This paper studies the Impact of SAFE PT tool in the handover process between shifts in the Royal Hospital adult emergency department (ED) and its impact on clinical improvement, patient satisfaction and decrease in length of stay (LOS) of patients. The study provides an insight into the end user adaptability and their opinions.
A prospective observational method; prior and post implementation survey comprising a questionnaire used to study the effects of the implementation of the SAFE PT handover.
50 participants each were approached prior and post implementation of SAFE PT to fill descriptive questionnaires. The new SAFE PT tool was found to be clear and user friendly. It enhanced the handover process to a smooth one and was found to be systematic and highlighted the high acuity patients as well as red flags of each patient handed over. The bedside handover coupled with the prefilled written SAFE PT made it a safe process with increased patient satisfaction emphasized by the significant reduction in percentage of patient LOS in the ED.
The SAFE PT handover proved to be a successful method of clinical handover between shifts in the ED with an impact on patient safety and care; leading to an increased patient satisfaction. It also contributed hugely to the reduction in the percentage of LOS of patients in the ED within 4 hours period. The result of the implementation of the new tool makes the ED proud to have a safe patient (SAFE PT) culture which is user friendly and one which has an emphasis on smooth patient flow. A 'SAFE PT' is indeed a 'HAPPY PT'.
Clinical handover demands a structured format for its efficient execution. This is possible with a well-developed tool which assists in transforming relevant information of patients to be handed over between shifts in the ED [1]. The SAFE PT handover developed and discussed in our earlier study [2] depicts a standard structured format which is the key to an efficient handover system. The implementation of the SAFE PT handover and its impact on the ED is evaluated in this study.
The clinical handover between shifts in ED is a complex matrix of multiple variables based in a difficult and unpredictable environment [3]. It's of importance that time, place and format be invested towards a structured module for safe and smooth transition of patients between shifts. The aim of a high-quality handover is to have continuity of care in an efficient and smooth way so as not to hinder or delay the care of patients but quicken the process and eliminating errors [4].
The SAFE PT tool is a well-developed tool that identifies the patient and relevant details of management of the patient during the stay in the department. It was developed based on international guidelines [5,6]. It highlights red flags with regards to the patient that are to be addressed, thereby reducing errors. It provides the user with recommendations for further management of patient including pending investigations, imaging, consultations and disposition plan. An overview of the patient can be easily accessed by just glancing at the SAFE PT handover sheet; this ensures that information can be easily accessed in short period of time saving valuable time for both patient and physician.
In the ED, there are multiple variables to distract a handover system. These factors need to be considered in large EDs divided into separate areas depending on acuity of care with high patient flow. This makes the handover a daunting task where it needs to prioritize patients over different sections of the department. So, it's even more necessary to have a tool that gives the takeover team an overall view of the patients in the department with specific red flags to patients of concern, the management plan agreed by both teams initiated and to be continued, division of resources appropriate to the area and patient. The entire system being patient centric and ensuring no duplication of work with a definite continuity of care over shifts for increased patient satisfaction. The incoming team that takes over from the outgoing team needs a tool that is reliable and dependable so as to continue the work with no hitches or glitches making a deep impact on quality of care.
The SAFE PT tool was designed based on the above criteria and its implementation initiated with a study to feel the impact it had on the culture in the Royal adult ED and measured with the help of quality Indicators [7,8].
Royal Hospital adult ED is a tertiary care teaching hospital, with new attendances of around 50,000 to the ED alone and a total hospital capacity of 650 beds. There is a separate paediatric ED within the hospital. This study is based in the adult ED, which has a capacity for 14 patients in cubicles, and two waiting areas (one for male and one for female patients).
There is an eight bed observation ward. The resuscitation room is set up for critically ill or injured patients; the 'major treatment' area is for those with similar conditions but requiring less intensive observations; and the day ward/observation area is for patients requiring a prolonged period of observation or requiring additional investigations. The Adult ED has round-the-clock consultants or specialists who lead three daily rounds in the adult department at beginning of each shift 07:30, 15:00 and 22:30 hours respectively. Each shift is led by a specialist who is assigned the overall responsibility of the department. The department is supported by similar nursing staff. ED doctor's handover under the supervision of a consultant during working hours and this task is replicated by specialist during out of working hours. The consultant leads the ward rounds attended by junior doctors and the nursing in-charge. The Royal ED has a high load of patients sometimes reaching 200 and above in a day and performance standards in the Royal Hospital mandate workup and diagnosis of patients within 4 hours. The ED being the most volatile service unexpected developments are frequently encountered and it's left to the shift in-charge to fix them as and when the need arises. The handover practice that was being practiced was a verbal one between physicians on a one to one basis by the bedside of patients or on ad hoc basis when consultant requested for it. There was a lack of structured tool to transfer information between shifts. This demanded a humongous task of implementing an accurate handover system.
