To analyze the requirement of High Dependency Unit (HDU) and Intensive care Unit (ICU) in an obstetric population in terms of utilization rate, indications for admission, interventions required and gestational outcome.
Retrospective observational study was carried out from October 2016 to September 2017 in Kasturba Hospital, Mother and Child Health Wing, Mahatma Gandhi Institute of Medical Sciences Sewagram placed in rural central India. Data related to indications for HDU/ICU admission, interventions required, length of stay and outcomes were collected, and results were analyzed.
Our obstetric HDU utilization rate was 11.2 per 1000 deliveries. Out of total 57 subjects 48 had no prior antenatal care. Majority (68.42%) were admitted in HDU with only obstetric reasons, while 31.57% required HDU for pre-existing medical diseases. The major obstetric indications were septicemia (35.08%) & PPH (29.08%) and hypertension was observed in 21.05% of women. Other less common causes included post-surgical acute kidney injury, APH, chorioamnionitis and pyelonephritis. Half of the women with pre-existing medical disease had cardiovascular problems. Patients with medical diseases had more pre-term labor (10 vs. 5; P ≤ 0.05), respiratory failure (9 vs. 2; P ≤ 0.05), cardiac failure (7 vs. 1; P ≤ 0.05), duration of stay more than 10 days (15 vs. 6; P ≤ 0.05), fetal growth restriction (6 vs. 3; P ≤ 0.05) and prolonged recovery time. Maternal mortality among these critically ill women was 12.28% and fetal mortality was 17.54%.
Establishment of well managed high dependency and intensive care unit in health care facilities dealing with high volumes of high-risk maternity cases reduces the maternal mortality significantly and results in improved maternal outcomes.
High dependency unit, Obstetric critical care, Pregnancy complications, Intensive care unit
Confidential enquiry into maternal deaths have revealed that there are still a significant number of maternal deaths associated with suboptimal care [1]. "There is a story behind every maternal death and life-threatening complication" and understanding the lessons to be learnt can help to avoid such outcomes [2]. Any pregnant woman can develop life threatening complications with little or no advance warning. Though pregnancy and labor are considered a physiological process the potential for catastrophic complications is constant and may develop in a matter of minutes. The diagnoses precipitating admission to critical care are predictable and include massive haemorrhage (> 2,500 ml loss), eclampsia, sepsis, thromboembolism, acute organ dysfunction (renal, hepatic, cardiac, respiratory, neurological) and anaesthesia-related morbidities such as aspiration, anaphylaxis and muscle relaxant-related problems [1]. These women with obstetric complications need access to quality maternal health services that can detect and manage life threatening obstetric complications. They need round the clock personalized care by skilled providers, essentially led by Obstetricians or Emergency Obstetric Care (EmOC) trained providers. For those women who have progressed to an adverse clinical condition where there is multi-organ involvement/failure, the care has to be provided in an intensive care unit setting led by intensivist/super-specialists [3].
The proportion of obstetric patients requiring admission to intensive care units (ICUs) varies among published series at between 1-9 per 1000 deliveries, with obstetric complications accounting for the majority of admission diagnoses. The availability of a high dependency unit (HDU) within an obstetric setting has a number of potential advantages, including the concurrent availability of expert obstetric care and critical care management. It has been suggested that the presence of 'on-site' critical care facilities would reduce the need to transfer patients to a general medical/surgical ICU [4]. It has been observed that majority of maternal deaths recorded at the institution have multiple morbidities including obstetric disorders and medical disorders complicating pregnancy. These mothers require specialised intensive critical care and some require ventilatory support. The presence of a well-developed critical care unit (HDU/ICU) with appropriate infrastructure, equipment's and trained staff is the key for providing necessary and timely intensive management to these critical mothers. In Western India the incidence of mothers requiring intensive care unit is around 5.48 per 1000 deliveries [5]. In central rural India we retrospectively analyzed the demographic parameters, reason for admission and outcome of obstetric cases requiring admissions in HDU/ICU with an aim to review HDU/ICU setup in terms of HDU utilization rate, indications for admission, interventions needed and maternal outcome.
