We present a complex case of a 50-year-old man who presented with inferior ST-elevation myocardial infarction and cardiogenic shock. Our patient presented with out-of-hospital ventricular fibrillation cardiac arrest. Cardiopulmonary resuscitation was promptly started and return of spontaneous circulation was achieved. The patient underwent urgent coronary angiography with implantation of drug-eluting stent in his right coronary artery. Intra-aortic balloon pump was inserted. However, this was complicated by worsening of left ventricular outflow tract obstruction and systolic anterior motion of mitral valve leaflet. He was successfully weaned off balloon pump, inotropes and liberated from mechanical ventilation. To our knowledge, this is the first case reported of balloon pump associated left ventricular outflow tract obstruction in a setting of inferior myocardial infarction. This case illustrates the importance of early removal of balloon pump and precise use vasopressor in instituting the stepwise treatment modalities leading to a favourable outcome.
A 50-year-old man presented with out-of-hospital ventricular fibrillation (VF) cardiac arrest from inferior ST-elevation myocardial infarction. The patient was intubated and started on intravenous (IV) noradrenaline. Primary percutaneous coronary intervention (PCI) was done to his right coronary artery (RCA) with implantation of drug-eluting stent. Intra-aortic balloon pump (IABP) was inserted in view of escalating pressor requirement and cardiogenic shock. American Heart Association (AHA) gave a class 2A indication [1] for IABP counterpulsation in the setting of cardiogenic shock. However, long term 6-year outcome of IABP-Shock II trial [2] did not demonstrate a reduction in mortality in the setting of cardiogenic shock. Left ventricular outflow tract obstruction (LVOTO) has been described in Takotsubo cardiomyopathy [3] and acute anterior myocardial infarction (MI) [4]. To our knowledge, we describe the first report of LVOTO worsened by IABP insertion in the context of inferior myocardial infarction. We present the following case in accordance with the CARE reporting checklist.
