A Traumatic brain injury (TBI) is caused by sudden exchange of mechanical energy that causes cranial injury. It is a condition with high morbidity and mortality. A substantial number of survivors suffer disabling injuries. Management is aimed at avoiding secondary brain injury, thus improving the prognosis and reducing mortality. In the General Zone Hospital 50 of the Mexican Social Security Institute in San Luis Potosí, TBI is a frequent cause of visit in the emergency service; it represents 1.6% of all consultations. The present study aims to establish the correlation of the Glasgow coma scale score (GCS) and tomographic findings with in-hospital mortality, which would allow timely decisions to be taken. Finding a correlation would help us to suspect the severity of the injury that could be found in the imaging study before obtaining it, helping at the same time to make decisions about the diagnosis and initial management of our patient, avoiding an increase in the secondary injury, improving the prognosis, and shortening the hospital stay.
It’s a prospective, observational study, in which a sample size was calculated for finite populations of 124 patients. With the data collected from the capture sheets in Excel, the statistical analysis was performed with the SPSS 20.0 program, analyzing the qualitative variables using Fisher's test, the quantitative variables are expressed in measures of central tendency and they were analyzed using chi square.
108 survivors and 16 deaths were documented. Within the group of surviving cases, two patients presented a GCS of 3 point, of which one had Marshall of IV and the other with multiple lesions; 6 cases with 7-points of GCS, of which presented Marshall II, III, IV, Greene 2, 4b and one case with mixed lesions. As well 78 cases with 13 points GCS, documenting 29 cases with Marshall I, 10 with Marshall II, 2 with Marshall III, 21 with Marshall IV, 6 with Greene 1, 5 with Greene 2 and 5 with mixed lesions. While in the group of cases that died, there were 4 cases with 3 of Glasgow, 2 with Marshall IV and 2 with mixed lesions; 1 patient with Glasgow of 13 points with Marshall IV. With the aforementioned, a relationship was found between GSC, CT findings with mortality in the group of patients who survive.
High mortality was demonstrated in patients with tomographic findings with severe lesions, and its relationship with GCS, therefore, in an initial evaluation in the emergency department with a low score, neuroprotective actions should be intensified even before having the computed tomography, which could make the difference between life and in-hospital death.
Traumatic brain injury, Glasgow coma scale score, Computed Tomography, Mortality
TBI: Traumatic Brain Injury; IMSS: Mexican Social Security Institute; HGZ 50: General Zone Hospital 50; SLP: San Luis Potosi; GCS: Glasgow Coma Scale Score; SAH: Subarachnoid Hemorrhage; ATP: Adenosine Triphosphate; ICP: Intracranial Pressure; CSF: Cerebrospinal fluid; GCS: Glasgow Coma Score; CT: Computed Tomography; DML: Deviation from the Midline, IME: Injury with Mass Effect
A Traumatic brain injury occurs when a sudden trauma, often a blow or jolt to the head, causes damage to the brain. The severity can vary from mild to severe, it is a condition with a high morbidity and mortality worldwide, affecting 10 million people [1]. A considerable number of survivors suffer from disabling injuries. Management is aimed at avoiding secondary brain injury, thus improving the prognosis, reducing mortality and hospital stay (Table 1) [2-6].
Table 1: Traumatic brain injury definition. View Table 1
The General Zone Hospital 50 (HGZ 50) of the Mexican Social Security Institute (IMSS) in San Luis Potosi (SLP) is the only hospital in the capital that has a neurosurgery service, which makes TBI a frequent cause of visit in the Emergency service. In 2017, HGZ 50 reported 181 patients diagnosed with TBI, which represents 1.6% of all consultations. Finding to be more frequent in men aged between 25 to 34 years. Figure 1 shows the distribution of the TBI in the HGZ 50 during 2017.
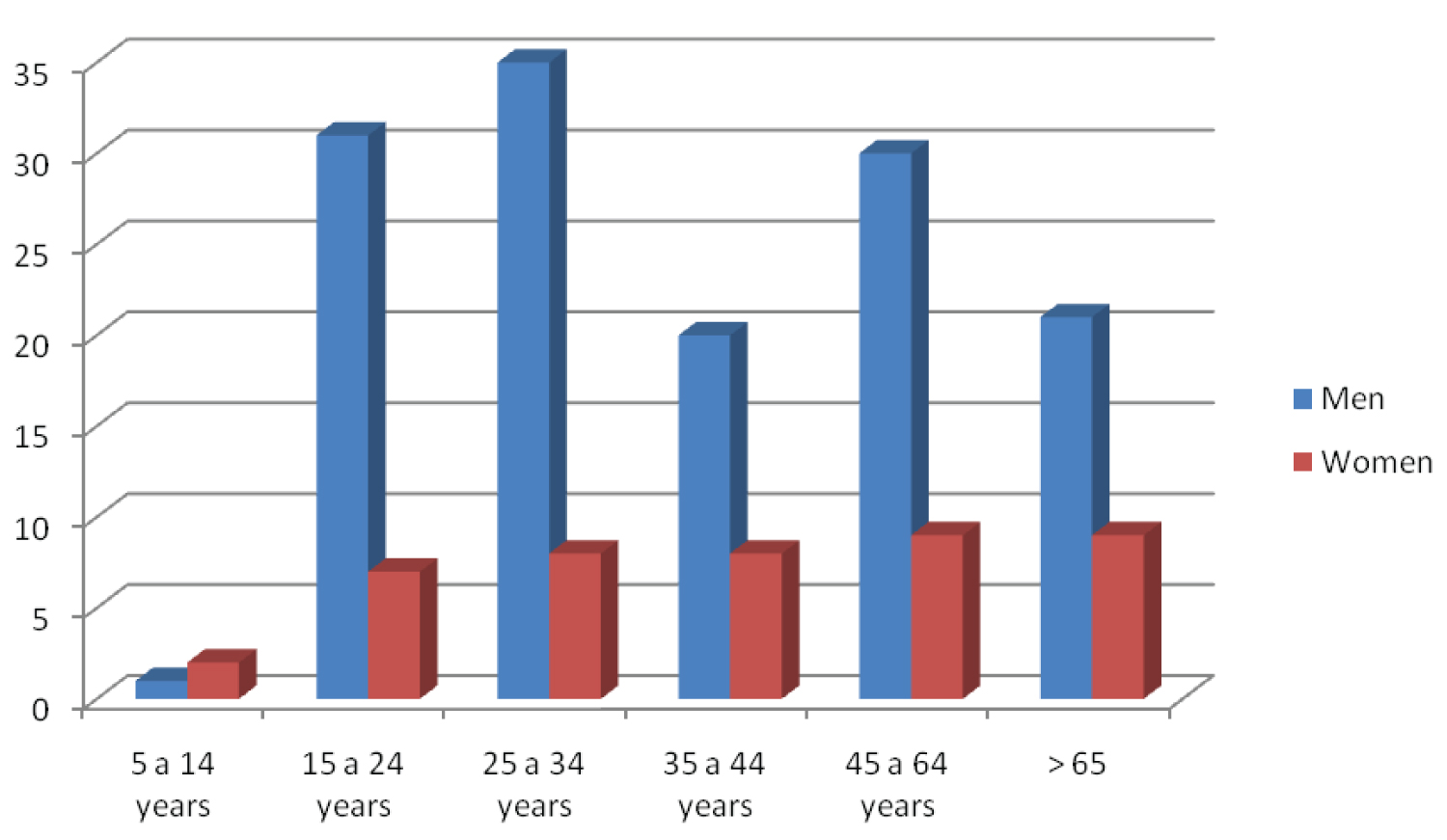 Figure 1: Traumatic Brain Injury: HGZ 50. 2017.
