The author has just written a book on the evolution of the specialty of Pediatric Cardiology over the last 50 years [1]. The intent of this review is to present a summary of this book. Because of large amount of this material, the review is separated into four parts. In this first part, transcatheter interventions (balloon angioplasty/valvuloplasty procedures) will be appraised.
Based a thorough review of the literature it appears that Rubio-Alvarez, et al. [2,3] were the very first to do and report transcatheter intervention to treat congenital cardiac defects (CHDs) in 1953; they performed pulmonary valvotomy using a modified ureteral catheter [2,3]. Nearly a decade later Dotter [4], Rashkind [5], Porstmann [6], and their colleagues described progressive dilatation of peripheral arterial stenotic lesions, balloon atrial septostomy, and percutaneous closure of patent ductus arteriosus (PDA), respectively. This and other reviews [7-9] were intended to present historical developments of catheter-based procedures in the treatment of heart disease in children. Historical aspects of 1) Balloon angioplasty/valvuloplasty of valvar pulmonary stenosis, valvar aortic stenosis, fixed subaortic stenosis, native aortic coarctation, postsurgical aortic recoarctation, branch pulmonary artery stenosis, mitral stenosis, cyanotic CHDs with pulmonary oligemia, stenotic bioprosthetic valves, congenital tricuspid and mitral stenosis, truncal valve stenosis, subvalvar pulmonary stenosis, supravalvar pulmonary stenosis (congenital membranous or postoperative), stenosis of the aorta (Leriche syndrome, atherosclerotic and Takayasu's arteritis), baffle obstruction following Mustard or Senning procedure (both systemic and pulmonary venous obstructions), superior and inferior vena caval obstructions, pulmonary vein stenosis, pulmonary veno occlusive disease, vertical vein stenosis in total anomalous pulmonary venous connection, pulmonary venous obstruction following repair of total anomalous pulmonary venous connection, specially designed pulmonary artery bands, cor triatriatum, cor triatriatum dexter, and coronary artery stenotic lesions that develop after Kawasaki disease; 2) Stents to enlarge stenotic lesions of branch pulmonary arteries, systemic veins, systemic and pulmonary venous pathways after Mustard procedure, aorta, right ventricular outflow conduits, pulmonary veins and native right ventricular outflow tract or to keep the ductus arteriosus open in patients with pulmonary atresia and hypoplastic left heart syndrome and maintaining patency of stenosed aorto-pulmonary collateral vessels, surgically created but obstructed shunts or acutely thrombosed shunts as well as covered stents; 3) Trans-catheter occlusion of cardiac defects comprising of atrial septal defect, patent foramen ovale (PFO), PDA, ventricular septal defect (VSD), and aorto-pulmonary window; and 4) Catheter-based atrial septostomy such as Rashkind balloon atrial septostomy, Park's blade atrial septostomy, balloon angioplasty of the atrial septum, trans-septal puncture and atrial septal stents were reviewed. The historical aspects were presented in a tabular form (Table 1).
Table 1: History of transcatheter interventions for pediatric heart disease*. View Table 1
At first, the pathologic features of pulmonary stenosis were reviewed. This is followed by presentation of historical aspects [7-9], indications [10] and the procedure of balloon pulmonary valvuloplasty (BPV) (Figure 1) [11-13].
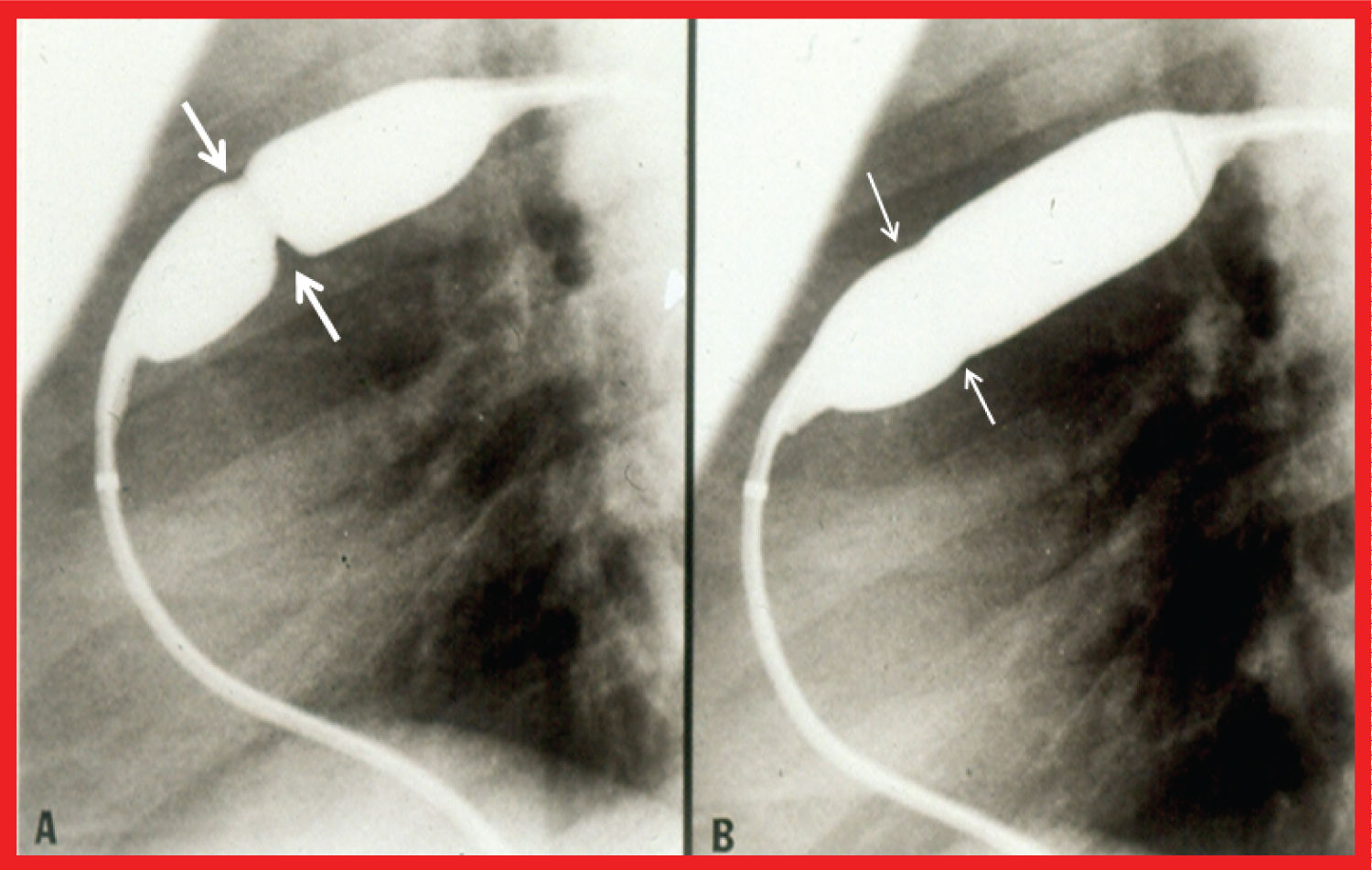 Figure 1: Balloon dilatation catheter placed across the pulmonary valve showing A) "Waisting" of the balloon in the early phases of inflation (thick arrows); B) Which is almost completely abolished with further balloon inflation (thin arrows) [23].
View Figure 1
Figure 1: Balloon dilatation catheter placed across the pulmonary valve showing A) "Waisting" of the balloon in the early phases of inflation (thick arrows); B) Which is almost completely abolished with further balloon inflation (thin arrows) [23].
View Figure 1
The notion of using balloons larger than the annulus of the pulmonary valve to dilate the pulmonary valve with balloons 1.2 to 1.4 times the pulmonary valve annulus was conceived on the basis of immediate [14] and both immediate and follow-up [15] results. Then, immediate [16,17], intermediate-term [18,19], and long-term [20] follow-up results (Figure 2) were presented which point out excellent results with minimal residual gradients across the pulmonary valve and event-free rates in high-80 s and mid-80 s at 5 and 10 years following BPV, respectively; but, significant increase in frequency of pulmonary insufficiency (PI) was seen during long-term follow-up evaluation [20].