A 50-year-old male with no significant history apart from smoking history presented with VF arrest. Cardiopulmonary resuscitation and immediate defibrillation were done on-site by paramedic. His no-flow time was 5 minutes whereas his low-flow time was close to 25 minutes. His examination was remarkable for a bilateral lung crepitations but there was no audible murmur. His 12-lead electrocardiogram (ECG) showed sinus tachycardia with ST elevation in the inferior leads (Figure 1). He was given oral aspirin, ticagrelor and intravenous frusemide. However, he developed cardiogenic shock and acute respiratory failure and he was intubated. Urgent coronary angiogram showed triple vessel disease with acute occlusion of right coronary artery (Video 1 and Video 2). The left anterior descending artery was 100% occluded and it received collaterals from the right coronary artery.
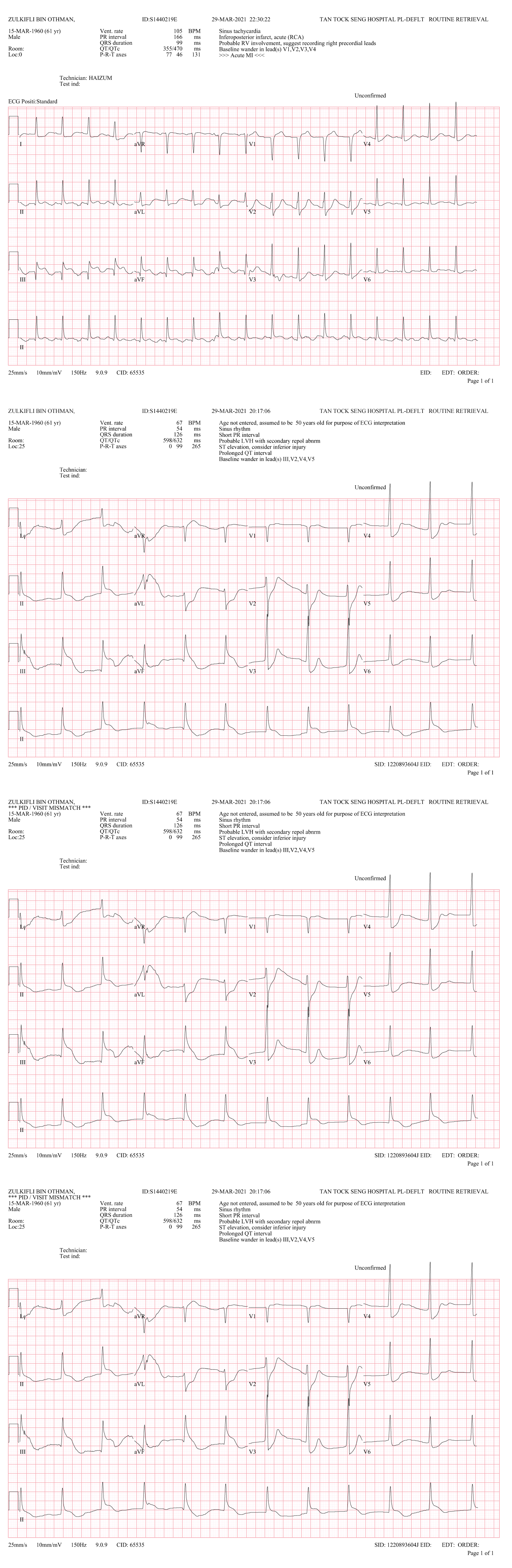 Figure 1: Electrocardiogram (ECG) showed sinus tachycardia with ST elevation in the inferior leads. View Figure 1
Figure 1: Electrocardiogram (ECG) showed sinus tachycardia with ST elevation in the inferior leads. View Figure 1
Video 1: Coronary angiogram showed acute occlusion of right coronary artery. View Video 1
Video 2: Coronary angiogram revealed 100% occluded left anterior descending artery receiving collaterals from right coronary system. View Video 2
The patient became hypotensive after catheterization, with systolic pressures measures between 80 and 90 mmHg. IABP was inserted and vasopressin was added. Immediate transthoracic echocardiogram (TTE) showed left ventricular ejection fraction (LVEF) of 45% with systolic anterior motion (SAM) of the anterior mitral leaflet and LVOT gradient of 127 mmHg (Video 3 and Figure 2). He underwent thrombus aspiration and balloon angioplasty using a Ryurei 2.0 × 15 mm NC balloon, inflated with high pressure under intravascular ultrasound guidance Drug-eluting stent (Ony × 3.5 × 10 mm) was implanted on the right coronary artery with re-establishment of TIMI 3 flow (Video 4).