View Figure 1
Figure 1: Traumatic Brain Injury: HGZ 50. 2017.
View Figure 1
An epidemiological survey reports that 85% are classified as mild to moderate, while 5% as severe [1]. Others report that 80% are classified as mild, 10% are moderate, and 10% are severe [7]. The incidence varies from 47.3 to 849 cases per 100,000 inhabitants per year [8].
Trauma is a major cause of death in the population aged between 1 to 45-years-old, TBI responds to the majority of these deaths with more than 50,000 deaths in the United States [9].
In our country it is the fourth cause of death, reporting a mortality of 38.8 per 100,000 inhabitants. It is more frequent in men, affecting mainly the ages between 15 and 45 years. Mainly due to car accidents in 75%, observed in motorcyclists, under 25 years of age, and the use of alcohol as risk factors [2].
Have knowledge the pathophysiology of TBI is of great importance to establish an adequate treatment [10]. We can find two stages, classified as primary injury and secondary injury. The primary injury is distinguished by a direct impact, either the presence of hemorrhage (punctate or subarachnoid) or by contusion. The second phase is distinguished by subsequent hemorrhage, edema, and hypoxia of brain tissue. During the primary injury, changes are generated in brain metabolism, which alter hemodynamics and homeostasis, so energy production is altered depending on anaerobic glycolysis, leading to a decrease in ATP. This affects ion transport across the membrane [6].
The secondary injury develops during hours and days after the initial impact. Elevated intracranial pressure (ICP) and decreased cerebral perfusion pressure may be the result of brain swelling, extra-axial focal lesions, or global mechanisms that occur at the cellular level that lead to cerebral edema. Excess excitatory amino acids, such as glutamate and aspartate, are seen in extracellular fluid and cerebrospinal fluid (CSF). This contributes to cytotoxic injury, which ultimately leads to acute neuronal and astrocytic inflammation, cell damage, or cell death through cell necrosis and apoptosis [7].
The Monro-Kellie law mentions that intracranial volume is made up of brain tissue, cerebrospinal fluid, and blood. When one compartment increases, there is compensatory decrease in another compartment to prevent intracranial hypertension [9]. Of the intracranial components, only blood volume can be rapidly altered as a compensatory response. Normally the blood flow is 50 ml/100 g/min, with a volume of 100 ml, which corresponds to 5 to 10% of the intracranial components [10]. The decrease in cerebral blood flow produces ischemia, hypoxia, increasing brain injury [9].
The energy required by the brain is obtained by the oxidative metabolism of glucose. About 50% is used in ion flux across the cell membrane. In the case of ischemia, oxygen shortages, oxidative phosphorylation and energy production are altered. It passes to the anaerobic route, generating cascade processes, causing degradation of the components of the cell. This in turn favors secondary injuries [10].
Central mechanisms of dysregulation after brain injury may contribute to the development and progression of extracerebral organ dysfunction by promoting systemic inflammation that has the potential for medical complications [11,12].
Hematological examinations are required for the approach. The decrease in hematocrit is related to bleeding. Hyponatremia data can tell us about inadequate antidiuretic hormone secretion, diabetes insipidus [13]. ICP monitoring remains a recommendation [14].
The Glasgow Coma Scale (GCS) is of great importance for the clinical classification of severity. The following table shows the parameters that are evaluated [15-19] (Table 2).
Table 2: Glasgow Coma Scale. View Table 2
We can use imaging studies as a tool to classify our patients with a TBI diagnosis. One of the scales is the Green Tomographic Scale as it appears in Table 3.
Table 3: Greene tomographic scale. View Table 3
On the other hand, we can use Marshall scale to stage the condition of our patients, as shown in Table 4.
Table 4: Marshall scale. View Table 4
Finding correlation between the Glasgow coma scale and the tomographic findings would help us make early decisions on the management of our patients. The level of consciousness would provide us with a suspicion of the degree of brain injury, and the prognosis as well as the probable outcome of the patient, having to act in a timely manner to limit secondary damage and improve the prognosis.
This is an observational, descriptive study, which took place in the HGZ 50 of the IMSS in San Luis Potosi with patients who arrive at the Emergency service with a diagnosis of moderate TBI- severe, over 15 years of age, Glasgow between 3 to 13 points, with no history of alcohol intake, from January 2019 to December 2020. A sample size was calculated for finite populations of 124 patients. With the data collected from the capture sheets in Excel, the statistical analysis was performed with the SPSS 20.0 program, analyzing the qualitative variables using Fisher's test, the quantitative variables are expressed in measures of central tendency and they were analyzed using chi square. For the correlation of the variables, the Pearson test will be used.
Neurological status was analyzed with the Glasgow coma scale and CT scans were taken, which is indicated as a diagnostic protocol study in all patients with TBI moderate to severe admitted in the Emergency room. The tomography was performed on the Toshiba Aquilion 16-slice tomograph.
The sample size was calculated using the formula for linear correlation significance for two variables, taking into account that TBI can lead to different types of injuries, a group with subarachnoid hemorrhage will be considered (evaluating the tomography with the Greene scale) and the rest of the lesions in a different group (evaluating the tomography using the Marshall scale).
The data was taken directly from the clinical record, either electronic or, at Archive area requesting the record. It will be valued the relationship between the clinical findings and the imaging study; the patients may present different lesions detected by the tomography, so two scales will be used depending on the findings found for their classification, in the case of being a subarachnoid hemorrhage without another type of injury, the Greene scale, for the rest of the lesions the Marshall scale will be used.
The interpretation of the CT is of relevant importance, so interpretation will be sought by a specialist in the matter, which may be the Emergency physician who has the necessary training to detect problems that warrant urgent decisions and as a quality control, support is requested from a neurologist to corroborate or rule out the diagnosis.
The study included 124 patients admitted to the Emergency department with the diagnostic of TBI moderate or severe. The mean age was 46.31, with a mode of 20, a range of 77, a minimum of age of 15, and a maximum of 92-years-old. Of those 29 were women and 95 men, Figure 2 shows the percentages.