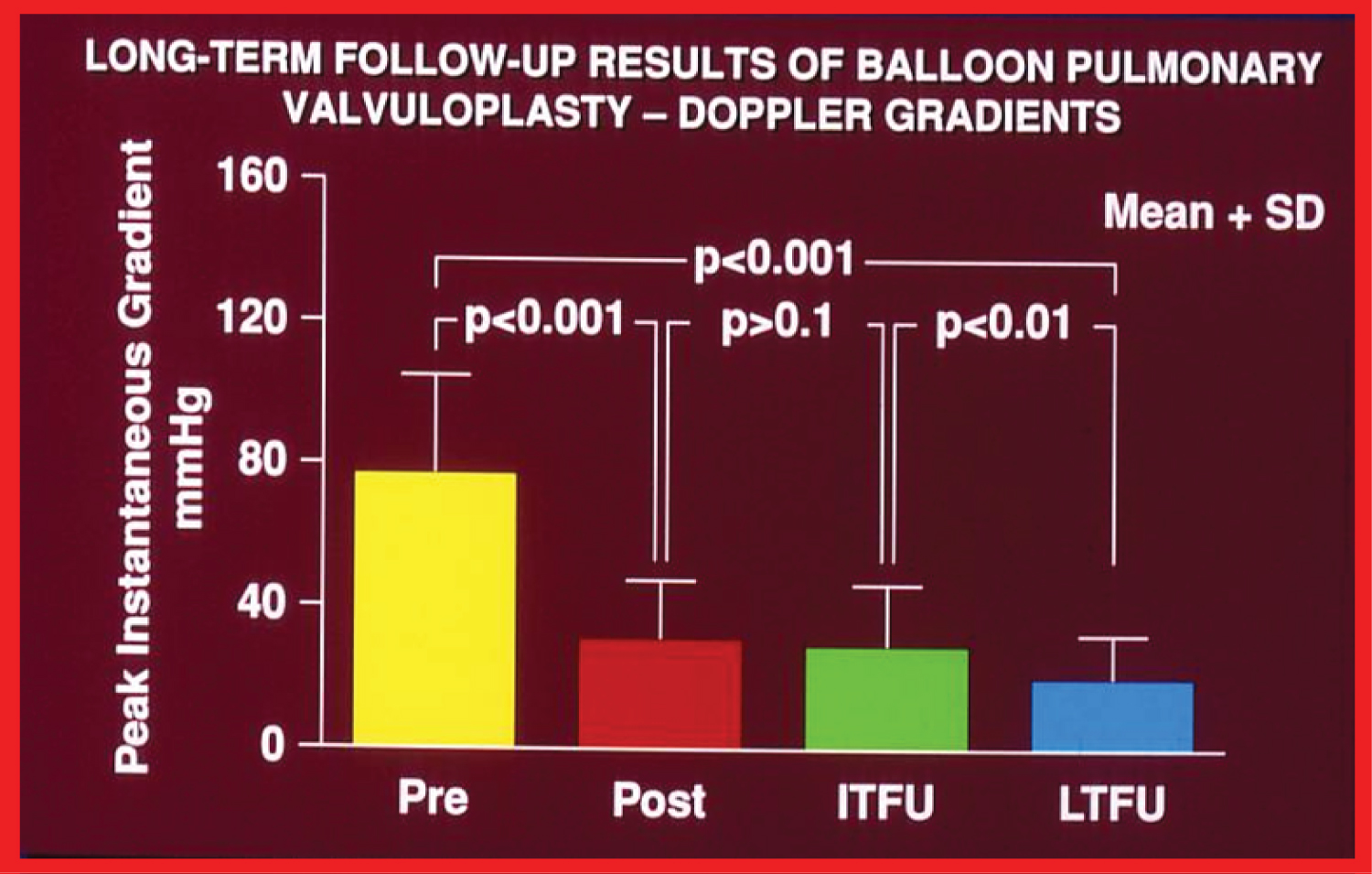 Figure 2: Bar graph showing maximum peak instantaneous Doppler gradients prior to (Pre) and one day following (Post) balloon pulmonary valvuloplasty, and at intermediate-term (ITFU) and long-term (LTFU) follow-up. Note the significant reduction (p < 0.001) after valvuloplasty, which remains unchanged (p > 0.1) at ITFU. However, at LTFU there was a further reduction (p < 0.001) in the Doppler gradients. The mean + standard deviation (SD) are depicted [20].
View Figure 2
Figure 2: Bar graph showing maximum peak instantaneous Doppler gradients prior to (Pre) and one day following (Post) balloon pulmonary valvuloplasty, and at intermediate-term (ITFU) and long-term (LTFU) follow-up. Note the significant reduction (p < 0.001) after valvuloplasty, which remains unchanged (p > 0.1) at ITFU. However, at LTFU there was a further reduction (p < 0.001) in the Doppler gradients. The mean + standard deviation (SD) are depicted [20].
View Figure 2
Restenosis was observed in 8 to 10% of children at intermediate-term follow-up [19-21]. The predictors of restenosis were balloon/annulus ratio < 1.2 and immediate post-valvuloplasty gradient ≥ 30 mmHg [21]. Repeat BPV for relief of restenosis is feasible and effective [22]. Restenosis that occurs after surgical pulmonary valvotomy can also be relieved by BPV [23]. Infundibular stenosis/gradients develop in nearly 30% patients with higher incidence in the older patients and in those with more severe obstruction [24]. Infundibular gradients higher than 50 mmHg should receive beta blockade therapy [24,25]. The infundibular obstruction regresses at follow-up in the majority of patients with only rare need for surgical intervention [24,25]. Right ventricular filling abnormalities do improve following BPV with consequent reduction/reversal of inter-atrial right to left shunt [26]. Relief of pulmonary valve obstruction in patients with dysplastic pulmonary valves is feasible, but may require larger balloons with balloon/annulus ratio of 1.4 to 1.5; the relief of obstruction is dependent upon the presence of commissural fusion [27]. Unsuccessful cases may require surgical excision of the obstructive valve leaflets along with trans-annular patch relief of valve annular obstruction. The role of balloon diameter, balloon length, number of balloons (double vs. single balloon), and pressure, duration and number of balloon inflations on the effectiveness of BPV was also scrutinized [15,28-30]. The mechanism by which BPV produces relief of pulmonary valve stenosis appears to be rupture/tear of the fused valve commissures with infrequent valve leaflet tears or avulsion [31].
Electrocardiogram (ECG) is valuable in demonstrating regression of hypertrophy of the right ventricle following BPV, but ECG confirmation for improvement does not become clear until six months following BPV [32]. Echo-Doppler studies are also useful and dependable non-invasive monitoring techniques; the Doppler gradients are usually indicative of residual obstruction and will also identify PI [33,34]. Residual PI is seen in most of the patients at late follow-up (Figure 3) [20,35-37]. Reducing the balloon/annulus ratio to 1.2 to 1.25 at the time of initial BPV was thought to reduce the degree and prevalence of PI at follow-up [37]; studies to confirm this hypothesis are warranted. There are only a few studies comparing balloon with surgical therapy are available [22]. In the few of these studies, surgical therapy is associated with higher incidence of mortality and morbidity as well as of PI, but with a greater reduction of gradient [22,38]. BPV is also useful in the treatment of the newborn with critical pulmonary stenosis [39-44] and adults with valvar pulmonary stenosis [38,45].
