Metformin associated lactic acidosis is a severe and potentially fatal condition. We here report a severe metformin-associated lactic acidosis in acute kidney injury caused by bilateral obstructing ureteral stones as an extremely rare combination of pathologies. Early treatment with bicarbonate infusion and subsequent acute haemodialysis was provided. As a result, respiratory failure and mechanical ventilation was prevented and the patient was discharged several days after the event. The patient gave written consent for publication of this case report.
A 72-year-old man presented to the emergency department complaining of lower abdominal pain. A week before presentation he developed malaise with lower abdominal pain. His urinary output was diminished and no urine output occurred during the last 18 hours. He had not experienced haematuria. He had dyspnea with mild exertion. There was no fever or chills present. The patient had well-formed stools without blood. The patient's medical history consisted of diabetes mellitus type II, hypertension, coronary artery bypass grafting plus aortic valve replacement and kidney stones requiring lithotripsy and percutaneous nephrolithotomy 10 years previously. His medications included: metformin, acetylsalicylic acid, metoprolol and simvastatin.
On general examination, the patient was somnolent and had Kussmaul's breathing pattern. He was hypothermic (35.5 ℃), tachypneic (40 breaths/min), hypertensive (214/108 mmHg), tachycardic (104 beats/min) and had an oxygen saturation of 97% at room air. Breath sounds were bilaterally clear on auscultation. The abdomen was soft, with normal bowel sounds and diffuse tenderness, without guarding, rebound tenderness or masses. Also, there was no costovertebral tenderness. The remainder of the physical examination was normal.
An urethral catheter was inserted, which did not lead to urine production. The initial laboratory tests revealed mild anaemia (8.0 mmol/L), white blood count of 16.6 × 109/L and a raised CRP (94 mg/L). Furthermore, he had a sodium level of 142 mmol/L, potassium level was 6.1 mmol/L, chloride 109 mmol/L, increased blood urea nitrogen level (42.1 mmol/L), increased phosphorus level (2.37 mmol/L) and markedly increased creatinine level (1,506 umol/L). His arterial blood gas revealed severe metabolic acidosis which was partially respiratory compensated (pH of 6.95, PaCO2 of 1.7 kPa, PaO2 of 22.1 kPa and HCO3- of 2.8 mmol/L). Glucose was 6.0 mmol/L, lactate 8.7 mmol/L and the anion gap was 30 mEq/L.
Given the patient's history of nephrolithiasis and identification of anuria accompanied with acute kidney injury, a postrenal obstruction was identified as the most probable cause of acute kidney injury. A computer tomography scan (CT) of the abdomen without contrast was performed. This revealed evidence for bilateral hydronephrosis due to bilateral obstructing ureteric stones (Figure 1). Besides the metabolic acidosis due to acute kidney injury, there was a severe lactic acidosis (up to 17 mmol/L). This was the result of metformin-associated lactic acidosis due to metformin use during acute renal impairment.