The study conducted over a period of 12 weeks involved 50 participants each prior and post implementation of the SAFE PT handover system. It looked into user friendliness, compliance to the new tool and the impact it had on patient safety and satisfaction.
Information was collected by survey questionnaires before and after the implementation of tool. The questionnaires assessed the type and format of the handover system and the impact the tool brought into the process. It also looked for incidents or hurdles that were asked to be mentioned and suggestions for improvement.
Compliance was measured by daily monitoring of the filed forms of the SAFE PT tool that had been used during the handover process and were evaluated if any incidents missed that had been reported by the nursing in-charge on the same day. Impact of the tool on physician and patient were studied. The takeover team was observed and questioned for the positive and negative effects they encountered from the new system. Impact on patient flow and satisfaction was measured by monitoring patient complaints or its effect on LOS of patient in the ED.
SAFE PT implementation is studied in detail in the earlier study2 and the survey performed post implementation of the handover studied over a period of 12 weeks. The handover process is now a common practice at the end of shift in Royal Hospital adult ED.
The pre and post implementation surveys of the SAFE PT tool involved questionnaires that were filled by middle grade and senior physicians and nurses.
The data collected from ED nurses related to preparedness of safe handover model and improvement in patient care was exported to SPSS version 20. CHI SQUARE test was applied to test to establish an association between improvement in patient care and preparedness for safe handover method.
H0: There is no association between department prepared for safe handover process and overall improvement in patient care OR
H0: Improvement in patient care is independent of department prepared for safe handover process. (H0 = Hypothesis 0).
H1: There is association between department prepared for safe handover process and overall improvement in patient care OR
H1: Improvement in patient care is dependent on department prepared for safe handover process. (H1 = Hypothesis 1).
From the Graph 1 it is evident that there is 74% improvement in patient care after implementation of safe handover model.
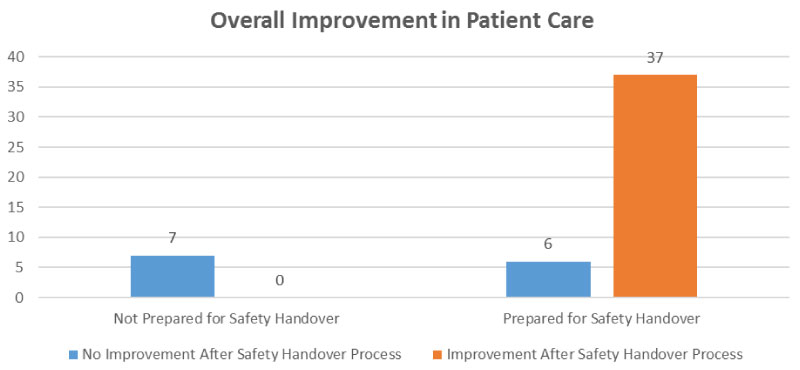 Graph 1: Safe handover process and overall improvement in patient care.
View Graph 1
Graph 1: Safe handover process and overall improvement in patient care.
View Graph 1
Applying chi square test to test for independence of improvement of patient care with respect to implementation of safe handover module. The output of chi-square test are given below.
From the top row of the last table, Pearson Chi-Square statistic, Chi-square = 23.166, and p < 0.001; i.e., a very small probability of the observed data under the null hypothesis of no association. The null hypothesis is rejected, since p < 0.05 (in fact p < 0.001). There is association between department prepared for safe handover process and overall improvement in patient care.
Data collected from ED physicians about pre and post preparedness of safe handover model was exported to SPSS version 20. Paired t test applied to test to find if there was significant difference in overall improvement in patient care with regard to pre and post implementation of safe handover model.
H0: There is no difference in mean improvement in patient care with regard to pre and post safe handover module.
H1: There is a difference in mean improvement in patient care with regard to pre and post safe handover module.