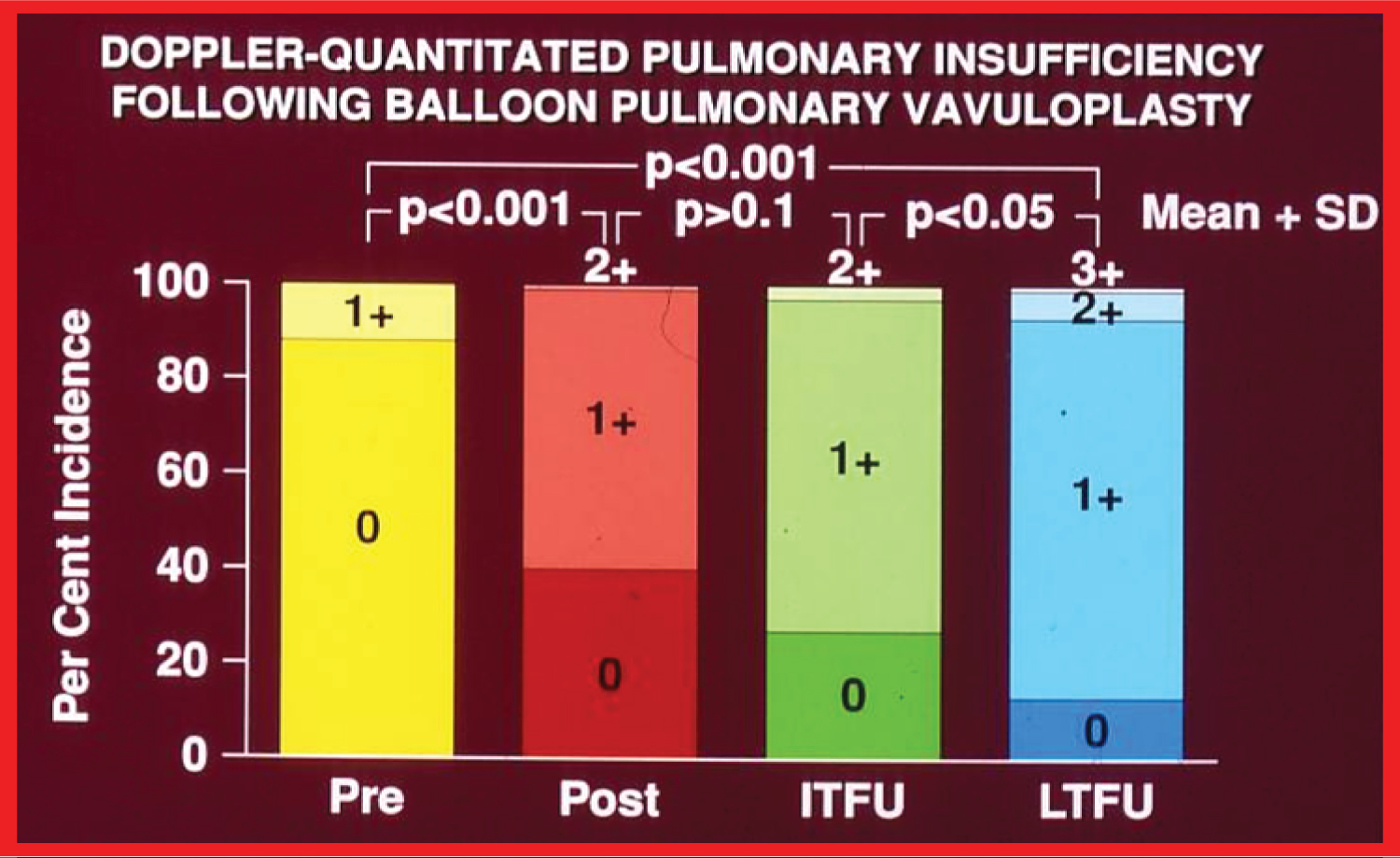 Figure 3: Bar graph demonstrating pulmonary insufficiency (PI) graded by Doppler prior to (Pre) and one day after (Post) balloon pulmonary valvuloplasty and at intermediate-term (ITFU) and long-term (LTFU) follow up. 0, No PI; 1+, 2+, 3+, PI grade. A gradual but significant increase (p < 0.05 to p < 0.001) in the incidence of PI is noted [20].
View Figure 3
Figure 3: Bar graph demonstrating pulmonary insufficiency (PI) graded by Doppler prior to (Pre) and one day after (Post) balloon pulmonary valvuloplasty and at intermediate-term (ITFU) and long-term (LTFU) follow up. 0, No PI; 1+, 2+, 3+, PI grade. A gradual but significant increase (p < 0.05 to p < 0.001) in the incidence of PI is noted [20].
View Figure 3
Historical aspects, indications, procedure of BPV, and immediate and follow-up results in patients with pulmonary stenosis associated with cyanotic CHDs were appraised [46-52]. BPV is recommended if the infant/child needs palliation of pulmonary oligemia but is not a candidate for total surgical correction at presentation. The procedure is indicated if the pulmonary valve obstruction is a significant part of the right ventricular outflow tract stenosis and multiple obstructions in series exist (Figure 4) so that there is likely to be residual subvalvar obstruction following relief of valvar narrowing so that flooding of the lungs is prevented. Increase in systemic arterial saturations immediately after BPV and growth of the pulmonary arteries at follow-up (Figure 5) seem to be the benefits of BPV in this subset of patients.
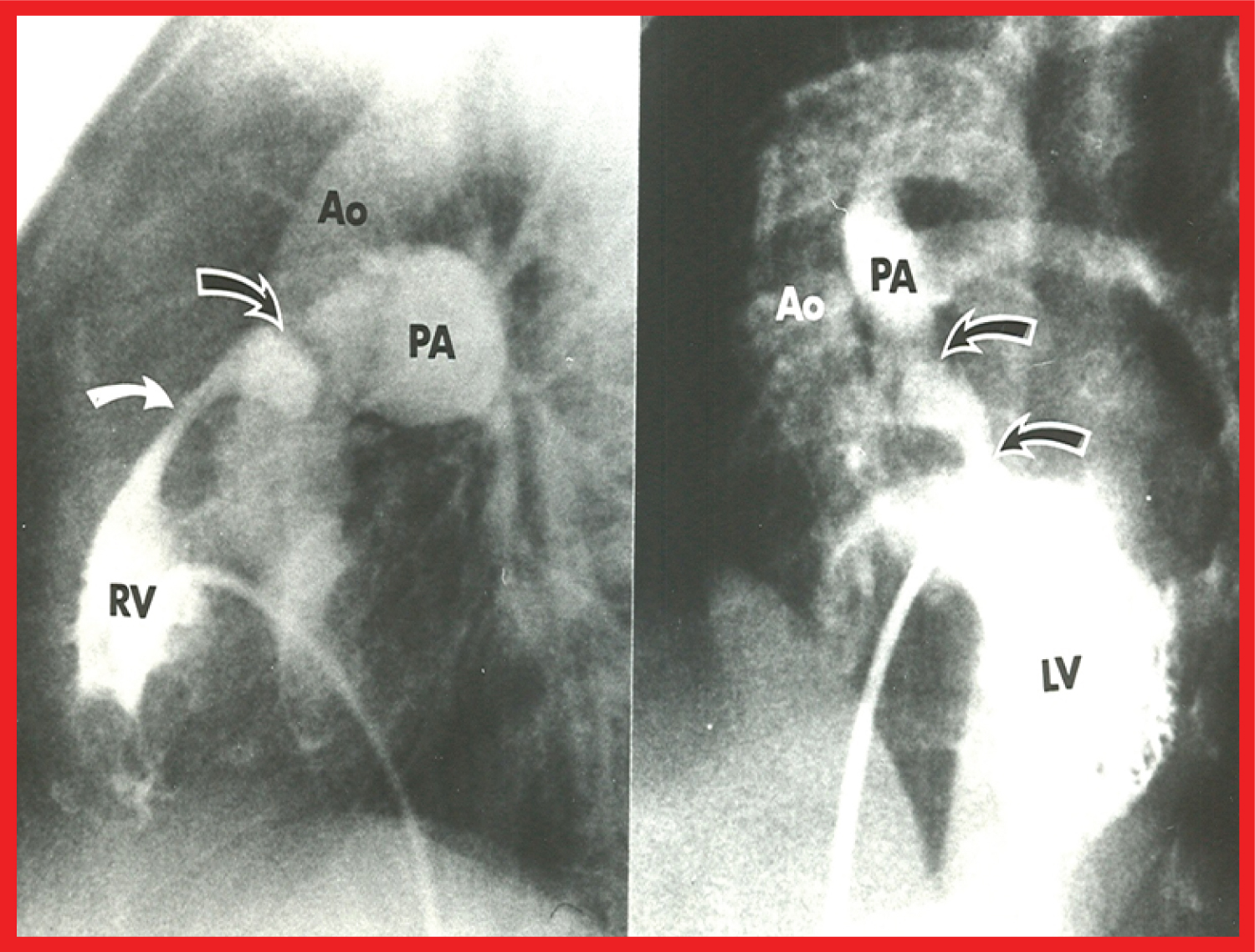 Figure 4: Selected cineangiographic frames from patients with tetralogy of Fallot (left) and d-transposition of the great arteries (right), demonstrating two sites of pulmonary outflow obstruction (two arrows). When the pulmonary valve obstruction is relieved by balloon valvuloplasty, the subvalvar obstruction remains and prevents the flooding of the lungs [48].
Figure 4: Selected cineangiographic frames from patients with tetralogy of Fallot (left) and d-transposition of the great arteries (right), demonstrating two sites of pulmonary outflow obstruction (two arrows). When the pulmonary valve obstruction is relieved by balloon valvuloplasty, the subvalvar obstruction remains and prevents the flooding of the lungs [48].