A hospital based, cross sectional, observational study was conducted in the Kasturba Hospital, placed in rural eastern Maharashtra in central India. Kasturba Hospital is attached to Mahatma Gandhi Institute of Medical Sciences, Sewagram, Wardha, a tertiary care referral centre serving underprivileged rural masses. MGIMS, Sewagram is an institution consistently being ranked among the top 20 medical schools in the country. The state has a maternal mortality ratio of 68 per one lakh live births (SRS 2011-13) and the health system is striving hard to provide quality maternity care and reduce maternal mortality further. MGIMS is a centre of excellence with a dedicated team of health care providers and hence most of the complicated maternal cases from the surrounding district's and even adjacent states of Andhra Pradesh and Madhya Pradesh are referred to this center. The referred cases at institution has further increased due to improved infrastructure in the form of newly constructed Maternal and Child Health Wing and availability of ICU facilities. Keeping the goal of providing a continuum of care with quality and with its endeavor to provide integrated, comprehensive reproductive, maternal, newborn, child and adolescent health in the region and showcase a model in the country, Government of India under the National Rural Health Mission and Government of Maharashtra sanctioned the state of art Model MCH wing at MGIMS, Sewagram which has become functional from October 2016. The Department of Obstetrics and Gynecology believes in providing quality services with a human touch to all the rural and urban women visiting the outdoor and indoor sections. The department has facilities for antenatal, postnatal, gynecological care as well as critical care unit with 9 bedded high dependency and 6 bedded intensive care unit.
Demographic information, relevant obstetric history, the reason for admission in HDU and ICU, need for ventilation, type of interventions and outcome of the pregnancy was obtained in a pretested, validated questionnaire. The data was collected through hospital information system, from October 2016 to September 2017 and information from October 2015-November 2016 was the control. The comparison was done between obstetric outcome prior to setup of HDU ICU and post. HDU was defined as an area in a hospital where patients can be cared more extensively than in a normal ward, but not to the point of intensive care, also known as the intermediate care unit. Patients in HDU may require ICU admission later (step up) or at the same time, patients in ICU who had an improvement in their condition, may be shifted to HDU (step down), before shifting them to the general ward. Intensive care unit (ICU) was defined as specialised care unit dedicated to obstetric patients who have developed multi-organ failure necessitating specialized care by super-specialists like intensivist/nephrologist/cardiologist, pulmonologist/endocrinologist, etc. or requiring ventilatory support (mechanical ventilation). The study team taking care of the women comprised of trained nurses, resident doctors, consultant obstetricians, anesthetist, Intensivist and physician.
Data was entered in a spread sheet (Excel) and analysis was done by using descriptive statistics using SPSS 17.0 version. Normal distribution of the data was examined by Kolmogorov-Smirnov test and reported as arithmetic means ± SD, non-normally distributed data as medians (quartiles) and categorical data as numbers and percentages. The proportions were compared by chi square test and a two-level P value < 0.05 was considered as significant.
During the period of study, there were 755 admissions in Obstetric HDU and ICU amounting to 9.89% of total 7631 obstetric admissions (Table 1). The average monthly admissions were 62 (Figure 1) with an average length of stay of 3 days and average bed occupancy was 92% (Figure 2). Out of these 755 women, 90 required admission in intensive care unit amounting to 1.17% of admissions. Most women; 717 (94.96%) were successfully discharged homeward and 14 expired (1.85%) (Figure 3). Maximum women were in the age group of 21-25 years (54%) (Figure 4). The commonest obstetric reason for admission in HDU was hypertensive disorders of pregnancy (28%) followed by obstetric hemorrhage (19%), severe anemia (17%) and sepsis (9%). Heart disease, sickle cell disease with crisis, jaundice, infections and other medical disorders like ARDS and renal dysfunction accounted for non-obstetric cause (Figure 5). Eighty-four (11.12%) women received ventilatory support (Figure 6), 72% of whom survived (Figure 7) and the average length of ventilatory support was 1-3 days (Figure 8). Length of ventilatory support dictated the maternal survival and more than 3 days of advanced respiratory support carried a significant risk of mortality (Figure 8). Maternal mortality was more often associated with non-obstetric causes (64.28%) compared to obstetric (35.71%). Significant improvement in outcome of patients was seen after the establishment of functioning HDU/ICU (Table 2) as evident from the reduction in maternal mortality from 5.72% (572/100,000 live births) to 1.85% (185 per 100,000 live births) with a statistically significant difference.