There is strong evidence (t = 3.05, p = 0.004) that there is improvement in patient care post implementation of safe handover model Graph 2. In this data set, it improved patient care on average, by 0.16. The null hypothesis is rejected, since p < 0.05 (in fact p = 0.004). Therefore, there is a difference in mean improvement in patient care post safe handover practice in positive way.
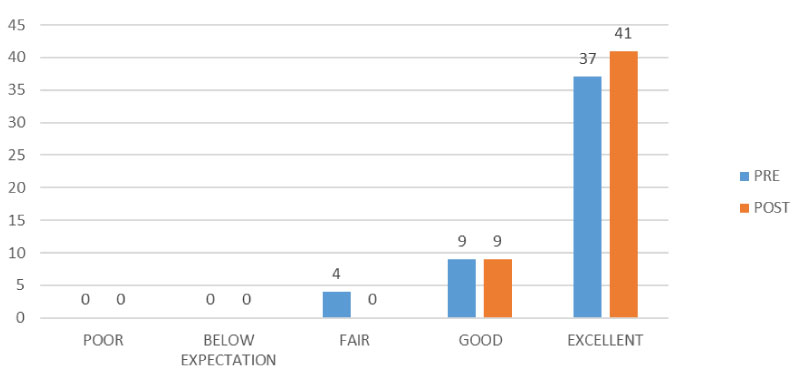 Graph 2: Mean improvement in patient care with regard to pre and post safe handover module.
View Graph 2
Graph 2: Mean improvement in patient care with regard to pre and post safe handover module.
View Graph 2
Data collected from ED physicians about pre and post preparedness of safe handover model are exported to SPSS version 20. Paired t test is applied to test whether there is significant difference in patient satisfaction with regard to pre and post implementation of safe handover module.
H0: There is no difference in mean satisfaction of patient with regard to pre and post safe handover module.
H1: There is a difference in mean satisfaction of patient with regard to pre and post safe handover module.
There is strong evidence (t = 4.41, p = 0.000) that there is improvement in patient satisfaction post implementation of safe handover model Graph 3. In this data set, it improved patient satisfaction on average, by 0.32. The null hypothesis is rejected, since p < 0.05 (in fact p = 0.000). Therefore, there is a difference in mean satisfaction of patient post safe handover practice in positive way.
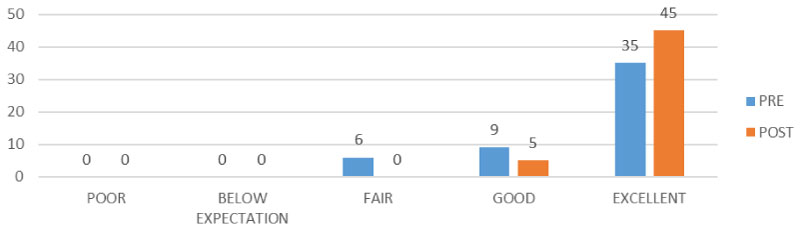 Graph 3: Mean satisfaction of patient with regard to pre and post safe handover module.
View Graph 3
Graph 3: Mean satisfaction of patient with regard to pre and post safe handover module.
View Graph 3
The observations that were obtained by participants who were involved in the implementation of SAFE PT handovers were studied and their results were compared to those prior to the implementation as depicted in the Chart 1.
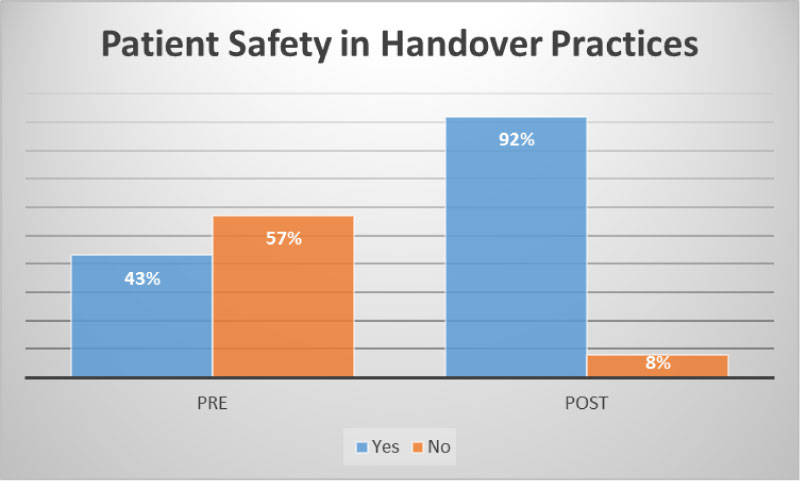 Chart 1: Patient safety in handover.
