This is a case report of a 39-year-old man who presented to the emergency room with atrial fibrillation (AF), pre-excitation, and Ebstein's anomaly (EA). Currently, there was no suggestion of pharmacologic management if the patient declines surgical or catheter ablation therapy. A review of the literature concluded that amiodarone may be a suitable therapy for the pharmacological management of this patient.
This 39-year-old man experienced occasional palpitations but on this occasion, the palpitations were worse with chest pressure during his morning sleep. He visited the emergency department with a pulse rate of 150 per minute, and electrocardiography showed a wide QRS-complex tachycardia in irregular beats (Figure 1) but laboratory tests showed only hypophosphatemia (1.3 mg/dL). Cardioversion was suggested for the developing ventricular tachycardia (VT) and ventricular fibrillation (VF) but he declined. Other suggested intravenous medications were unavailable, so he received a gentle amiodarone infusion which gradually recovered arrhythmia within a few hours. The recovered electrocardiography disclosed Wolff-Parkinson-White (WPW) syndrome. The thyroid function test, followed serum phosphate, and 24-hour electrocardiography were normal. The echocardiography revealed interventricular septal hypertrophy, right atrial and ventricular enlargement, and dislocation of the tricuspid valve toward the apex (Figure 1). With the combination of EA, WPW syndrome, and paroxysmal AF, he refused cardiac ablation. After dosage adjustment over several months, the patient was managed with 200 mg amiodarone daily.
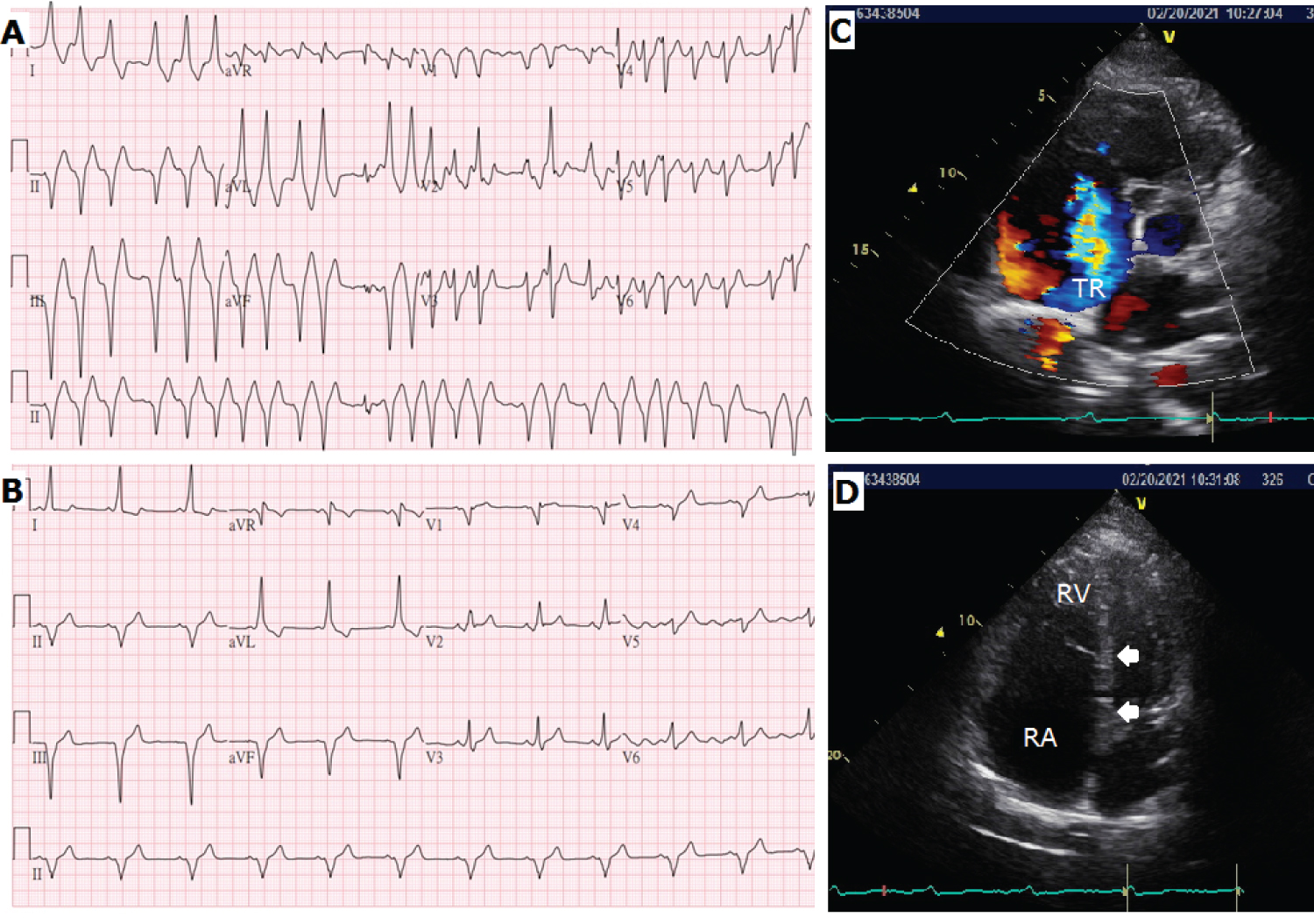 Figure 1: A) Electrocardiography initially showed a heart rate of 150 beats per minute, and the irregular interval without a predictable period indicated atrial fibrillation. There were wide QRS-complexes with varying QRS morphology, which were related to atrial fibrillation with different degrees of aberrant conduction; B) Electrocardiography after successful cardioversion showed a sinus rhythm of 68 beats per minute. The short PR interval (< 120 ms) and a slurred sloping wave (delta wave) were the typical signs of Wolff-Parkinson-White syndrome. The dominant S wave in V1 indicated a right- sided accessory pathway; C) There was significant right atrial (RA) enlargement and moderate tricuspid regurgitation (TR) from the short-axis view of the echocardiograph. The estimated systolic pulmonary artery pressure was 35 mmHg; D) The four- chamber view showed displacement of 29 mm between the insertion site of the septal tricuspid leaflet (upper arrow) and the septal mitral valve (lower arrow). There was a large area of atrialization of the right ventricle (RV), resulting in a very small residual RV. There was no atrial septal defect found in the patient.