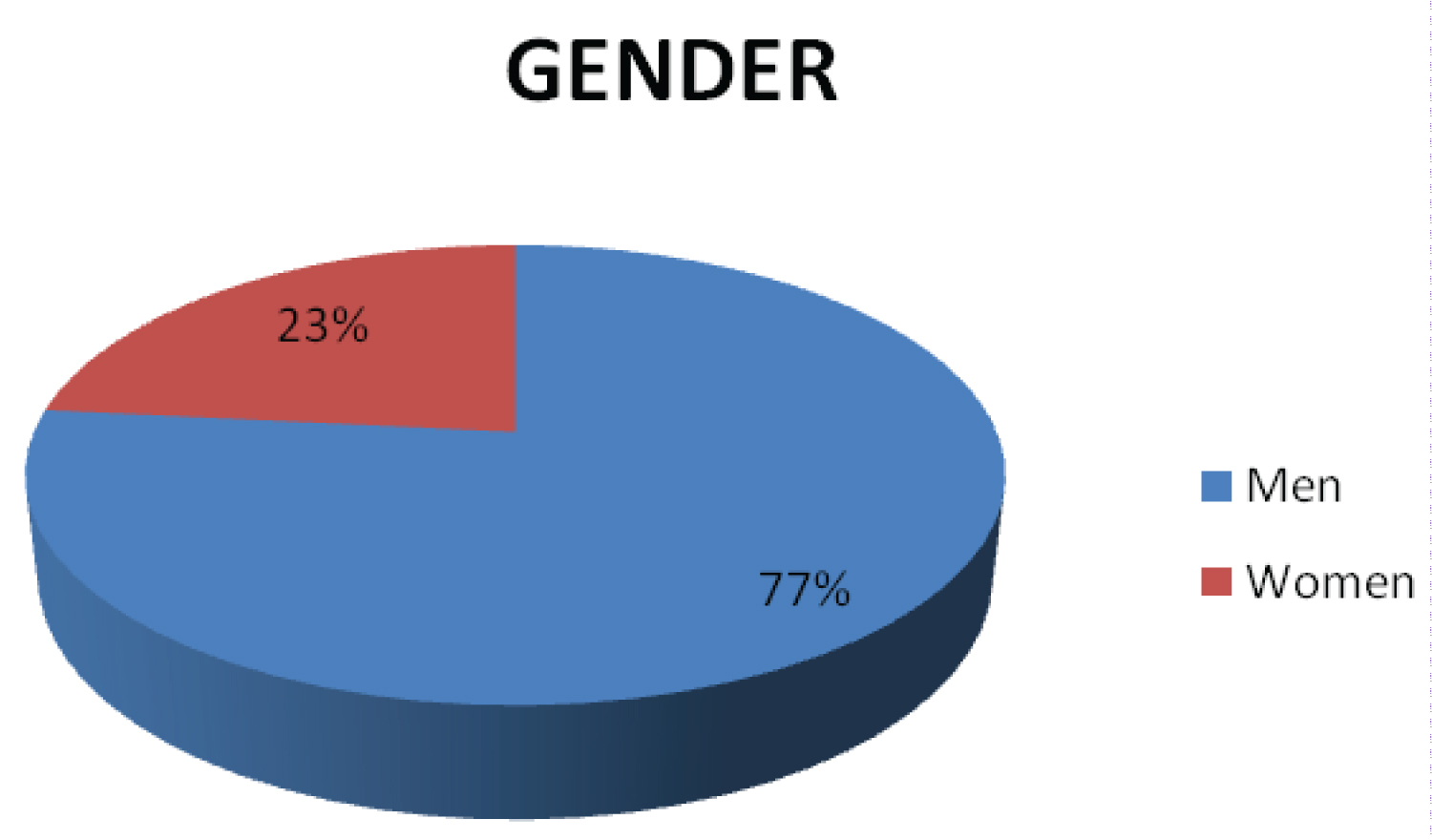 Figure 2: Percentage by Gender.
View Figure 2
Figure 2: Percentage by Gender.
View Figure 2
During the study, it was documented a relationship between the GCS, tomographic findings, and mortality. There were reported 108 survivors and 16 deaths. Within the group of surviving cases, two patients presented a GCS score of 3 points, of which one had Marshall of IV and the other had multiple injuries; 6 cases with 7-point GCS, of which presented Marshall II, III, IV, Greene 2, 4b and one case with mixed injuries. As well 78 cases with GCS of 13 points, documenting 29 cases with Marshall I, 10 with Marshall II, 2 with Marshall III, 21 with Marshall IV, 6 with Greene 1, 5 with Greene 2 and 5 with mixed injuries, this can be observe in Figure 3. In the other hand, in the group of cases that died, there were 4 cases with GCS of 3 points, 2 with Marshall IV and 2 with mixed injuries; 1 patient with GCS of 13 points with Marshall IV. This is represented in the Figure 4. With the above, a relationship is found between the GCS, tomographic findings with mortality in the group of patients who survive with p 0.41, however, no relationship is found in the group of patients who died with p .499.
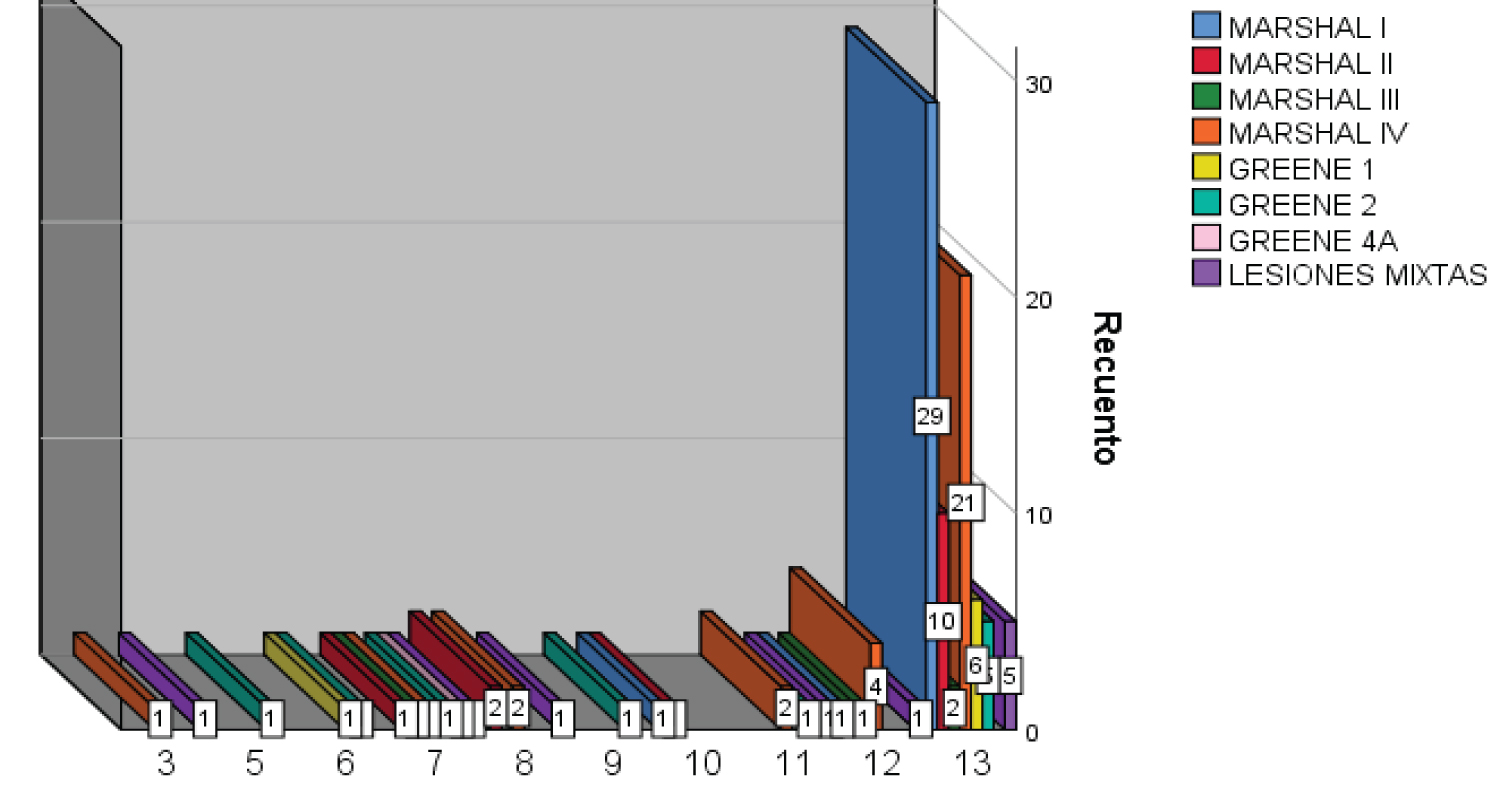 Figure 3: Surviving Cases: Relationship between GCS and Tomographic findings.