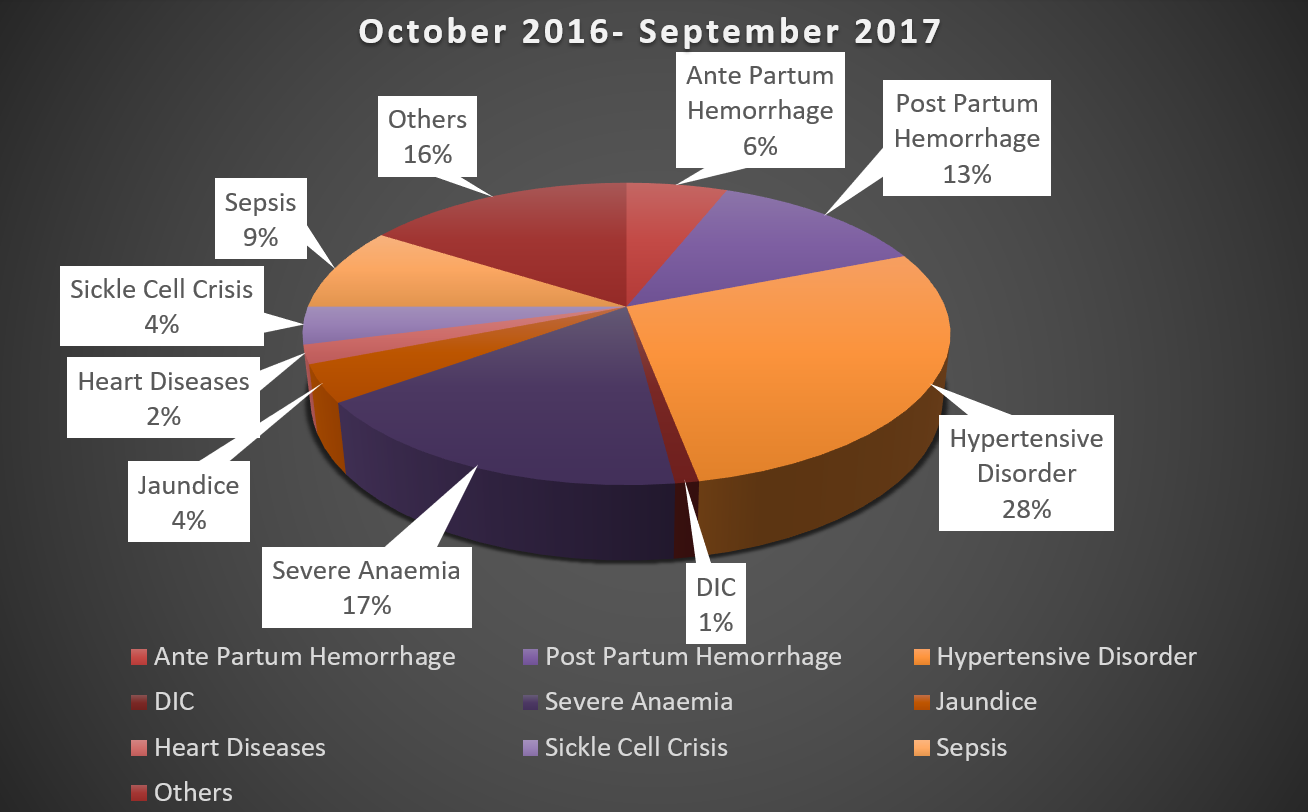 Figure 1: Indications for admission in obstetric HDU/ICU.
View Figure 1
Figure 1: Indications for admission in obstetric HDU/ICU.
View Figure 1
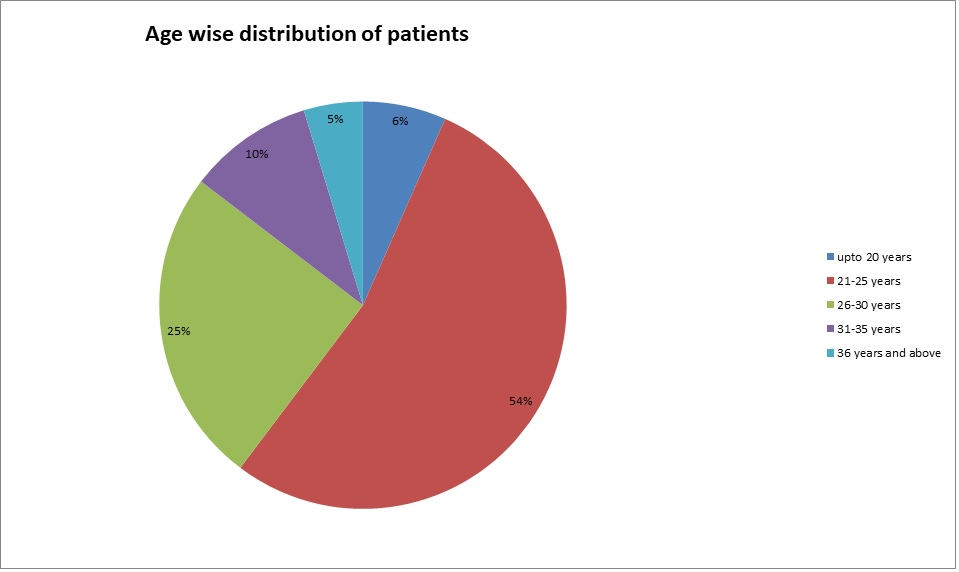 Figure 2: Age wise distribution of patients admitted in obstetric HDU/ICU.