View Chart 1
Chart 1: Patient safety in handover.
View Chart 1
Participants commented that they felt patient safety had improved post implementation of the SAFE PT handover. The Chart 1 shows the marked improvement that was felt by the teams after the implementation of handover system.
The SAFE PT handover gained popularity amongst staff as it was easy to use in short span of time and this was expressed by majority of the participants in Figure 1.
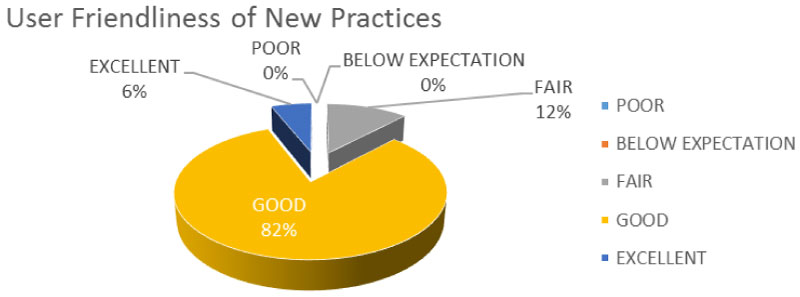 Figure 1: User friendliness of SAFE PT tool.
View Figure 1
Figure 1: User friendliness of SAFE PT tool.
View Figure 1
A good handover tool is one which has an overview of patients in the department with the resources and environment taken into consideration. This was compared in the survey prior and post implementation of data based on 4 criteria as listed in Chart 2.
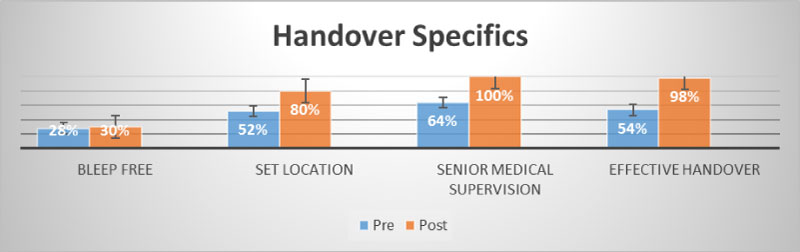 Chart 2: Handover specifics.
View Chart 2
Chart 2: Handover specifics.
View Chart 2
Participants believed the handover system was not bleep free and this was due to continuous inflow of new patients arriving to the ED. To overcome this problem an exclusive overlapping shift was introduced to manage new arrivals. There was an effective handover with good senior medical supervision in a defined location with the aid of the SAFE PT tool in a standardized method. Senior medical supervision brought additional positive improvement in management of patients. They were able to guide teams to overcome hurdles and enhanced the safety of patients Chart 3.
 Chart 3: Handover supervision.
View Chart 3
Chart 3: Handover supervision.
View Chart 3
Every shift had a senior physician to lead the handover and thus giving it authenticity as well as team approach in the management of patients. It also ensured compliance to the new system bringing out the benefits of having a second opinion in management of difficult cases and reducing errors in diagnosis of patients Chart 4.
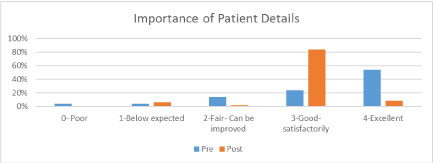 Chart 4: Importance of patient details in handover.
View Chart 4
Chart 4: Importance of patient details in handover.
View Chart 4
The new implemented handover system was found to provide relevant patient details which was appreciated by participants and considered important in transfer of data. These details were case specific and thus provide a higher quality of care Chart 5.
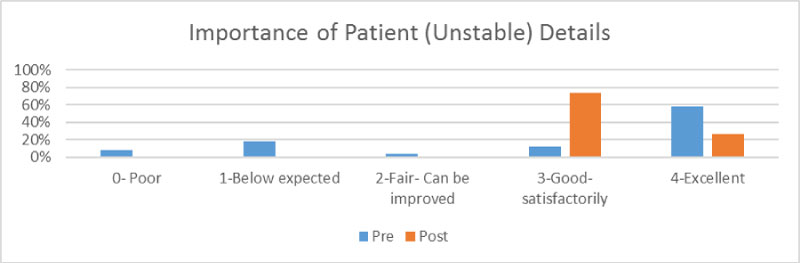 Chart 5: Importance of details of unstable patients.