View Figure 3
Figure 3: Surviving Cases: Relationship between GCS and Tomographic findings.
View Figure 3
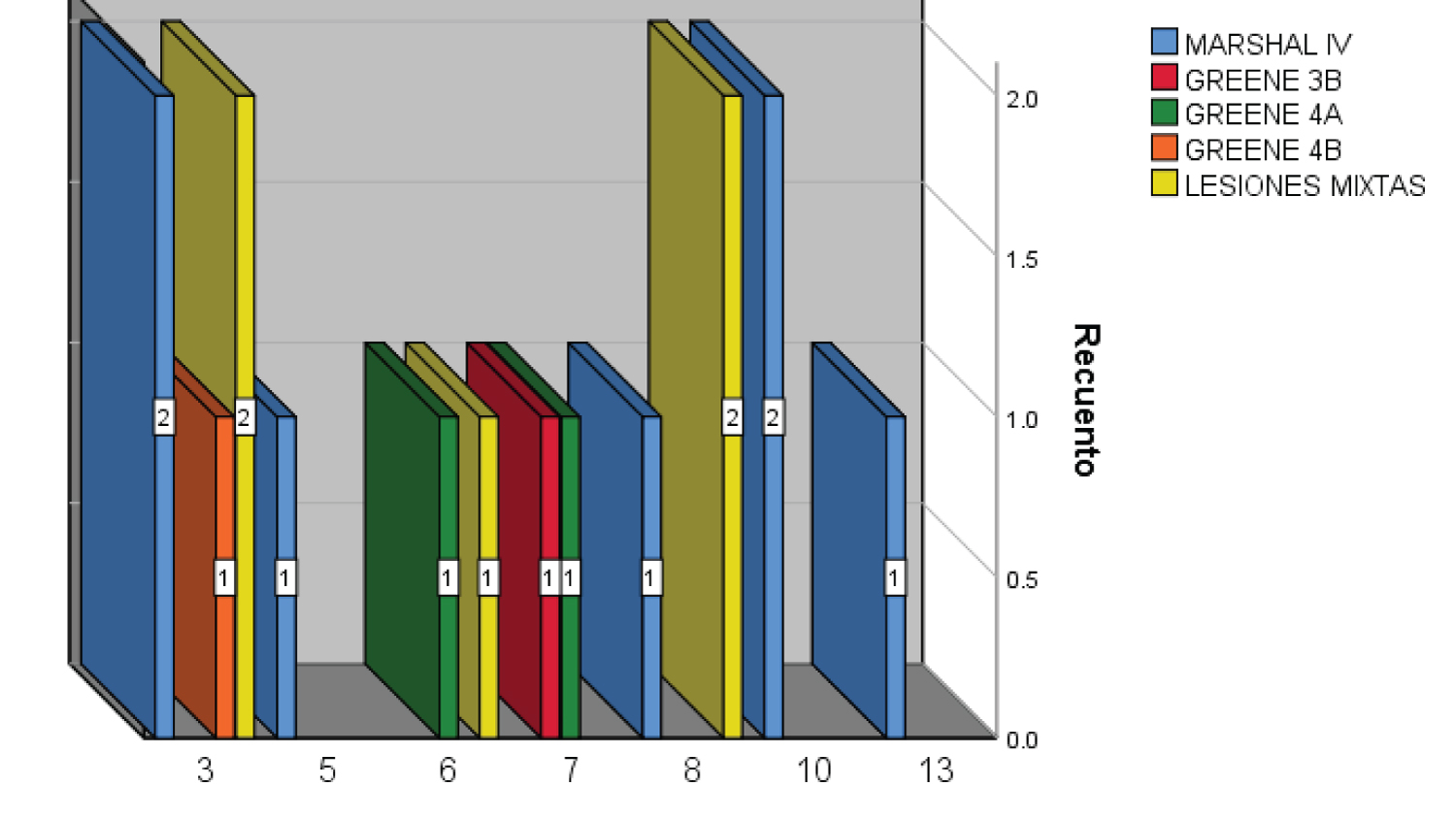 Figure 4: Deceased Patients: Relationship between GCS and Tomographic findings.
View Figure 4
Figure 4: Deceased Patients: Relationship between GCS and Tomographic findings.
View Figure 4
When seeking to determine the relationship between the GCS with in-hospital mortality, 7 cases were found with a 3-point Glasgow of which 5 died, while of the 79 cases with a 13-point Glasgow only one died, proving to be significant with p .000. This is represented in Figure 5.
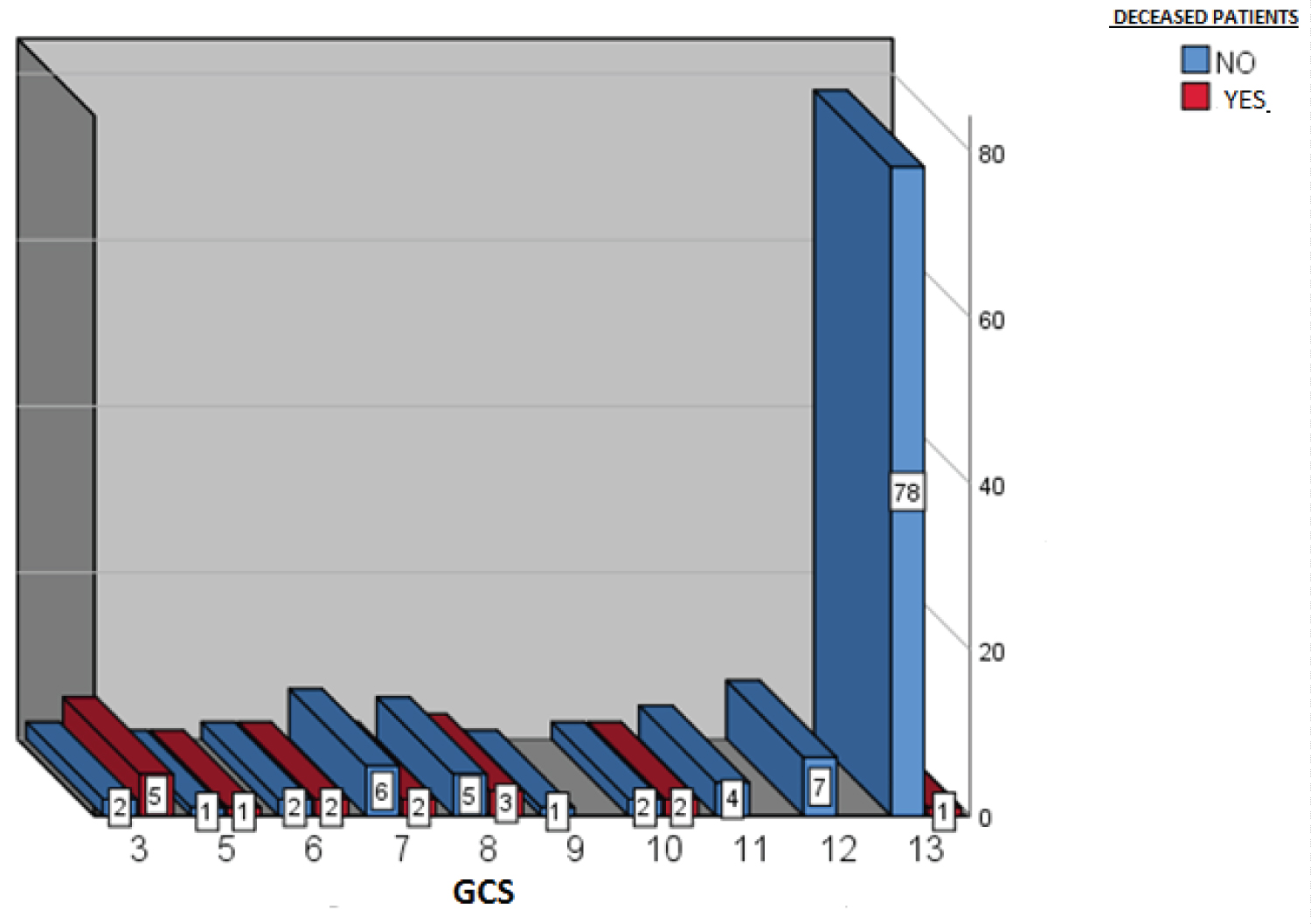 Figure 5: Relationship between the GCS and Mortality.