View Figure 2
Figure 2: Age wise distribution of patients admitted in obstetric HDU/ICU.
View Figure 2
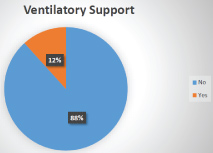 Figure 3: Percentage of women requiring ventilatory support.
View Figure 3
Figure 3: Percentage of women requiring ventilatory support.
View Figure 3
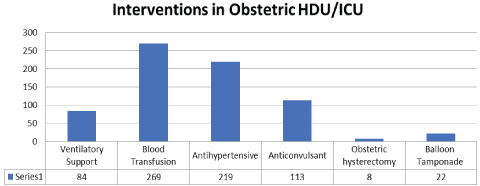 Figure 4: Interventions carried out on women admitted in obstetric HDU/ICU.
View Figure 4
Figure 4: Interventions carried out on women admitted in obstetric HDU/ICU.
View Figure 4
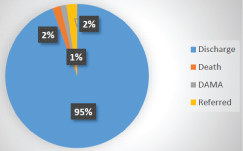 Figure 5: Outcome of women admitted in obstetric HDU/ICU (Oct 2016- September 2017).
View Figure 5
Figure 5: Outcome of women admitted in obstetric HDU/ICU (Oct 2016- September 2017).
View Figure 5
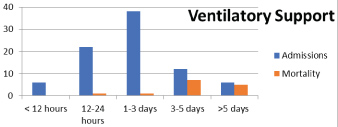 Figure 6: Average length of ventilatory support.
View Figure 6
Figure 6: Average length of ventilatory support.
View Figure 6
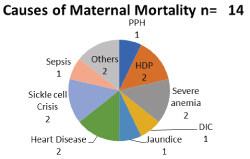 Figure 7: Causes of maternal mortality.
View Figure 7
Figure 7: Causes of maternal mortality.
View Figure 7
 Figure 8: Outcome of women on ventilatory support.
View Figure 8
Figure 8: Outcome of women on ventilatory support.
View Figure 8
Table 1: Performance of obstetric facility in MCH wing after setup of HDU/ICU, Sevagram (2016-17). View Table 1
Table 2: Performance of obstetric HDU/ICU and pregnancy outcome. View Table 2
Intensive care is appropriate for patients who require or are likely to require advanced respiratory support alone, for those requiring support for more than one organ system or for patients with chronic impairment of one or more systems sufficient to restrict daily activities (co-morbidity) and who require support for an acute reversible failure of another organ system. High dependency unit care on the other hand is appropriate for patients requiring support for a single organ system (excluding advanced respiratory support), those who can be benefited from more close observation and monitoring than can be safely provided in a general ward, patients no longer needing intensive care but cannot be returned to general ward and for post-operative patients who require more close and intense monitoring. It is a level of care which lies in between a general ward and an intensive care unit (ICU) [6] and typically patients who are at a high risk of developing life-threatening complications. High dependency care provides a level of intermediate care and can act as a "step-up" or "step-down" unit between the level of care delivered on a general ward and intensive care. An associated co-morbidity may convert a high dependency care to a need for intensive care [7].
