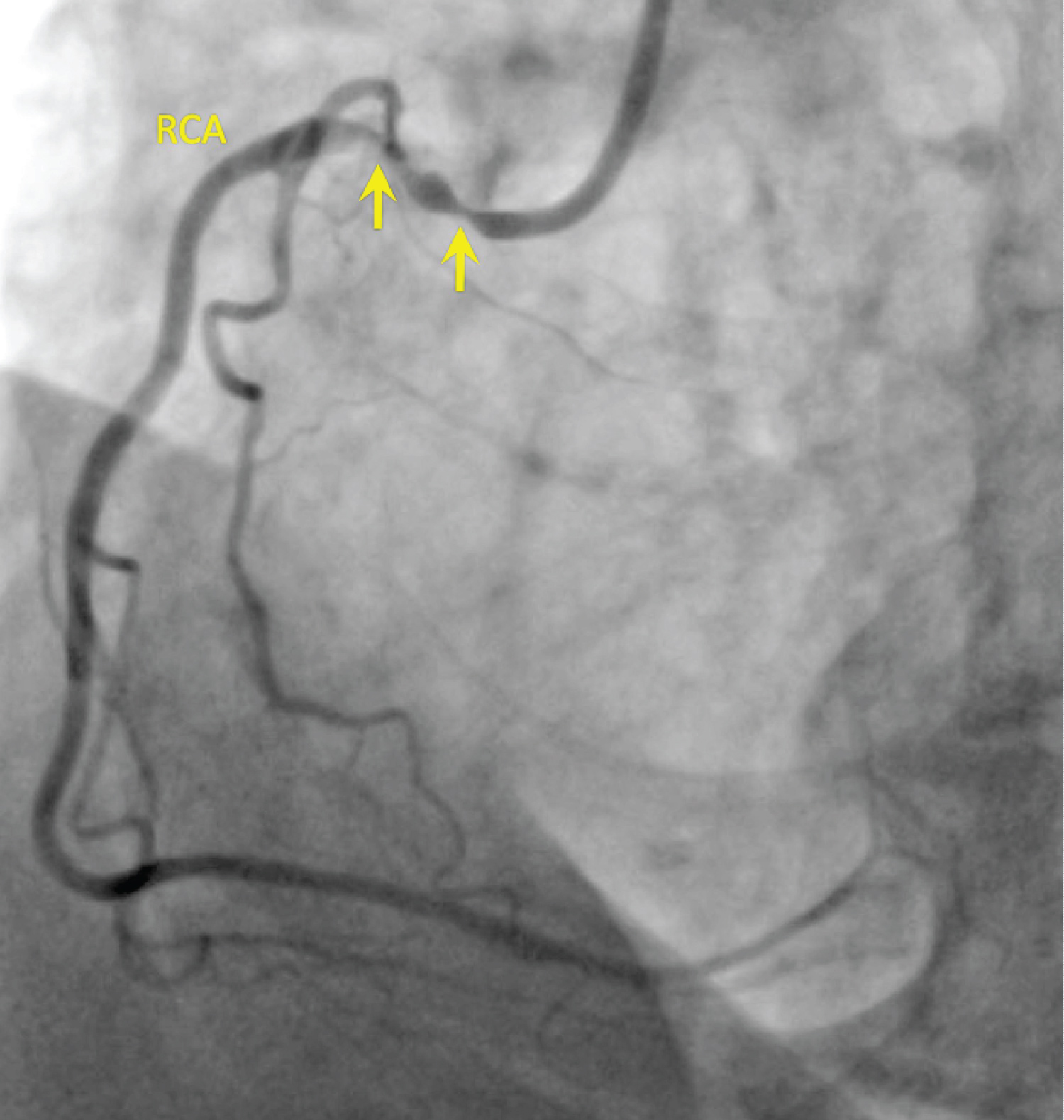 Figure 5: LAO projection showing 90% ostial and 80% proximal right coronary artery (RCA) stenoses. View Figure 5
Figure 5: LAO projection showing 90% ostial and 80% proximal right coronary artery (RCA) stenoses. View Figure 5
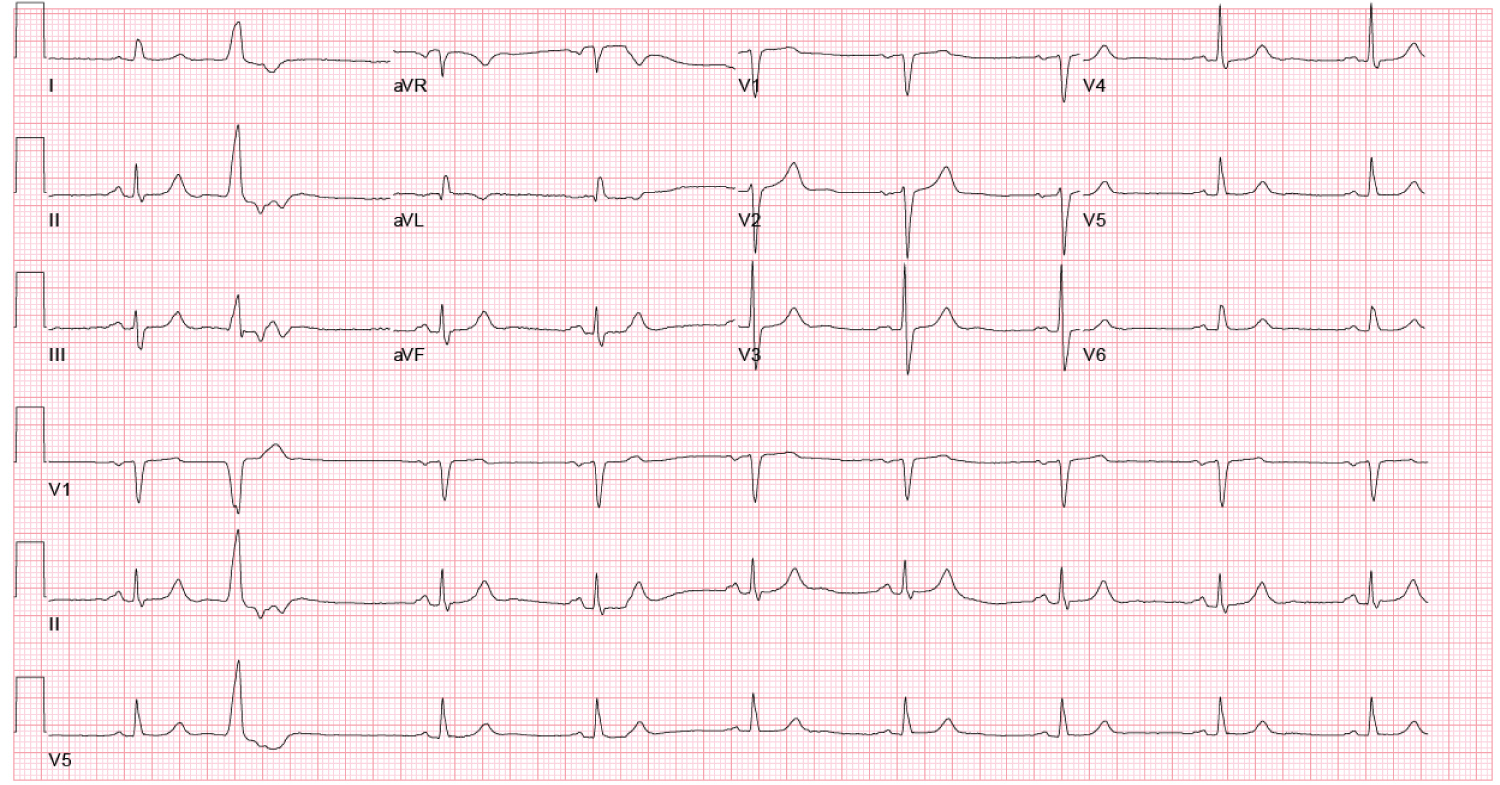 Figure 6: Follow-up ECG 4 month's post-PCI showing complete resolution of T-wave abnormalities in V2-6. View Figure 6
Figure 6: Follow-up ECG 4 month's post-PCI showing complete resolution of T-wave abnormalities in V2-6. View Figure 6
Wellens' sign refers to the abnormal ECG findings of deeply, symmetrically inverted or biphasic T-waves in the precordial leads in the context of unstable angina [1,2]. The T-wave abnormalities often appear after the chest pain has subsided and are not associated with ST-segment elevation, signs of an old anterior wall infarct (i.e., poor R-wave progression or Q-waves in the precordial leads), or serum troponin elevation. The dynamic nature of the T-waves is thought to reflect the waxing and waning of coronary flow during unstable angina. Similar T-wave abnormalities can be found in other conditions, such as an acute intracranial event (e.g., subarachnoid hemorrhage), the apical variant of hypertrophic cardiomyopathy, and stress-induced cardiomyopathy. However, when they are present in the setting of unstable angina, the coronary stenosis is most often found in the proximal LAD [1,2]. This case adds to the small number of published reports describing Wellens' sign in unstable angina but in the absence of significant LAD stenosis [3]. The persistence of the ECG abnormalities for multiple days following PCI may reflect delayed resolution of repolarization abnormalities.
No funding was provided for this case report.
None.