View Figure 5
Figure 5: Relationship between the GCS and Mortality.
View Figure 5
Regarding the correlation of tomographic findings with mortality, it was documented that in patients with Marshall I (31 cases), Marshall II (14 cases), Marshall III (4 cases), Greene 1 (7 cases), Greene 2 (10 cases) there were no deaths. However, there were reported deaths in the groups with Marshall IV (7 of 38 cases), Greene 3b (1 case), Greene 4a (2 of 3 cases), Greene 4b (1 case), and mixed lesions (5 of 15 cases). These findings show that there is a correlation between tomographic findings and mortality with statistical significance of p 0.000. This is represented in Figure 6.
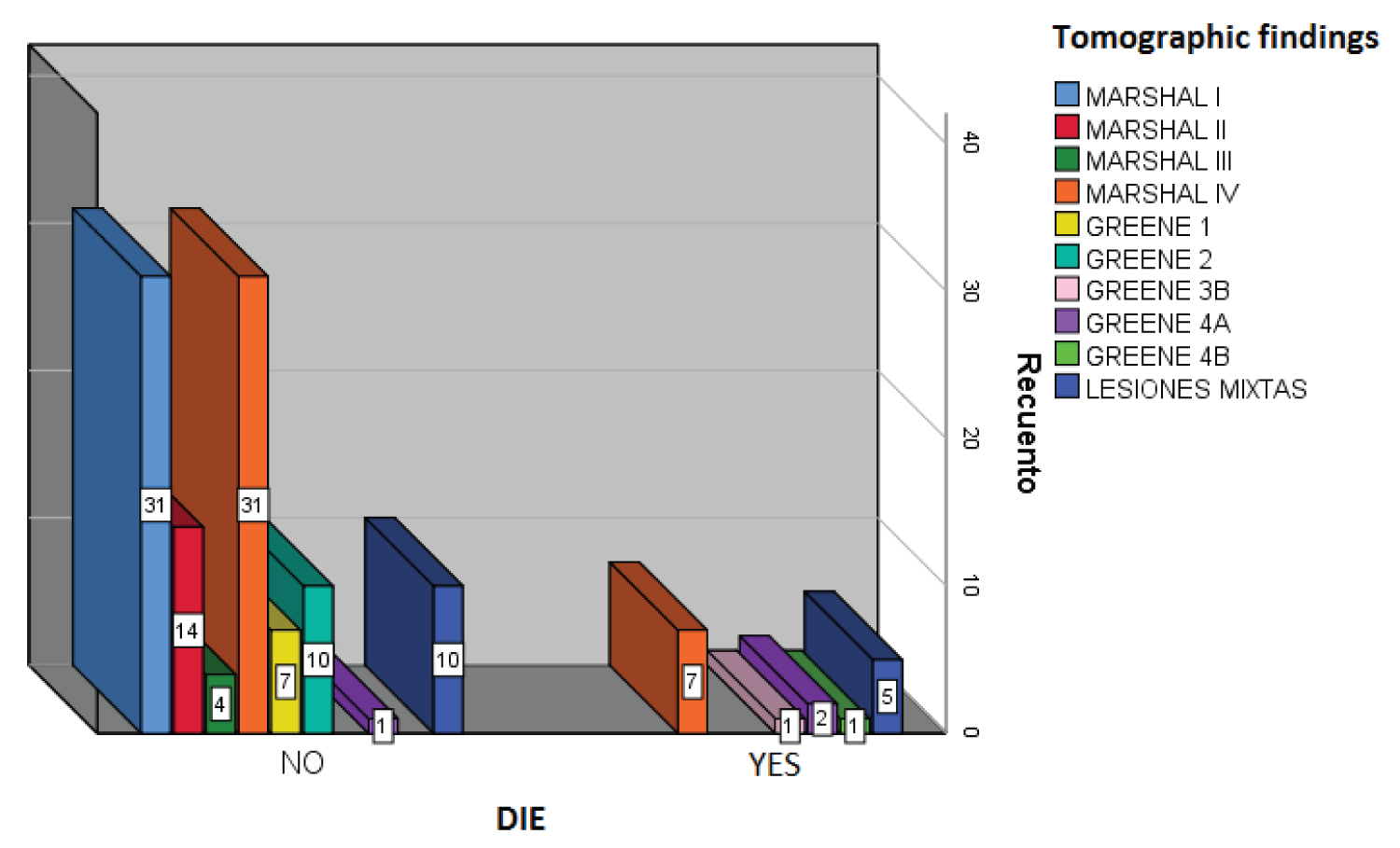 Figure 6: Correlation of Tomographic findings and Mortality.
View Figure 6
Figure 6: Correlation of Tomographic findings and Mortality.
View Figure 6
In order to establish the relationship between the GCS and the tomographic findings, we found that of the patients who presented 3-point Glasgow, 3 were classified with Marshall IV, 1 with Greene 4b and 3 with mixed injuries; While the patients with 13 points on GCS, 29 were documented with Marshall I, 10 with Marshall II, 2 with Marshall III, 22 with Marshall IV, 6 with Greene 1, 5 with Greene 2, and 5 with mixed injuries. Showing a relationship with statistical significance of p 0.001, this is represented in Figure 7.