Management of the critically ill obstetric woman at an ICU is a unique challenge to ICU physicians and obstetricians. Maternal and Child Wing of MGIMS, Sevagram is equipped with both a High Dependency Unit and an Intensive care unit. During the study period, there were 7631 obstetric admissions, 5363 mothers delivered, 755 (9.89%) patients required admission in HDU and 90 (1.17%) required care in intensive unit. Various studies have reported an admission rate of obstetric patients in intensive care as approximately 0.1-0.9% of deliveries [8-10]. In Western India the incidence of ICU utilization by obstetric patients was 5.4 per 1000 deliveries, for 5 years [5]. The utilization varies widely among developed nations too, from 1.3% in 10 years in Hong Kong [2], 2.4% over two years in Netherlands [11], 10.2% in 4 years in Ireland [4] and 26.7% in 23 years in UK [12]. Zeeman, et al. admitted 1.7% of deliveries to obstetric intermediate care unit in their 2-year audit period [13]. Unfortunately, sparse data regarding HDU utilisation and care from developing nations is available. Studies from India report a lower rate of admission [7,8]. An obstetric High Dependency Unit admission rate of 5% has been cited in a number of recent reports [12,14]. These variations might be due to differences in defining major morbidity criteria for ICU admission and non-availability of an alternative facility for intermediate care. There is excellent data regarding critical care utilisation (260/100,000), however, prevalence rates for women who require a higher level of monitoring or single organ support is more difficult to quantify and may be as high as 1,200/100,000 i.e. 20 times the numbers represented in the Intensive Care National Audit and Research Centre (ICNARC) report and nearer to that mentioned in the present study [1].
High acuity pregnancy related illnesses necessitating a level of cardiovascular and respiratory monitoring exceeding 'normal' practice in delivery units have been recorded in significant number of women with a range of diagnoses; from small post-partum haemorrhages (> 1,500 ml), to pre-eclampsia, uterine rupture and HELLP syndrome. The ICNARC report in 2007 found that, of the 418 pregnant women admitted to HDU, obstetric reason for admission was seen in 72% [1]. As in other reports [9,10,15], in the present study, pregnancy-related hypertension with its complications (28%) and major obstetric hemorrhage (18%) were the two of the three main primary diagnoses at the time of admission. Both are associated with increased risk of maternal morbidity and mortality. Another important cause being severe anaemia (19%). Among patients with obstetric hemorrhage, majority had postpartum as compared to antepartum hemorrhage (13% vs. 6%). In various studies the important obstetric causes for HDU admission quoted were PPH and hypertensive disorders [2,4,5,11,12]. However, Dattaray, et al. found that sepsis accounted for the majority (35.08%) of admissions, followed by PPH (29.82%) and severe hypertensive disorders of pregnancy (21.05%). Common causes of sepsis were massive obstetric hemorrhage, chorio-amnionitis, urinary tract infections, puerperal infections and sequelae of operative interventions including criminal abortions. PPH and hypertensive disorders were the next two common causes in their study [16]. In the present study, sepsis accounted for 9% of the cases. Home deliveries in rural India or at health centres with inadequate infrastructure, unsupervised deliveries, dogmatic traditional approaches during birth, failure to use uterotonics and underlying anemia continue for PPH amounting to almost 28% of maternal mortality in India. An audit of severe maternal morbidity in Dublin, with 13 systems and management-based definitions, showed a rate of 320/100,000 for massive obstetric haemorrhage, as defined by the requirement of greater than or equal to five units of blood transfusion, occurred in 125/100,000 deliveries in one large multicentre study [8]. It has been observed that anemia and poor nutrition contribute to the risk of hemodynamic compromise arising from blood loss during delivery and this increases the maternal morbidity. The present study reports 17% of critically ill women have severe anemia which further complicates the scenario. In women with hypertensive disorders of pregnancy requiring HDU care, lack of timely diagnosis and inappropriate management coupled with ignorance of life-threatening complications like HELLP and eclampsia were responsible for poorer outcome.
Among non-obstetric complications various medical disorders like rheumatic heart disease, infective hepatitis, sickle cell disease with crisis, acute respiratory distress syndrome, dengue, renal dysfunction, H1N1 etc. necessitated HDU admission. Similar observations were reported by other researchers [2,4,11], though sickle cell disease with crisis is observed to be more common in this particular region of central, rural India. Acute, intensive maternal disease related morbidities were significantly increased in the obstetric cases with prior medical illness, and these included cardiac failure, respiratory failure and prolonged hospital stay and increased recovery time. A total of 12% of patients required advanced respiratory support in the form of mechanical ventilation. Another study conducted in China reports it to be as high as 40% [2]. The most frequent indications were acute respiratory failure (21%) and hemodynamic failure (41%).