Ao: Aorta; LV: Left Ventricle; PA: Pulmonary Artery; RV: Right Ventricle
View Figure 4
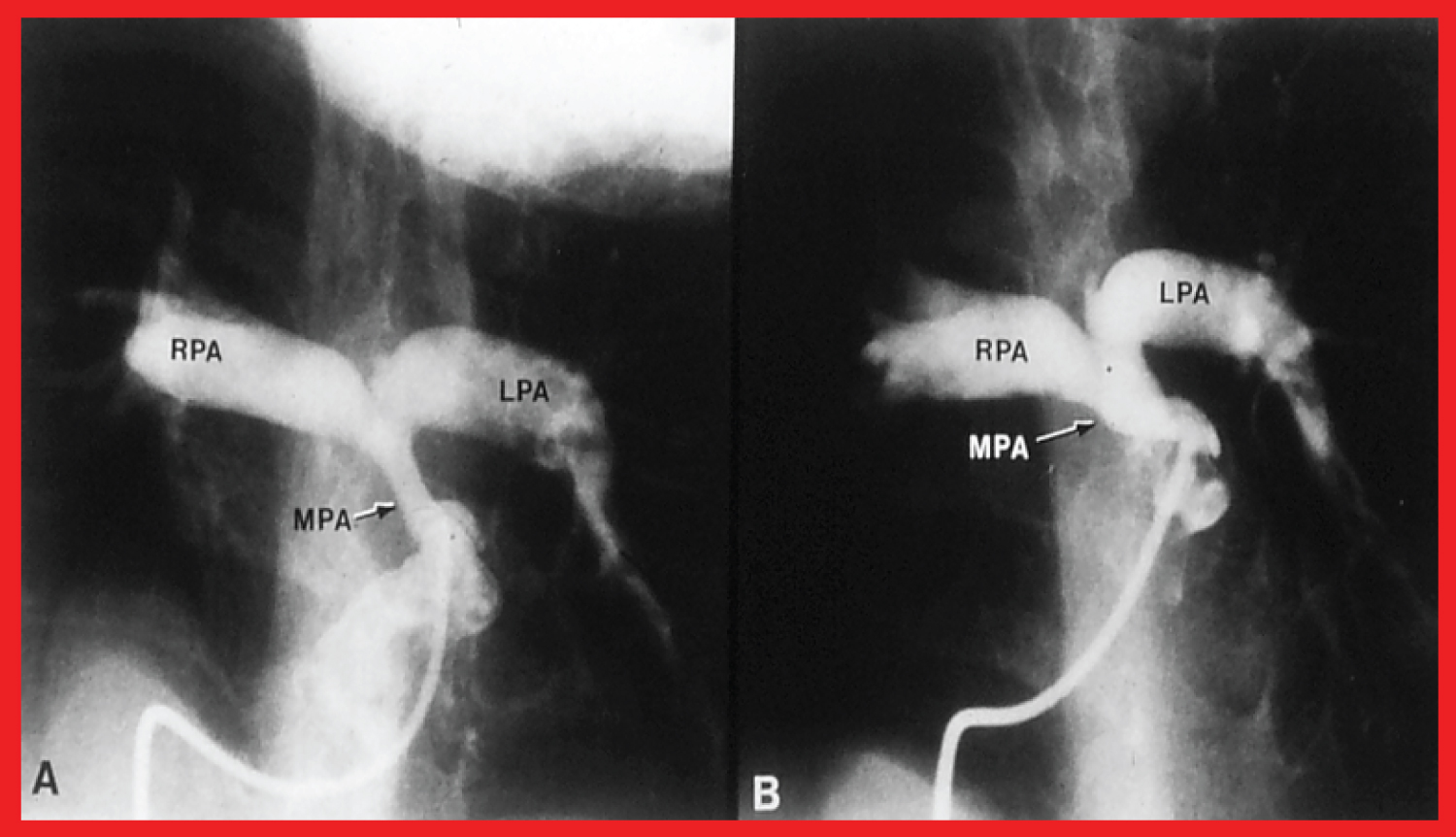 Figure 5: A) Selected frames from pulmonary artery cineangiograms in a sitting-up view in a patient with tetralogy of Fallot, prior to and B) 12 months following balloon pulmonary valvuloplasty. Note the significant improvement in the size of the valve annulus and main pulmonary artery (MPA) at follow-up [48].
Figure 5: A) Selected frames from pulmonary artery cineangiograms in a sitting-up view in a patient with tetralogy of Fallot, prior to and B) 12 months following balloon pulmonary valvuloplasty. Note the significant improvement in the size of the valve annulus and main pulmonary artery (MPA) at follow-up [48].
LPA: Left Pulmonary Artery; RPA: Right Pulmonary Artery
View Figure 5
There are several other cyanotic CHDs that may be benefitted by other types of transcatheter therapeutic methods and these include: 1) Transposition of the great arteries (TGA) with intact ventricular septum: Balloon atrial septostomy and other transcatheter techniques to enlarge the PFO. 2) Severe/critical PS with inter-atrial right-to left shunt: Balloon valvuloplasty. 3) Narrowed systemic-to-pulmonary artery shunts: Balloon angioplasty, stent implantation and 4) Pulmonary atresia with intact ventricular septum: Radiofrequency perforation and balloon valvuloplasty.
There are several intra-cavitary right ventricular obstructions including, isolated infundibular stenosis, double chamber right ventricle, hypertrophic cardiomyopathy involving the right ventricle, and subpulmonary obstructions in morphologic left ventricle in patients with corrected TGA. Most of these can't be addressed with balloon dilatation [53,54]. Supravalvar pulmonary artery stenosis may be produced by multiple causes; discrete obstructive lesions may be adequately relieved by balloon angioplasty while long segment and diffuse obstructive lesions are not amenable to transcatheter balloon therapy [53-55]. Balloon angioplasty of branch pulmonary artery stenosis is successful in only 50% of the patients even when high pressure balloons are used, and in addition, complications and recurrences are high [53,54]. Therefore, endovascular stents are currently used in the management of branch pulmonary artery stenosis.
Initially the pathologic and pathophysiologic features of aortic stenosis were reviewed. This is followed by discussion of historical aspects [7-9], indications [56-58], and procedure of balloon aortic valvuloplasty (BAV) [58,59]. Then a presentation of immediate [56], intermediate-term [57-59] and long-term [60] follow-up results (Figure 6) was made which show good results with low residual gradients across the aortic valve and event-free rates of 80%, 76%, 76% and 60% at 1-, 2-, 5- and 10-year follow-up, respectively following BAV. However, considerable increase in prevalence of aortic insufficiency (AI) was seen during long-term follow-up [60,61]. Restenosis occurs in 23% of children at intermediate-term follow-up [56,62]. The predictors of restenosis were age ≤ 3 years and immediate post-valvuloplasty gradient ≥ 30 mmHg [56,62]. Repeat BAV for restenosis is feasible and effective [56]. Restenosis that follows after surgical valvotomy can also be relieved by BAV [57,22]. Subvalvar gradients develop in a very small percentage of patients and resolve with time [58]. The effect of balloon diameter, balloon length, number of balloons (double vs. single balloon), and pressure, duration and number of balloon inflations during BAV was also scrutinized [56-58,63]. The mechanism by which BAV relieves aortic valve obstruction is by rupture/tear the fused commissures with occasional valve leaflet tear or avulsion [31,55,57,58].