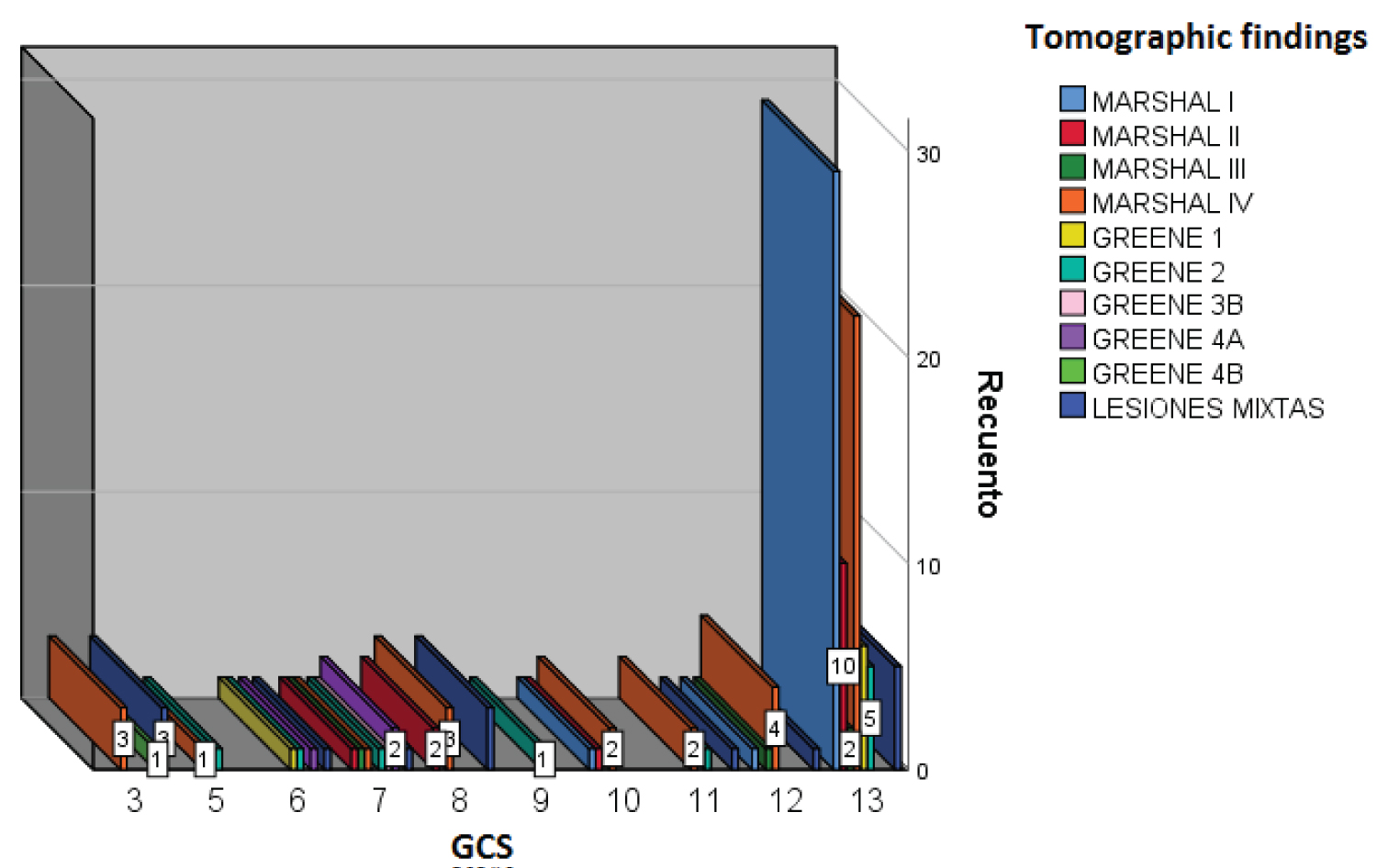 Figure 7: Relationship between Tomographic findings and GSC.
View Figure 7
Figure 7: Relationship between Tomographic findings and GSC.
View Figure 7
Of the 124 patients, 31 cases did not present injuries, 65 presented 1 injury, 18 cases with 2 injuries, 7 with 3 injuries, and 3 with 4 injuries (Figure 8). The most frequent tomographic diagnoses were subarachnoid hemorrhage and subdural hematoma with 37 cases each, followed by hemorrhagic contusions with 17 cases and epidural hematoma with 15. The least frequent finding documented is fracture with 14 cases. The tomographic diagnoses can be seen in Figure 9.
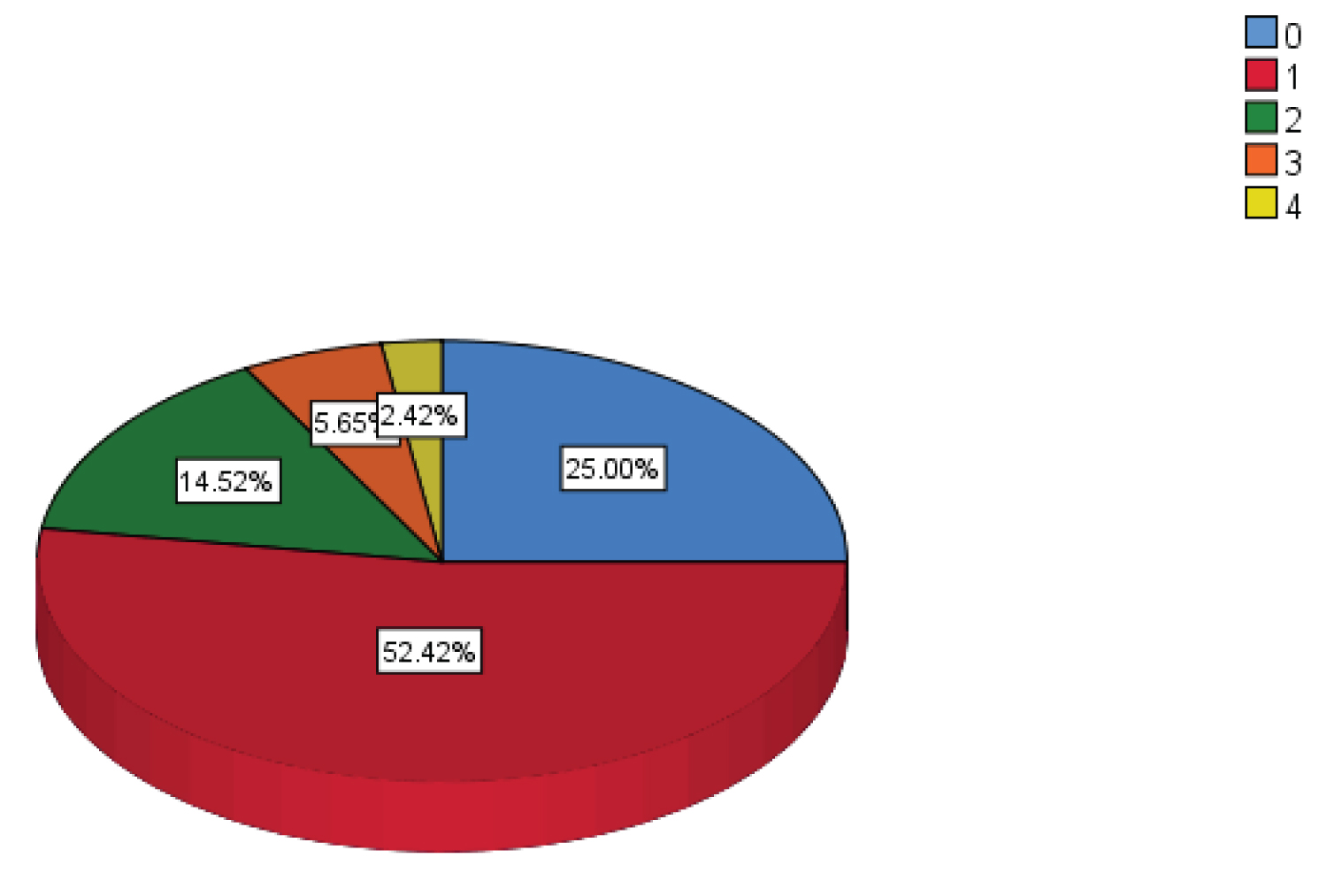 Figure 8: Percentage of Number of Injuries.