The mortality rate of 2% for obstetric ICU/HDU admissions in the present study is below the developed world median of 3.4% (range 0-18.4%) and the developing world median of 14.0% (range 0-40%) [17] which shows a dedicated team effort and advocates the establishment of well-functioning obstetric critical care units in developing countries like India. Other studies report maternal death rate in the ICU varying from 3.4-21% [18-21]. Inadequate knowledge about the illness, infrequent admission of obstetric patients and non-availability of critical care setup results in high mortality and morbidity. The death rate in the present study was high among patients admitted for non-obstetric (64.28%) as opposed to obstetric indications (35.71%) thus implying the need for concentrating on good antenatal care, prompt diagnosis of high risk conditions and appropriate management in skilled setups wherein more attention needs to be focused on life threatening obstetric conditions as these are the woman who can be saved. The mortality rate was found to be similar in the hypertension group (2.15%) as compared to the haemorrhage group (2.63%). Severe PPH necessitated surgical interventions (28%) like obstetric hysterectomy, however balloon Tamponade helped to save life in 22 of 103 post-partum hemorrhage patients (21.35%). Dattaray, et al. [16] also found that patients with medical disorders had more mortality in comparison to obstetric group (5/18 vs. 2/39; P ≤ 0.05). In contrast in another study there were no such differences [22].
High mortality rate quoted in various studies [18-21] could be due to late referral from the peripheral centers, lack of awareness about the disease severity by the community, delay in transportation, and delay in initiation of the treatment. Another study found high maternal age, absence of prenatal care, transfer to ICU > 24 hours after onset of acute problem and severity of illness at the time of admission as assessed by APACHE II score to be the factors responsible for maternal mortality [15]. Early detection and timely appropriate intervention might avoid or minimize the effects of such complications. Proved treatment strategies for obstetric hemorrhage and sepsis along with timely management of critically ill patients in the high-dependency unit may help decrease maternal mortality and morbidity as a high-dependency care unit fulfils the needs of at least half of the obstetric population who require higher acuity care and simultaneously save considerable expenditure. Emphasis on early detection of maternal problems and prompt referral to tertiary centers could minimize the prevalence of multiple organ failure and mortality in these women. Our findings highlight the need for establishing a high dependency unit in all such centres in order to avoid unnecessary admission to the intensive care unit and to ensure proper management. Again, since puerperal morbidity has now become a focal parameter for quality of maternal care, a continued psychosocial follow-up of these patients should ideally be implemented to ensure better quality of life. Constant vigilance, judicious judgment along with provision of adequate resources are still the major stepping stones on the road to maternal safety [16].
The focus of interest should shift to intermediate care due to inadequate supply of intensive care facilities as a tool of bridging the gap between the level of care and support available in general ward and intensive care unit. Some hospitals have developed intermediate care in the form of HDU, however the information regarding the use of such units delivering quality care is very limited.
Staff caring for patients in acute hospital settings should have competences in monitoring, measurement, interpretation and prompt response to the acutely ill patient appropriate to the level of care they are providing. Education and training should be provided to ensure staff have these competencies and they should be assessed to ensure they can demonstrate them [23]. Developing team work, assertiveness and inter-professional working relationships, monitoring outcomes at all levels and critical incident analysis is imperative for ongoing improved maternal outcomes. Implementing these competences will require an effective leadership with system-wide approach and rigorous change management. The principle in managing the acutely ill pregnant woman is optimal management of the condition, with a multidisciplinary team. The present study reinforces and strongly advocates establishment of dedicated obstetric HDU/ICU especially in developing countries like India, to deliver a continuum of skilled obstetric care which promptly and skillfully addresses acute complications, chronic disorders getting amplified during pregnancy and catastrophic events through pregnancy, childbirth and post-partum so as to reduce maternal morbidity and mortality significantly.
Hemorrhage and pregnancy-related hypertension with its complications are the two common indications for HDU/ICU admissions in this study. Other than these two common obstetric indications, medical disorders like heart disease, respiratory diseases and their complications, infections are prevalently seen in pregnant women with acute morbidity requiring ICU/HDU admissions. A dedicated obstetric HDU/ICU will go a long way in reducing maternal mortality as the response time from onset of acute severe illness to provision of high-quality critical care will be substantially reduced. A multidisciplinary team approach with trained staff for timely quality management is the crux for continuum of skilled obstetric and critical care in pregnant women. Hence, the need for a dedicated obstetric ICU/HDU or critical care unit should be considered in every large public hospital and tertiary health care facilities catering to high risk pregnant women.
The authors report no conflict of interest.
We acknowledge sincerely the support of faculty and postgraduates of Obstetrics, Medicine and Anesthesiology and administrators of Mahatma Gandhi institute of Medical Sciences, Sevagram, India and Kasturba Health Society. We also acknowledge the Ministry of Health and Family welfare for providing the Maternal and Child Health Wing a dedicated High Dependency Unit and Intensive Care Unit.
Non-Funded.
We declare that all authors have equally contributed in the article.