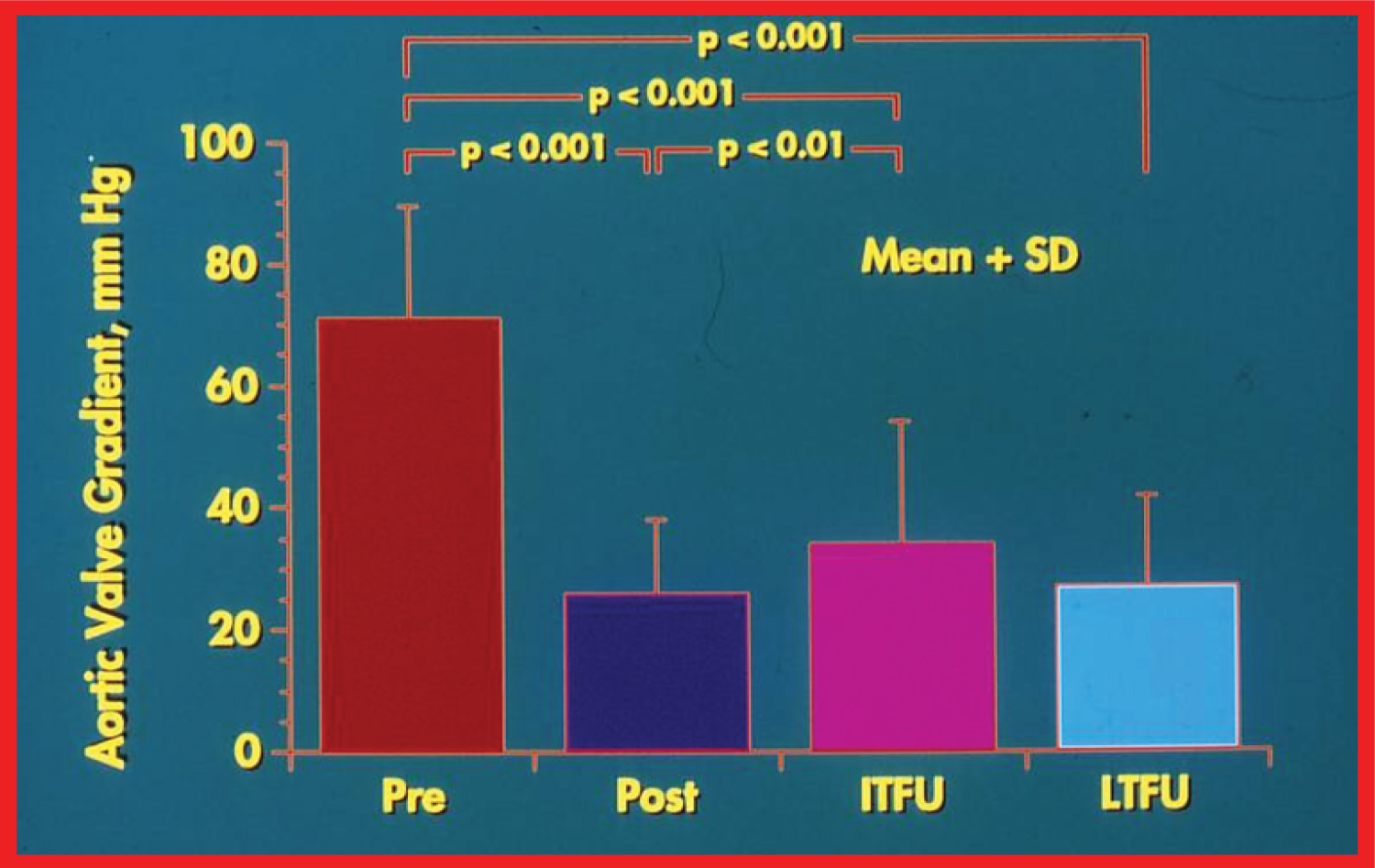 Figure 6: Bar graph showing maximal peak instantaneous Doppler gradients before (Pre) and 1 day after (Post) balloon aortic valvuloplasty, and at intermediate term (ITFU) and late (LTFU) follow-up. There was a significant reduction (p < 0 ~ 001) in the gradient after balloon aortic valvuloplasty which remained essentially unchanged (p > 0.1) at ITFU (12 ± 5 months) and at LTFU (3 to 9 years [mean 6 years]). Doppler-derived maximal peak instantaneous gradients at follow-up continued to be lower (p < 0.001) than pre-valvuloplasty gradients.
View Figure 6
Figure 6: Bar graph showing maximal peak instantaneous Doppler gradients before (Pre) and 1 day after (Post) balloon aortic valvuloplasty, and at intermediate term (ITFU) and late (LTFU) follow-up. There was a significant reduction (p < 0 ~ 001) in the gradient after balloon aortic valvuloplasty which remained essentially unchanged (p > 0.1) at ITFU (12 ± 5 months) and at LTFU (3 to 9 years [mean 6 years]). Doppler-derived maximal peak instantaneous gradients at follow-up continued to be lower (p < 0.001) than pre-valvuloplasty gradients.
View Figure 6
Echo-Doppler studies are helpful and are reliable non-invasive monitoring techniques; the Doppler gradients usually reflect residual obstruction and will also identify AI [56-58,60,61]. Significant residual AI is seen in 24 to 38% of patients at late follow-up (Figure 7). Quantity of immediate post-valvuloplasty AI appears to predict development of late AI; however, the causes of AI are not known [60,61,64]. There are only a few studies comparing balloon with surgical treatment [58,59,61]. Based on these limited data, it appears that BAV is an attractive alternative to surgical valvotomy [58,59,61]. BAV is also useful in the management of the neonate with critical aortic valve stenosis [41-44,58] and adults with valvar aortic stenosis [64,65].
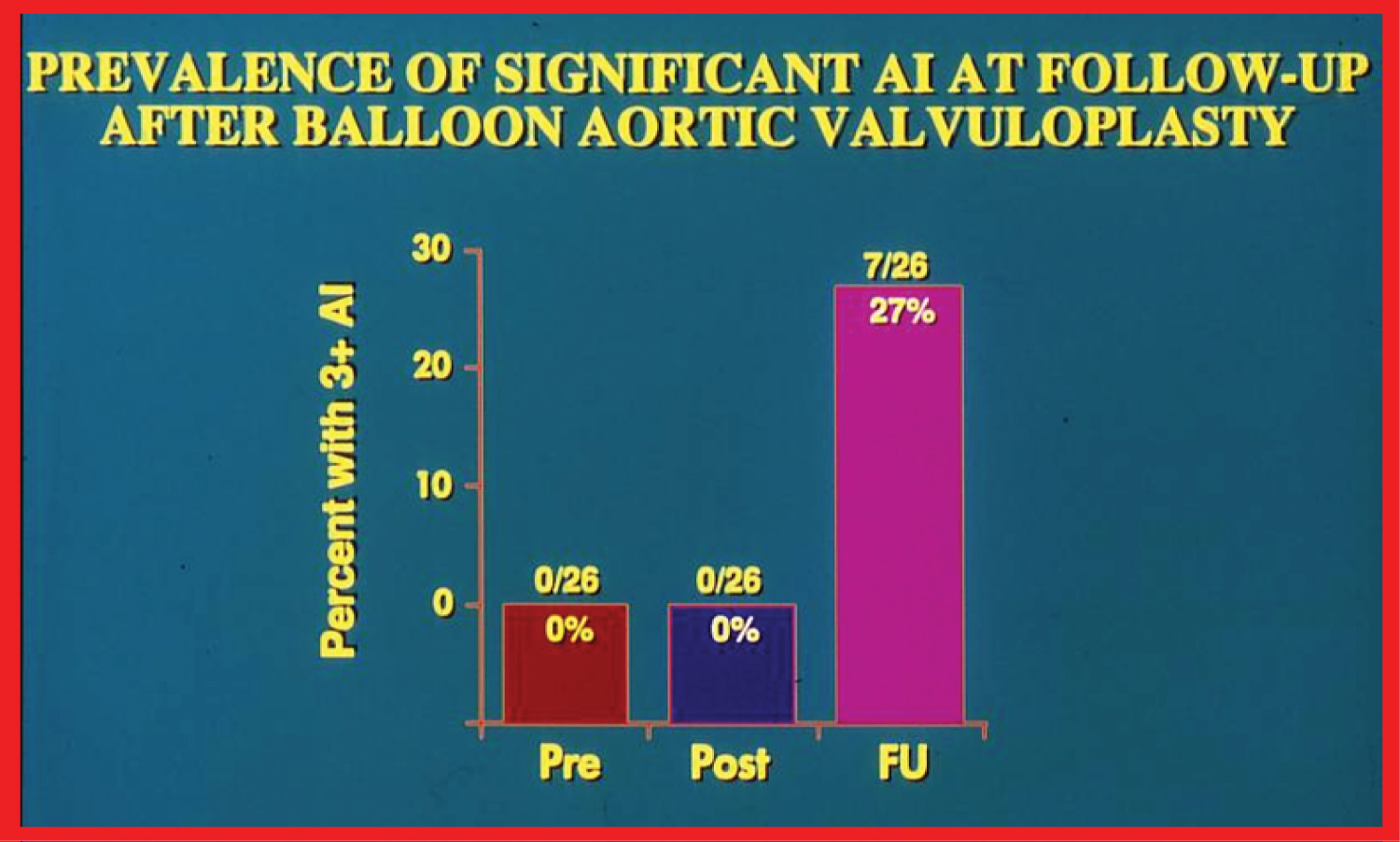 Figure 7: Bar graph demonstrating the prevalence of grade III aortic insufficiency (AI) prior to (Pre), immediately following (Post) balloon aortic valvuloplasty and at late follow-up (FU). Note the significant increase of AI at late follow-up [61].
View Figure 7
Figure 7: Bar graph demonstrating the prevalence of grade III aortic insufficiency (AI) prior to (Pre), immediately following (Post) balloon aortic valvuloplasty and at late follow-up (FU). Note the significant increase of AI at late follow-up [61].
View Figure 7
We examined the prevalence of abnormalities of arterial pulse and limb growth in patients who have undergone trans-femoral artery balloon dilatations by a comparison of three groups of patients, namely, trans-femoral artery balloon dilatations, retrograde femoral arterial catheterization, and control subjects [66]. Children who had trans-femoral artery balloon dilatation exhibited superficial femoral artery compromise, but did not have significant retardation of limb growth. This was presumed to be related to development of collateral circulation in children [66].