View Figure 8
Figure 8: Percentage of Number of Injuries.
View Figure 8
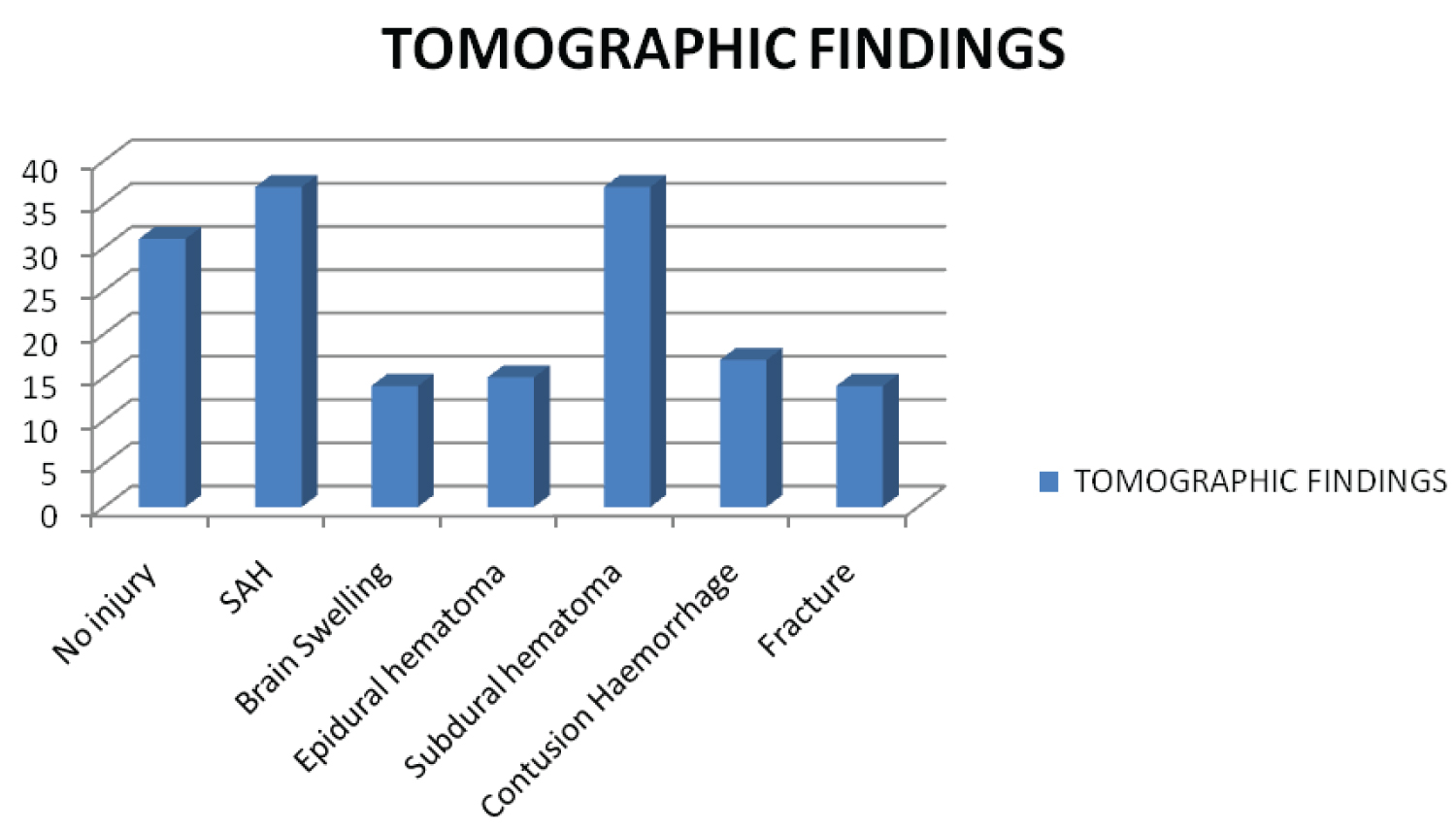 Figure 9: Frequency of Tomographic Findings.
View Figure 9
Figure 9: Frequency of Tomographic Findings.
View Figure 9
It was registered 84 patients who received conservative management, while 40 cases received surgical management, as shown in Figure 10.
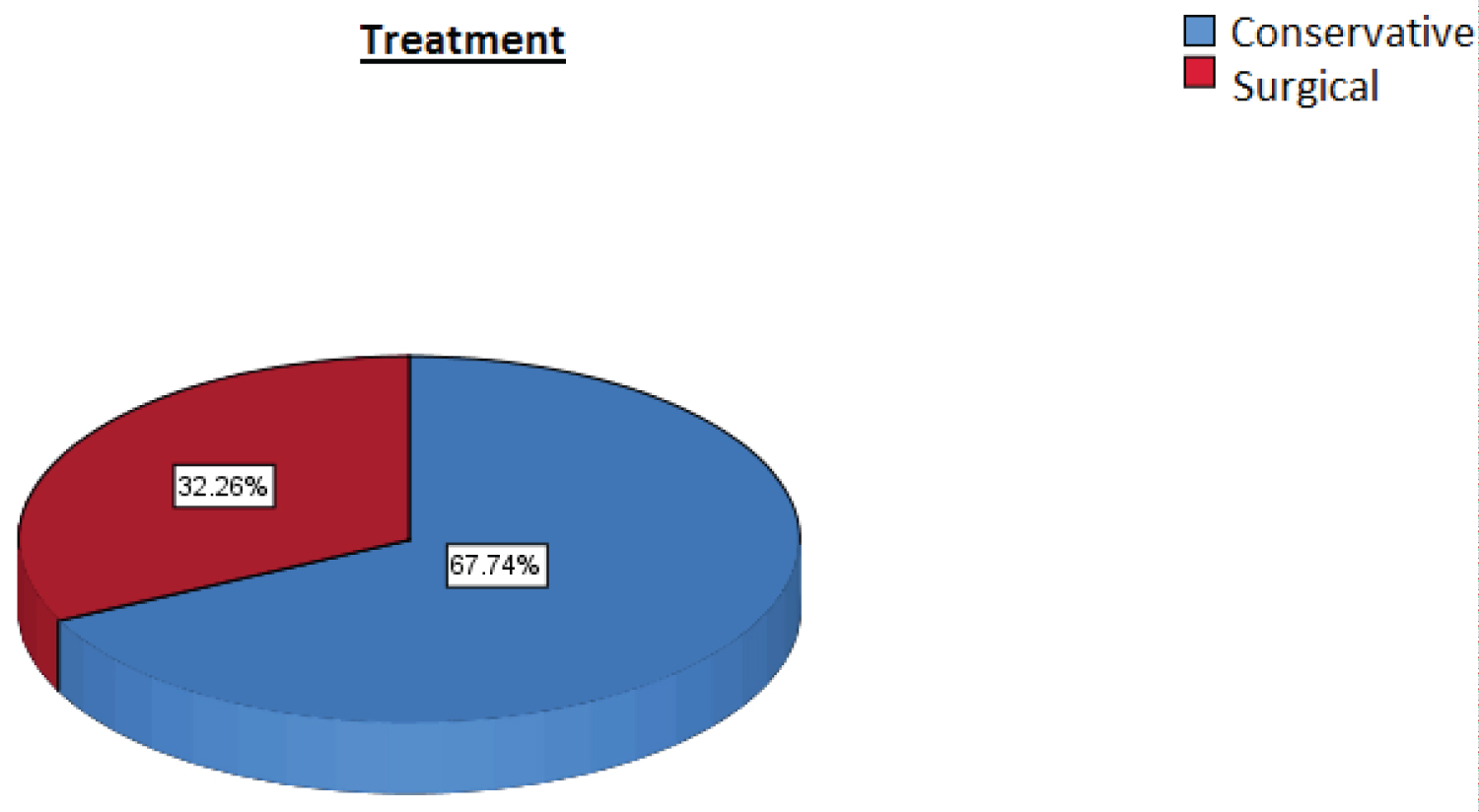 Figure 10: Percentage of Surgical and Non-Surgical Patients.