View Chart 5
Chart 5: Importance of details of unstable patients.
View Chart 5
Prior to implementation of SAFE PT tool it was found that there was not much importance given in handing over unstable patient details. Participants acknowledged that it was good to have details of unstable patients highlighted in the new system as these patients demanded immediate attention and resources could be allocated at the earliest. This ensured that there was no delay in treatment of high risk and life threatening conditions.
The quality team of the ED monitors the different performance indicators of the ED on a quarterly basis to the quality management department of Royal Hospital. It was reported that there was a significant change in the KPIs of the adult ED during the period of implementation of the SAFE PT handover system and the results were as shown in the Figure 2.
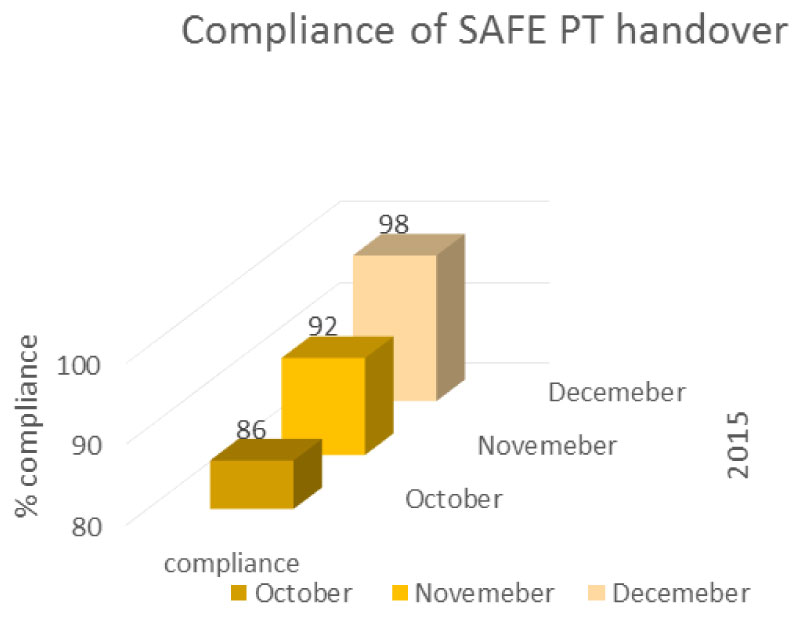 Figure 2: Compliance to SAFE PT handover tool; KPI [9] adult ED.
View Figure 2
Figure 2: Compliance to SAFE PT handover tool; KPI [9] adult ED.
View Figure 2
The SAFE PT tool was monitored for its compliance and had a near complete compliance rate at the end of 12 weeks period from its initiation showing its acceptability amongst the staff and their increased dependence on it. It also established that the Royal ED staff relied on the SAFE PT handover tool for transfer of data between shifts to ensure patient safety. The SAFE PT handover was found to have an Impact on patient care and satisfaction Chart 6.
 Chart 6: Patient care.
View Chart 6
Chart 6: Patient care.
View Chart 6
Participants noticed a definite improvement in the quality of care provided by the department and it showed a direct impact on patient satisfaction. This was also reflected in the patient satisfaction survey conducted by the quality team of the ED as shown in Figure 3.
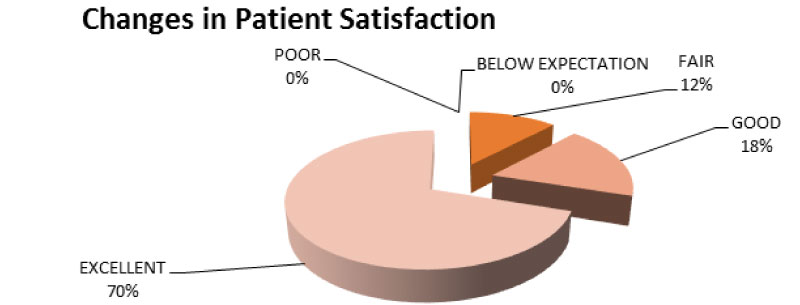 Figure 3: Patient satisfaction; KPI [9] adult ED.
View Figure 3
Figure 3: Patient satisfaction; KPI [9] adult ED.