A review of historical aspects [7-9,67], indications [67-69], procedure of balloon dilatation [67,68], and immediate and follow-up results in patients with fixed subaortic membranous stenosis [68] was undertaken. Good results were seen when the membrane was thin, less than 2 mm [68-70]. The results were poor in patients with thick fibro-muscular ridge and long tubular fibro-muscular tunnel types of subaortic stenosis. Because the immediate and intermediate-term results of balloon dilatation of fixed subaortic membranous stenosis, when it is thin, are encouraging, balloon dilatation may be considered as treatment of choice in the initial management of this type of discrete subaortic membranous stenosis [68-71].
At first the pathologic features of coarctation of the aorta (CoA) were reviewed. Then, a description of historical aspects [7-9], indications [72-75], and the procedure of balloon angioplasty (Figure 8) ensued [73-75].
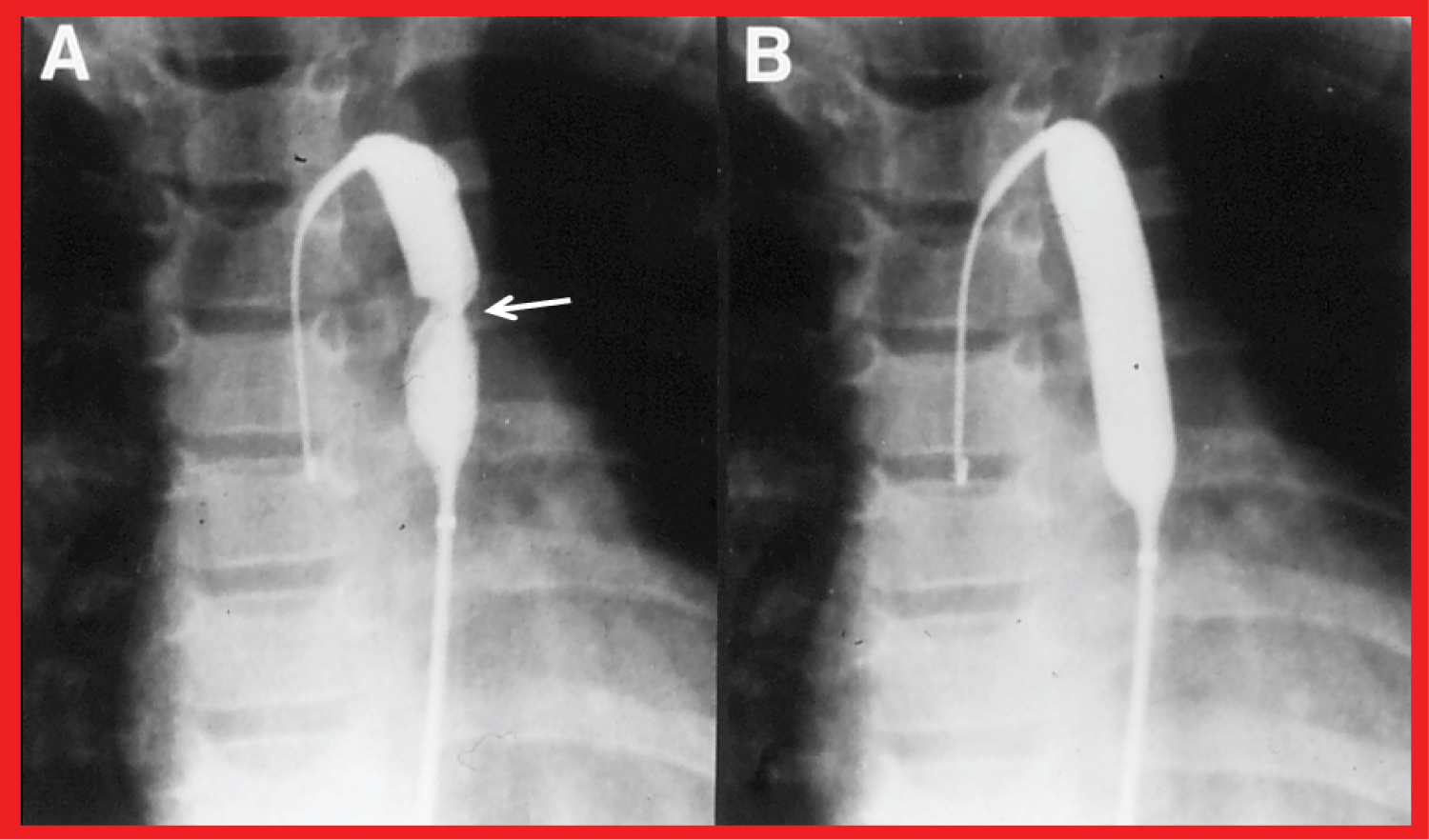 Figure 8: Selected cineflurograpic frames in postero-anterior projection in a child, demonstrating an angioplasty balloon across the aortic coarctation with A) Waisting (arrow) of the balloon during the initial phases of balloon inflation; B) The waist has completely disappeared; with further balloon inflation. The guide wire (GW) is positioned in the ascending aorta (AAo) [73].
View Figure 8
Figure 8: Selected cineflurograpic frames in postero-anterior projection in a child, demonstrating an angioplasty balloon across the aortic coarctation with A) Waisting (arrow) of the balloon during the initial phases of balloon inflation; B) The waist has completely disappeared; with further balloon inflation. The guide wire (GW) is positioned in the ascending aorta (AAo) [73].
View Figure 8
This is followed by a presentation of immediate [17,76], intermediate-term [77-80], and long-term [81] follow-up results (Figure 9). These data indicated that immediate and intermediate-term results are excellent for native CoA; however, recoarctation can develop necessitating re-intervention. Aneurysms may occur, but uncommon. During long-term follow-up normal arm blood pressures in most and low blood pressure-determined gradient between arms and legs were demonstrated [81]. Actuarial reintervention rates were shown to be age dependent, the younger the age at initial balloon angioplasty higher the necessity for reintervention (Figure 10) [81]. The balloon angioplasty technique is equally applicable to adult patients with coarctation [82].
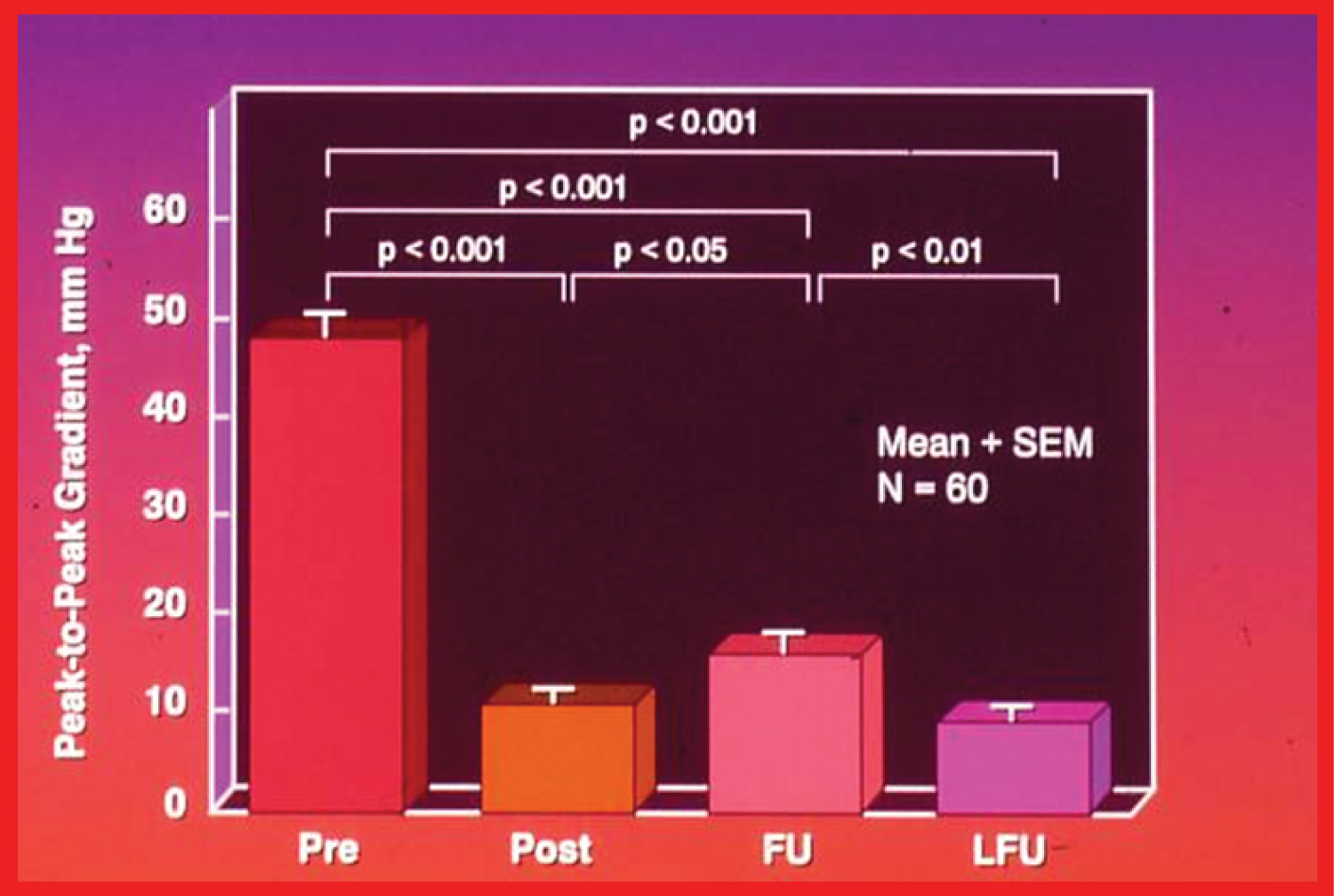 Figure 9: A bar graph of results following balloon angioplasty of native aortic coarctation is shown. The peak-to peak systolic pressure gradients across the coarctation decreased significantly (p < 0.001) from their previous values (Pre) to immediately after (Post) balloon angioplasty. However, the gradient increased (p < 0.05) slightly at intermediate-term follow-up (FU). But, these gradients continued to be lower (p < 0001) than the pre-angioplasty values. At long-term follow-up (LFU) the arm-leg peak systolic pressure difference, measured by blood pressures, was lower than the coarctation gradients prior to (p < 0.001) and at intermediate-term follow-up (p < 0.01). The mean + SEM (standard error of mean) are shown. N: number of patients undergoing balloon angioplasty [81].