View Figure 10
Figure 10: Percentage of Surgical and Non-Surgical Patients.
View Figure 10
The aim of our study was to determine the correlation of the Glasgow coma scale score and tomographic findings with in-hospital mortality in patients admitted to the emergency department of the HGZ 50.
A Traumatic brain injury (TBI) is caused by sudden exchange of mechanical energy that causes cranial injury [2]. The severity can vary from mild to severe; it is a condition with a high morbidity and mortality worldwide, affecting 10 million people [1]. A considerable number of survivors suffer from disabling injuries. In our country it is one of the main causes of death. It has been documented that it is more frequent in males, between the ages of 15 and 45 [2].
In our study, 108 survivors and 16 deaths were documented. Within the group of surviving cases, two patients presented a GCS score of 3 points, of which one had Marshall of IV and the other with multiple injuries. As well 78 cases with Glasgow of 13 points, documenting 29 cases with Marshall I, 10 with Marshall II, 2 with Marshall III, 21 with Marshall IV, 6 with Greene 1, 5 with Greene 2 and 5 with mixed injuries. While in the group of cases that died, there were 4 cases with 3-point Glasgow, 2 with Marshall IV and 2 with mixed injuries; 1 patient with Glasgow of 13 points with Marshall IV. There were no deaths in patients with Marshall I, II, III, or Greene 1 and 2. With the above, a relationship is found between Glasgow coma score, tomographic findings with mortality in the group of patients who survive, however no relationship is found in the group of patients who died.
Chang M. in 2011, conducted a cohort study in the Emergency Unit of the Hospital "Luis Vernaza" in Ecuador with the diagnosis of moderate or severe TBI, with the title "Clinical-tomographic relationship (GCS-Marshall) with the stage of the Glasgow Outcome Scale in Patients With Moderate-Severe Head TBI. "Luis Vernaza Hospital" during July-September 2010. The patients were evaluated with the Marshall tomographic classification and initial score of the Glasgow coma scale. Documenting that both the GCS and the Marshall tomographic classification are significantly related to the prognosis, for which they have proven to be useful tools to predict the recovery of patients with moderate-severe TBI, being the GCS more reliable. It is statistically demonstrated that the higher the GCS value on admission, the better the recovery and functionality will be obtained at discharge or after 30 days of hospital stay. Regarding the Marshall classification, it was documented that the greater the intracranial lesion evidenced in the tomography, the patient will have a worse clinical status at discharge or 30 days of hospitalization [20].
On the other hand, Esquivel M. in 2004 carried out a retrospective descriptive investigation, in which 50 cases of patients who died from TBI were studied in Mexico between January 1997 and February 2000, with the title of "Clinical-tomographic analysis of patients who died from head trauma (TBI) in Mexico Hospital". The degree of injury with the most patients according to Marshall's topographic classification for TBI was grade VI in 46% of the cases; of these, 14 patients had severe TBI, 6 moderate and 3 mild. The second grade of injury with the most cases was Marshall III with 9 patients, all with severe TBI in relation to Glasgow at admission. In injury grade I (no pathology in the CT scan), 8 cases (16%) were grouped, of which 4 were mild TBI and 4 were severe TBI [21].
The results of the aforementioned authors support the findings of our research, since in these studies it is observed that the higher the Glasgow coma score, the lower the mortality. As well as the greater the intracranial injury, the greater the mortality. However, in these studies it was not classified by Greene, nor was death documented by degree of severity or by tomographic findings.
In our study, a relationship was found between the Glasgow coma scale score and in-hospital mortality, since patients with a higher score had lower mortality. Seven cases with Glasgow of 3 points were documented, of which 5 died, while of the 79 cases with Glasgow of 13 points, only one died.
Chang M. (2011) in his study shows statistically that the higher the GCS value upon admission, the better the recovery and functionality at discharge will be obtained.
As previously described in both studies, a relationship was found, however in the study by Chang M. no mortality was specified by score.
A correlation was also found between tomographic findings with the mortality of patients with TBI, the greater the injury, higher mortality. It was documented that the patients with Marshall I to III, and Greene 1 and 2 had no deaths, unlike the groups with Marshall IV, Greene 3-4 and mixed injuries.
In 2014 Cruz A. carried out an investigation of cases (deceased) and controls (alive), between 2009-2012, in the ICU of the Vladimir Ilich Lenin University General Hospital in Holguín, with the title "Predictive factors of mortality due to severe TBI". In which the greater the severity of intracranial injuries according to Marshall III-IV classification, subdural hematoma and post-traumatic subarachnoid hemorrhage were associated with mortality [22].
In our investigation, a higher mortality was documented with Marshal IIV, Greene 3-4 and mixed injuries. While in the study by Cruz A. a higher mortality is reported from Marshall III and IV, it is not classified by Greene.
Other data found in the investigation was the relationship between the Glasgow coma scale with the tomographic findings. It was documented that the lower the Glasgow score, the greater the intracranial injury.
Chang M. in his study found that both GCS and Marshall scales were related, that is to say that the symptoms were related to what was evidenced in the tomographic images and an inverse correlation was indeed obtained.
As we can see, the result of the mentioned author supports the results obtained in our study. Finding that of the patients with 3-point Glasgow, 3 were classified with Marshall IV, 1 with Greene 4b and 3 with mixed injuries.
The most frequent tomographic diagnoses were subarachnoid hemorrhage and subdural hematoma, followed by hemorrhagic contusions and epidural hematoma.
Rodríguez M. in 2010 carried out a descriptive and cross-sectional study of 62 patients with TBI, admitted to the Provincial Teaching Hospital "Saturnino Lora" in Santiago Cuba, from January 2005 to May 2006, with the title "Value of tomography Computerized Axis for the Early Diagnosis of TBI". Where the most frequent lesion is the intraparenchymal hematoma (29%), followed by the subdural and epidural, brain contusion, multiple injuries, and brain swelling [23].
In this case, the results of the aforementioned author differ from our findings since Rodríguez mentions intraparenchymal hematoma as the most frequent diagnosis, while in our document study subarachnoid hemorrhage as the most frequent diagnosis.
Our study demonstrated a high mortality in patients with tomographic findings with severe lesions, and its relationship with the Glasgow coma scale, therefore, in an initial evaluation in the emergency department with a low Glasgow punctuation, the actions of neuroprotection should initiate even before having a tomographic study, which could make the difference between life and in-hospital death.
On the other hand, when having tomographic findings with serious injuries, should also alert the emergency doctor to carry out early consultation for neurosurgery, which could also modify the outcome of the patient. In this regard, considering microplanning, a neurosurgeon should be available whenever a patient is admitted to the emergency room.