View Figure 1
Figure 1: A) Electrocardiography initially showed a heart rate of 150 beats per minute, and the irregular interval without a predictable period indicated atrial fibrillation. There were wide QRS-complexes with varying QRS morphology, which were related to atrial fibrillation with different degrees of aberrant conduction; B) Electrocardiography after successful cardioversion showed a sinus rhythm of 68 beats per minute. The short PR interval (< 120 ms) and a slurred sloping wave (delta wave) were the typical signs of Wolff-Parkinson-White syndrome. The dominant S wave in V1 indicated a right- sided accessory pathway; C) There was significant right atrial (RA) enlargement and moderate tricuspid regurgitation (TR) from the short-axis view of the echocardiograph. The estimated systolic pulmonary artery pressure was 35 mmHg; D) The four- chamber view showed displacement of 29 mm between the insertion site of the septal tricuspid leaflet (upper arrow) and the septal mitral valve (lower arrow). There was a large area of atrialization of the right ventricle (RV), resulting in a very small residual RV. There was no atrial septal defect found in the patient.
View Figure 1
Pre-excited AF (AF with ventricular pre-excitation), supraventricular tachycardia with aberrant conduction, and ventricular tachycardia should be considered for irregular wide-complex tachycardia. The significant irregular RR interval with varying QRS morphology is characteristic of pre-excited AF, in which the electrical impulses via the AP (accessory pathway) exceed the AV nodal pathway. In this condition, intravenous amiodarone, adenosine, and other AV nodal blocking agents may lose the intrinsic inhibition of orthodromic conduction, accelerate the ventricular rate or contribute to VT or VF. According to current guidelines, prompt direct-current cardioversion is recommended for hemodynamically compromised patients, with the administration of intravenous Ibutilide or procainamide to stabilize the patient. Ibutilide and procainamide prolong the refractoriness of both pathways and Ibutilide helps to terminate AF [1]. However, these medications are not easily obtainable, and the intravenous infusion of amiodarone is regarded as a class III recommendation.
In Korea, flecainide was used to maintain sinus rhythm in an older patient with paroxysmal AF and WPW. Flecainide maintains the sinus rate with little effect on the AV nodal refractory period in patients without structural heart disease. The concomitant administration of low dose bisoprolol made the delta wave disappear [2]. In a retrospective review of the administration of intravenous amiodarone for patients with pre-excited AF, most patients (18/30, 60%) achieved sinus rhythm without electrical cardioversion [3]. Intravenous amiodarone for patients with pre-excited AF is a treatment option if the guideline-suggested managements are unavailable or initially undesirable, but not recommended for patients with unstable hemodynamics, extremely high heart rate, multiple comorbidities, and younger patients. The rhythm may become VF at any time, even before the administration of intravenous amiodarone, hence a defibrillator should be readily available.
However, management becomes more complicated when the patient has concurrent EA. Patients with EA may develop cyanosis, exercise tolerance, heart failure, embolization, and arrhythmia. The arrhythmogenic atrialized right ventricle causes AV conduction delay and atrial tachyarrhythmia. The dislocated tricuspid valve elongates the tricuspid annulus, and makes the formation of the right-sided AP, especially on the lower half of the tricuspid annulus [4]. In fact, these patients have more complicated AP. Up to 50% of patients with EA have more AP, multiple AP, or board AP. Surgical or catheter intervention is suggested for symptomatic patients but these procedures are challenging, but it remains a highly effective and curative management [5]. Without intervention, adults with EA are more likely to die from sudden cardiac death rather than heart failure [6], hence pharmacological prevention of tachyarrhythmia is reasonable. Amiodarone is recommended for AF with heart failure or structural heart disease as it maintains sinus rhythm, thus may be appropriate for patients with uncorrected paroxysmal AF, WPW, and EA.
In a patient with pre-excited AF, the recommended therapy is the administration of IV procainamide or Ibutilide, cardioversion, and catheter ablation of the accessory pathway. IV amiodarone might be an alternative therapy for pre-excited AF, but a defibrillator should be readily available. In a patient with paroxysmal AF, WPW and Ebstein's anomaly, oral amiodarone to maintain sinus rhythm might be reasonable.
All the authors declare no conflict of interest.
There were no sources of support.
All authors made equal contribution.