View Figure 9
Figure 9: A bar graph of results following balloon angioplasty of native aortic coarctation is shown. The peak-to peak systolic pressure gradients across the coarctation decreased significantly (p < 0.001) from their previous values (Pre) to immediately after (Post) balloon angioplasty. However, the gradient increased (p < 0.05) slightly at intermediate-term follow-up (FU). But, these gradients continued to be lower (p < 0001) than the pre-angioplasty values. At long-term follow-up (LFU) the arm-leg peak systolic pressure difference, measured by blood pressures, was lower than the coarctation gradients prior to (p < 0.001) and at intermediate-term follow-up (p < 0.01). The mean + SEM (standard error of mean) are shown. N: number of patients undergoing balloon angioplasty [81].
View Figure 9
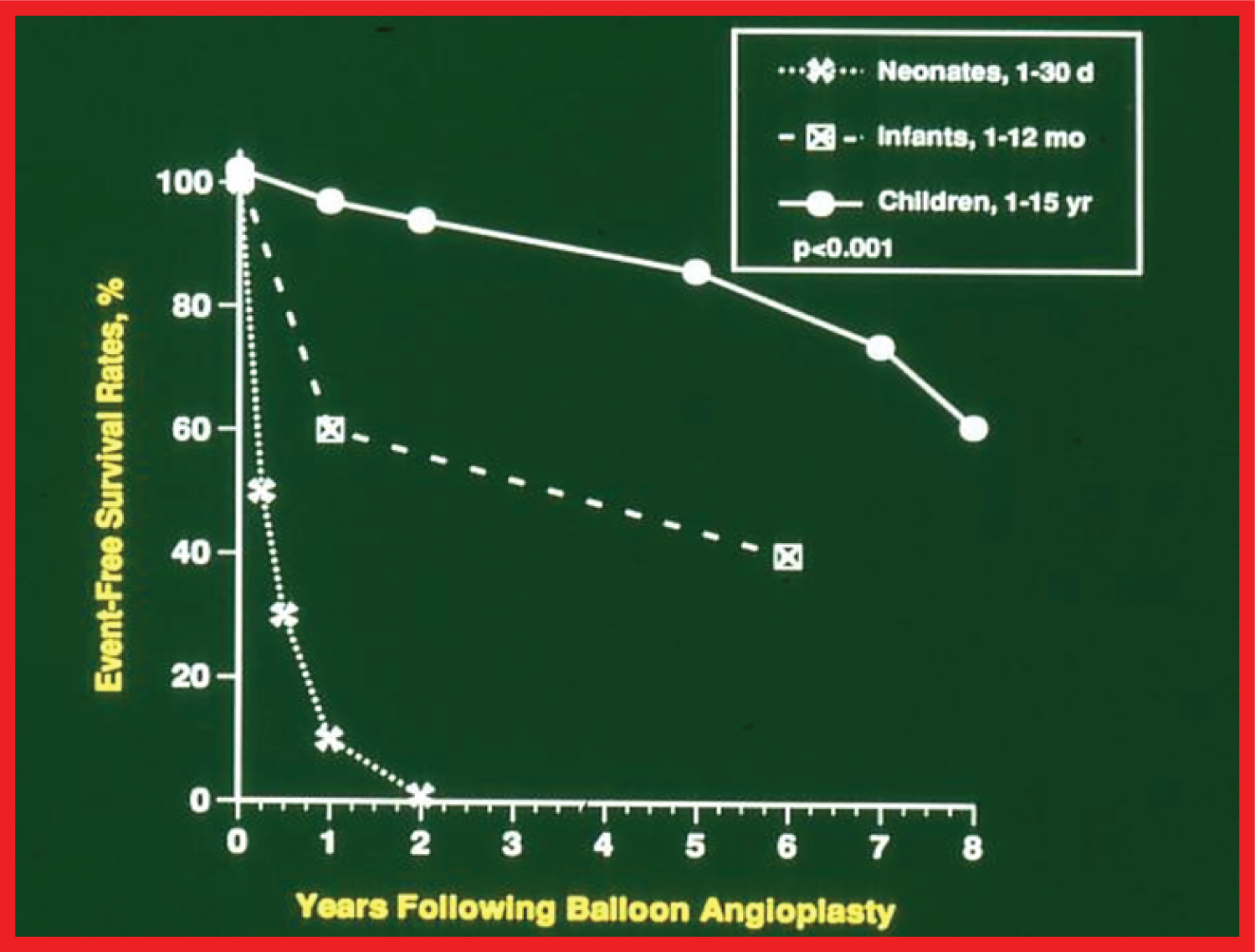 Figure 10: The actuarial event-free survival curves of neonates (< 30 days), infants (1 to 12 months) and children (1 to 15 years) who had undergone balloon angioplasty of aortic coarctation are drawn. The event-free survival rates are better for the children than for the neonates and infants (p < 0.001) [81].
View Figure 10
Figure 10: The actuarial event-free survival curves of neonates (< 30 days), infants (1 to 12 months) and children (1 to 15 years) who had undergone balloon angioplasty of aortic coarctation are drawn. The event-free survival rates are better for the children than for the neonates and infants (p < 0.001) [81].
View Figure 10
Causes of recoarctation were age less than 12 months, aortic isthmus less than 2/3 the size of the ascending aorta immediately proximal to the right innominate artery, coarcted aortic segment less than 3.5 mm before dilation, and coarcted aortic segment less than 6 mm after angioplasty; the higher the number of risk factor, the greater the probability of recoarctation [83]. When restenosis occurs, repeat balloon dilatation is feasible and effective in relieving obstruction [22]. Aneurysm may develop following balloon angioplasty, this phenomenon is similar to that seen after surgical procedures. Remodeling of aorta occurs and the aorta assumes a more uniform shape following successful balloon dilatation [84]. Biophysical response of coarcted aortic segment to balloon angioplasty was studied which demonstrated poor recoil in the patients with recoarctation indicating that elastic properties may not have been preserved in the patients with recoarctation [85]. Effect of technical factors on balloon angioplasty results, mechanism of relief of stenosis by balloon angioplasty and utility of echo-Doppler studies in the assessment of results of balloon angioplasty were also reviewed [78]. Comparison of balloon with surgical therapy is problematic. The efficacy of balloon angioplasty appears to be similar to that of surgery and the mortality rates are also similar and are likely to be related to the associated cardiac defects. However, the morbidity and complication rates are higher with surgical intervention than with balloon dilatation [86,87]. The controversy with regard to whether balloon angioplasty should be used instead of surgery for native coarctation [88-90] was also reviewed.
The author made several other contributions to the literature which included: trans-ductal balloon angioplasty [91], balloon angioplasty of long segment coarctation [92], and revisiting balloon angioplasty of coarctation in the neonate and young infant to test a hypothesis that balloon angioplasty offers successful palliation, defined as avoiding surgery for 4 weeks along with control of congestive heart failure [93,94] were also discussed.