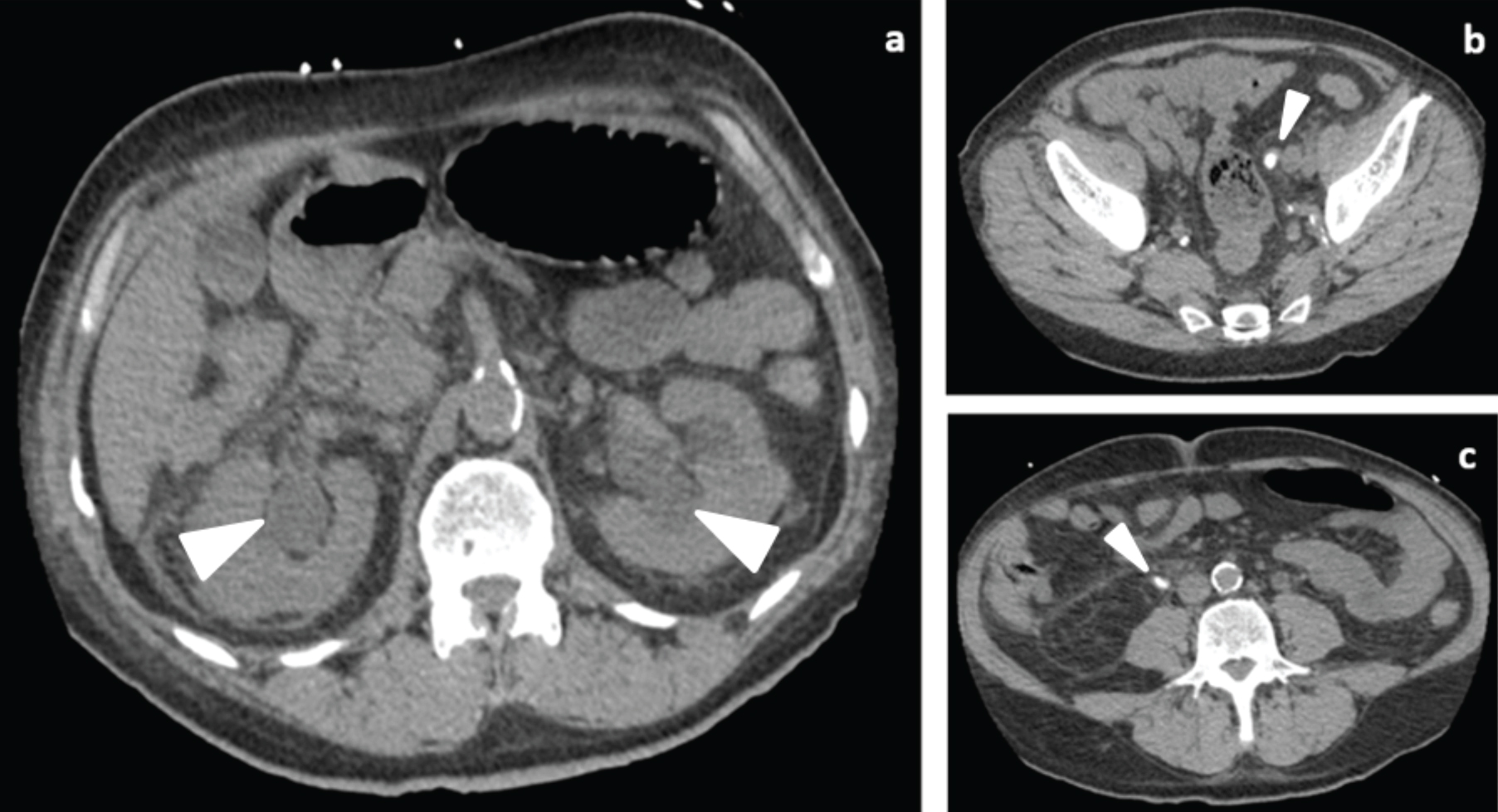 Figure 1: Abdominal CT without contrast. (a) Abdominal CT without contrast, axial image, showing bilateral hydronephrosis (marker); (b) Abdominal CT without contrast, axial image, left ureteral stone (marker); (c) Abdominal CT without contrast, axial image, right ureteral stone (marker).
View Figure 1
Figure 1: Abdominal CT without contrast. (a) Abdominal CT without contrast, axial image, showing bilateral hydronephrosis (marker); (b) Abdominal CT without contrast, axial image, left ureteral stone (marker); (c) Abdominal CT without contrast, axial image, right ureteral stone (marker).
View Figure 1
The patient was at risk of respiratory failure because of the need for respiratory compensation of metabolic acidosis. Based on the severe metabolic acidosis and possible onset of uremic encephalopathy, which were deemed to pose the highest immediate risk, acute haemodialysis was initiated. However, because of the severe respiratory distress a decision was made to first stabilize the patient with bicarbonate infusion to reduce the intensity of the work of breathing. The patient responded well to the initial treatment causing a decrease of the respiratory rate. He was subsequently admitted to the ICU for placement of a dialysis catheter and start of urgent haemodialysis. After 3 hours of haemodialysis with our refractory metabolic acidosis protocol, the acid base balance improved, the breathing pattern and the mental state normalized.
Subsequently, bilateral nephrostomy catheters were inserted for urinary tract decompression and preservation of the renal function. Thereafter continuous venovenous haemofiltration was necessary to achieve further normalization of the metabolic disturbances. Based on improvement of metabolic abnormalities the continuous venovenous haemofiltration was discontinued. The serum creatinine level gradually decreased to 211 umol/L at discharge after five days in hospital. The ureteric stones were eventually removed by ureteroscopy in an outpatient setting.
The incidence of acute kidney injury due to postrenal obstruction is low (< 10%) [1]. This low incidence of post renal acute kidney injury is explained because a single functioning kidney can maintain near-normal excretory function and acid-base balance. Post renal acute kidney injury develops almost exclusively in ureter obstruction with a single functioning kidney or in bilateral renal or lower urinary tract obstruction, which mostly occurs by prostatic disease in men [2]. The yearly incidence of nephrolithiasis is approximately 0.5% in North America and Europe. The lifetime risk of kidney stones is about 10-15% in the Western civilization. There is a high risk of recurrence of around 50% in 5-10 years [3]. Patients with nephrolithiasis present with an acute onset of colicky pain, typically radiating from the flank to the groin, costovertebral tenderness, urinary tract infection, blockage of the urine flow, and occasionally haematuria (in 30% of patients). The pain is usually episodic, lasts for 20 to 60 minutes and does not completely resolve before the next episode of pain. The pain is often accompanied by nausea and vomiting [4,5].