View Figure 3
Implementation of the SAFE PT tool efficiency was found to have an impact in the Key Performance Indicators of the ED [9] There was a decrease in the percentage of patients staying over 4 hours in the ED as indicated in Figure 4.
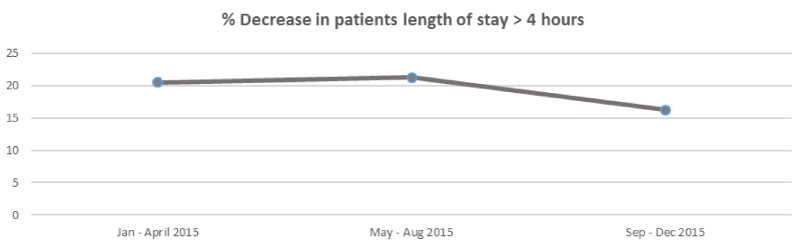 Figure 4: Quarterly % decrease in LOS in 2015 in adult ED; KPI [9] adult ED.
View Figure 4
Figure 4: Quarterly % decrease in LOS in 2015 in adult ED; KPI [9] adult ED.
View Figure 4
There was an indirect effect noted post implementation of the SAFE PT tool as noted in the departmental KPI of Return of patients to ED within 24 hours which invariably translated to the fact that there was a decrease in errors and morbidity rate of patients in ED as illustrated in Figure 5.
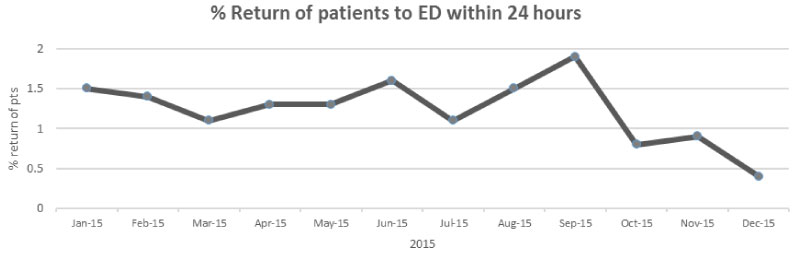 Figure 5: KPI [9] adult ED.
View Figure 5
Figure 5: KPI [9] adult ED.
View Figure 5
This study was based on observations of stake holders directly involved in the implementation of the SAFE PT tool. The possibility of Hawthorne effect as a limitation here cannot be ignored. Also, there was no observational analysis on the accuracy of handover performed. The compliance was based on forms filled and filed but there was no audio-visual aid of the actual process of handover being monitored which looked at performance for any gaps in transferring data. The study was limited to the Adult ED of Royal Hospital and was not compared to the handover process in the Paediatric ED and to other hospitals in the Muscat region.
The study would have benefited if the period was extended to 6 months with inclusion of markers to identify accuracy of information transferred between handovers and involved a larger sample study to authenticate its influence on patient care. There was limitation in unavailability of data measuring adverse events. A further period of study is recommended to see if there was an impact on decrease in adverse events post implementation.
The SAFE PT handover was a turning point to the culture of patient safety in Royal Hospital ED. Its impact was noted in improvements in the key performance indicators of the department that monitor quality and patient safety in their mandate. The mnemonic was a constant reminder to all staff that the patient safety was ingrained deeply into the system. It was an easy way to remember the structured format ensuring no vital information was missed during handover. Royal Hospital ED believed in a safe patient culture and emphasized it through the SAFE PT handover. It set an example to other departments to follow suit. Its user friendliness made it popular amongst the staff. The enormous gain that couldn't be ignored was the smile on patient's faces when their time spent in the ED was shortened and bore fruit. Patient Satisfaction was improved with the implementation of the SAFE PT handover.
The authors would like to thank all the staff at the emergency department at Royal Hospital facilitating this research, and extend special thanks to Dr. Sheeba Jabir, Dr. Spateeka Prakash for their assistance in the "'SAFE PT' handover, and to Professor Kevin Mackway-jones (Manchester Metropolitan University) for his support and expertise advice.
The author has not received any funding or benefits from industry or elsewhere to conduct this study.
Not commissioned; externally peer reviewed.
Authors confirm compliance with animal/human ethics guidelines. The ethical clearance for the study was approved by the Medical Ethics and Scientific Research Committee at the Royal Hospital with an approval number MESRC 48/2006.