Although the author initially advocated balloon angioplasty in the neonate, because of high rate of recurrence documented in his and other investigators' experience and common occurrence of varying degrees of hypoplasia of the transverse aortic arch and isthmus in the neonate, surgery is now accepted as preferred alternative in the newborn. Nonetheless, balloon angioplasty of coarctation has a valuable role in critically ill young babies [92,95-97], specially if avoidance of anesthesia or aortic cross-clamping required for surgery is important in the overall management of the baby. In addition, the present trend at the majority of institutions is that the type of intervention to tackle coarctation is mostly dependent upon the age of the patient at presentation and the anatomy of coarctation site (discrete vs. long segment and presence of aneurysms) [98].
Despite acceptable short-term and long-term results of balloon dilatation, some problems remain and include, likelihood of aortic rupture, aneurysm formation, failure to effectively address long-segment, tubular narrowings, and recurrence of stenosis. Apparently secondary to these reasons, stent therapy for aortic coarctation has achieved acceptance over the past decade and a half [99-102]. Then, future directions were briefly reviewed; because the cellular mechanisms for recoarctation are unknown, keeping the coarctation segment open mechanically appears to be an available option. However, the stents do not expand as the child grows; this issue may be addressed by possible uses of biodegradable, growth and "dilatable" types of stents [93,103].
A review of historical aspects [7-9,104], indications [86,105,106], procedure of balloon angioplasty itself [86,105-107], immediate results [86,105], and intermediate-term [78,80,105,106], and long-term [75,106] follow-up results of post-surgical recoarctation was undertaken. The immediate and follow-up results of balloon angioplasty of postsurgical aortic recoarctation indicate low residual gradients (Figure 11) and normal blood pressures in most of the patients [75,106]. Nonetheless, the requirement for transcatheter or surgical re-intervention to manage recoarctations, aortic arch/isthmic narrowing and aneurysms in some patients is present. In older subjects, stents may are useful in the treatment of these patients. One of the causes of recoarctation was hypoplasia of the aortic segment proximal to recoarctation site; this is not too dissimilar to the causes of recoarctation following balloon angioplasty of native CoA. Remodeling of the aorta also occurs in post-surgical balloon angioplasty children in a manner similar to that seen with native CoA. A review of usefulness of echo-Doppler studies [86,105,106] in the assessment of results of balloon angioplasty of post-surgical recoarctations and a comparison with surgical therapy was also undertaken [86].
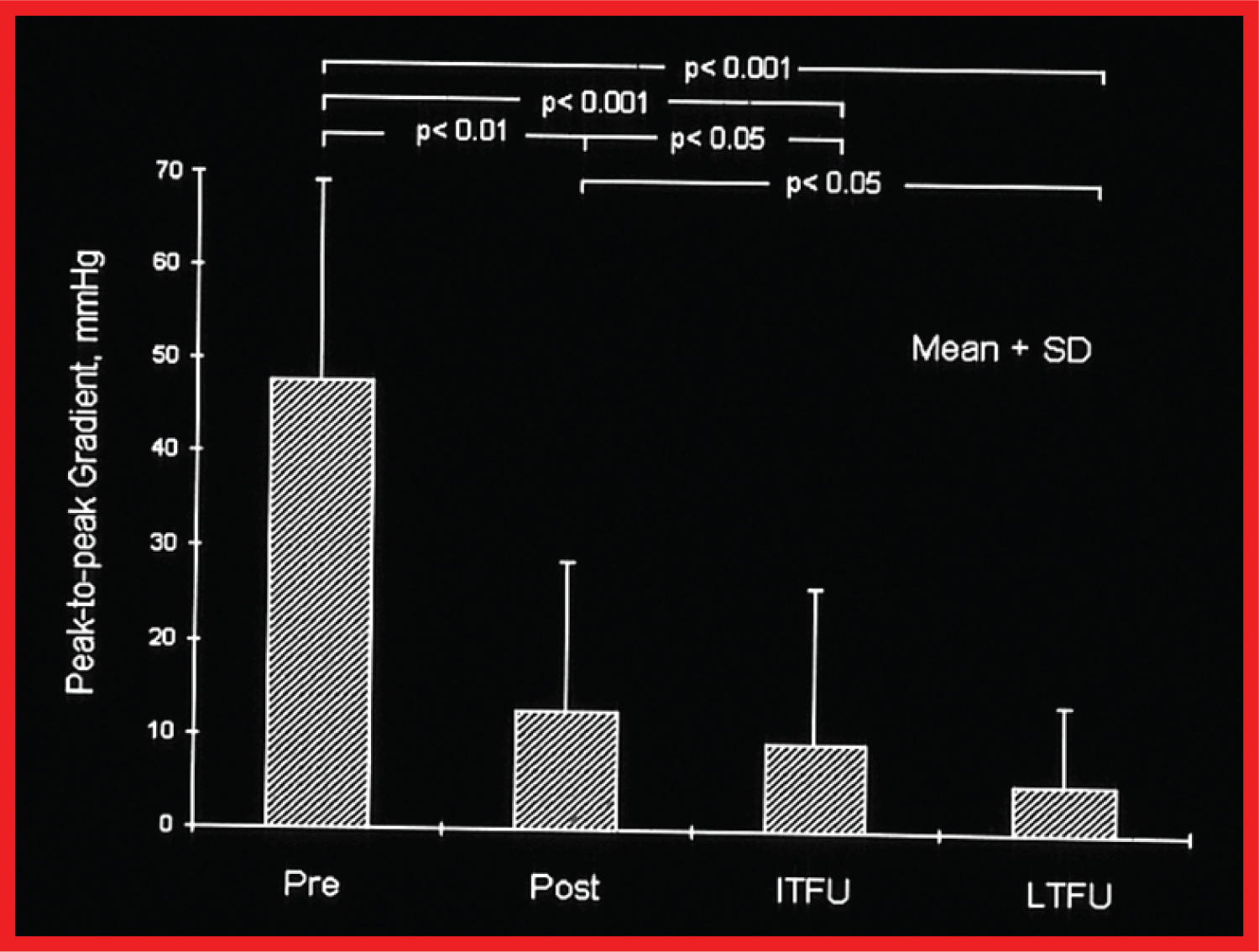 Figure 11: A bar graph of the immediate and follow-up results after balloon angioplasty of postsurgical aortic recoarctation is shown. The peak-to-peak systolic pressure gradients (mmHg) across the coarctation decreased significantly (p < 0.001) from before (Pre) to immediately after (Post) balloon angioplasty. They decreased further (p < 0.05) at intermediate-term (ITFU) and at long- term follow-up (LTFU). The ITFU and LTFU gradients remained remarkably lower (p < 0.001) than those prior to balloon angioplasty. The mean and standard deviation (SD) are shown [106].
View Figure 11
Figure 11: A bar graph of the immediate and follow-up results after balloon angioplasty of postsurgical aortic recoarctation is shown. The peak-to-peak systolic pressure gradients (mmHg) across the coarctation decreased significantly (p < 0.001) from before (Pre) to immediately after (Post) balloon angioplasty. They decreased further (p < 0.05) at intermediate-term (ITFU) and at long- term follow-up (LTFU). The ITFU and LTFU gradients remained remarkably lower (p < 0.001) than those prior to balloon angioplasty. The mean and standard deviation (SD) are shown [106].
View Figure 11
Percutaneous treatment of miscellaneous congenital and acquired obstructive lesions was scrutinized. These are: Narrowed Blalock-Taussig shunts [48,49,108], tricuspid and mitral valve stenoses [109], stenotic bioprosthetic valves (both homografts and heterografts) [110], baffle obstruction following Senning/Mustard operation [111], stenosis of superior and inferior vena cavae [109], obstructed total anomalous pulmonary venous connection [109], obstructed anostomotic site following total anomalous pulmonary venous connection repair [109], PFO [109], PDA [109] and coronary artery stenosis in Takayasu's arteritis [112]. A review of the indications for interventions, the technique of balloon dilatation, and immediate and follow-up results for each of the above, where available, was performed. Balloon therapy indications for are generally similar to those utilized for surgery. The technique involves positioning an appropriate-sized balloon catheter across the stenotic lesion and inflating the balloon two or three times. The balloon size selected is comparable to the valve annulus diameter in the valvar obstructive lesions and two or more times the diameter of the vascular stenoses. In the latter condition, the size of the balloon should not generally exceed 1.5 times the size of the adjacent normal blood vessel. The immediate results following balloon dilatation were excellent in some of the disease entities reviewed above and were marginal in other lesions. There is a dearth of data on the long-term follow-up results. Complications are generally negligible. However, there is no information comparing surgical with balloon therapy. The majority of interventional cardiologists advocated these procedures because there is no requirement for general anesthesia, thoracotomy, cardiopulmonary bypass, and prolonged hospitalization associated with the surgical therapy. Other advantages mentioned are lack of residual scar of the surgery, reduced psychological trauma, and less expense. For vascular obstructive lesions not amenable to balloon angioplasty, employing stents has become a management option [99-102].