When nephrolithiasis is clinically suspected, confirming imaging should be performed. Ultrasound (US) can identify stones located in the kidney and pyeloureteral and vesicoureteric junction, but may fail to detect urethral calculi. For ureteric calculi, the sensitivity and specificity of US for detection is respectively 45% and 94% [6]. Conversely, a non-contrast-enhanced low-dose CT has a sensitivity and specificity of respectively 96.6% and 94.9% for the detection of urolithiasis [7]. For this reason, CT of the abdomen and pelvis without contrast is considered the gold standard imaging technique to confirm or exclude the diagnosis of ureteric stones in the acute setting. In addition, CT offers the possibility to detect or exclude other intra-abdominal pathology [8].
There are two options for urgent decompression: either retrograde placement of an ureteral stent via ureteroscopy or percutaneous placement of a nephrostomy catheter. Currently there is little evidence in favour of one over the other [9]. Frequently post-obstructive polyuria occurs after resolution of the obstruction. Therefore, careful fluid monitoring and replenishment is essential to prevent volume depletion, which can lead to subsequent prerenal kidney injury [10].
Due to the bilateral outflow obstruction the patient developed acute kidney injury and severe metabolic dysfunction. The acidosis was further exacerbated as a result of the subsequent development of MALA, due to metformin accumulation. MALA is an extremely rare disease (0.03 to 0.06 per 1000 patient-year) and is associated with mortality rates of 30-50%. MALA refers to a blood lactate concentration greater than 5 mmol/L and arterial pH less than 7.35 in combination with metformin use [11]. The mechanism of MALA is inhibition of mitochondrial respiration in tissues (i.e. liver and muscle), which leads to a rise in lactate. Furthermore, metformin impairs gluconeogenesis from lactate, pyruvate and alanine [12].
Supportive care and resuscitation are the primary management of MALA. There is no antidote available for metformin toxicity. Bicarbonate can be used to correct the acidemia. However, this is in some ways controversial. It may exacerbate intracellular acidosis, leftward shift of the haemoglobin dissociation curve, excessive sodium administration and may lead to numerous electrolyte abnormalities. Due to the high mortality associated with MALA it is important to consider extracorporeal treatment (ECTR), such as haemodialysis and haemofiltration, in the early phase of care [11].
Although there are no randomised clinical trials among patients with severe metformin poisoning that addressed this, the use of ECTR is supported on the basis of retrospective series and case reports. ECTR in metformin toxicity leads to removal of metformin and contributes to the correction of the hyperlactatemia. In addition, ECTR provides a faster, more predictable method to correct the acidosis compared to bicarbonate infusion, and rapid correction of electrolyte abnormalities. ECTR is recommended if the lactate concentration is greater than 20 mmol/L, pH less than or equal to 7.0 and standard therapy (supportive care and bicarbonate infusion) fails. It can be considered if the lactate concentration is greater than 15 mmol/L and pH less than 7.1. The threshold for initiating renal replacement therapy is lowered when comorbidities are present. These comorbidities include shock, impaired kidney function, liver failure or decreased level of consciousness. Intermittent haemodialysis with bicarbonate buffer is considered the preferred initial renal replacement therapy. This technique is superior, compared to other dialysis techniques, for correcting acidemia and removing metformin and lactic acid. In addition, haemodialysis is a technique that is worldwide available and relatively inexpensive. If metabolic abnormalities relapse after initial session, either intermittent haemodialysis or continuous renal replacement therapy is acceptable. Renal replacement therapy can be discontinued when the lactate concentration is lower than 3 mmol/L and pH greater than 7.35 [11].
Metformin-associated lactic acidosis in acute kidney injury caused by bilateral obstructing ureteral stones is an extremely rare combination of pathologies, which are potentially life-threatening diseases. In this case, CT of the abdomen quickly revealed the cause of the increased creatine level, severe metabolic acidosis and possible onset of uremic encephalopathy. Urgent treatment with bicarbonate infusion and subsequent acute haemodialysis were essential to prevent respiratory failure and mechanical ventilation. Subsequently, urinary tract decompression was performed to preserve the renal function.
R.P.J. Boxma: Writing - Original Draft.
M.G. Vervloet: Writing - Review & Editing.
J.J. Haitsma: Writing - Review & Editing and Supervision.
Assistance with the case report: None.
Financial support and sponsorship: None.
Conflicts of interest: None.
Patient consent: Obtained.