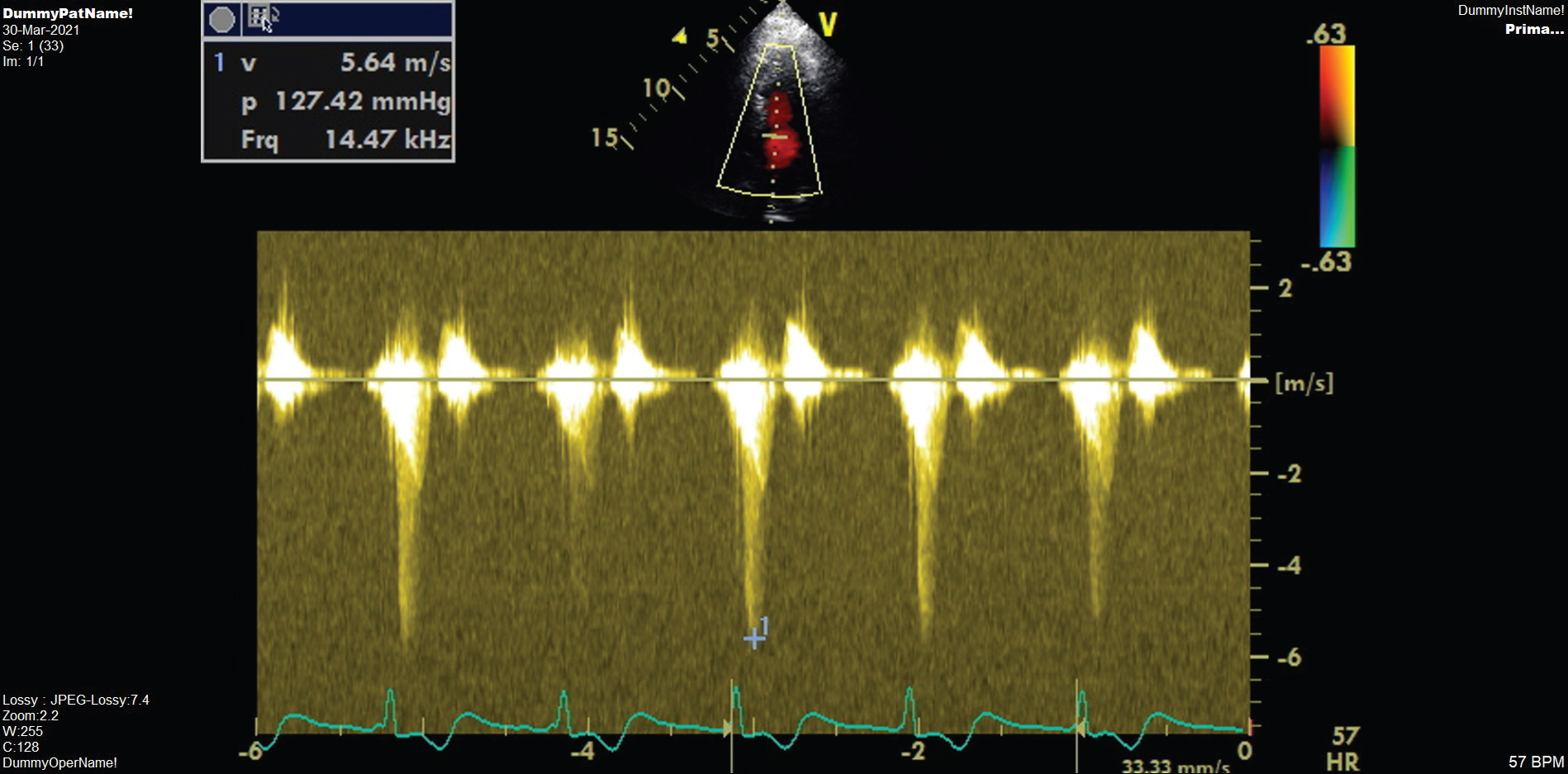 Figure 2: Transthoracic echocardiogram showed peak gradient of 127 mmHg in LVOT. View Figure 2
Figure 2: Transthoracic echocardiogram showed peak gradient of 127 mmHg in LVOT. View Figure 2
Video 3: Apical 3-chamber view illustrates hypokinesia in the inferior wall and SAM of anterior mitral valve leaflet. View Video 3
Video 4: Re-establishment of TIMI 3 flow after drug eluting stent implantation. View Video 4
His maximum troponin was 22,000 ng/L. He was treated with targeted temperature management at 33 C, IV Piperacillin-Tazobactam, hydrocortisone 50 mg 6 hourly and Atorvastatin 40 mg daily. The patient subsequently suffered downstream complication of cardiogenic shock, i.e., ischemic hepatitis, acute kidney injury and ventilator associated pneumonia. His lactate was elevated at 10.9 mmol/L, total white count 22 × 10^9/L, creatinine 300 umol/L and alkaline phosphatase elevated at 500 IU/L.
IABP was subsequently placed on 1:3 augmentation and intravenous phenylephrine initiated in view of significant LVOTO. Intravenous fluid boluses were given based on dynamic parameters of fluid responsiveness. Volume View (Edwards Life science) was used as a tool for hemodynamic monitoring. The blood pressure improved significantly with these measures. Vasopressin (maximum infusion rate of 1.8 IU/kg/hr) and Noradrenaline (maximum infusion rate of 0.6 mcg/kg/min) were gradually weaned off with no rebound hypotension. IABP was removed with vascular closure device on day 4 of ICU stay. His heart rate remained well controlled with IV Esmolol and Remifentanil infusion. He was promptly liberated from mechanical ventilation on Day 6 of hospitalization. His kidney and liver function improved gradually with no requirement for renal replacement therapy. A repeat TTE demonstrated no LVOTO with a peak gradient of 5.53 mmHg (Figure 3). There was concentric hypertrophy, mild chordal SAM with marked improvement of LVEF to 55% (Video 5).
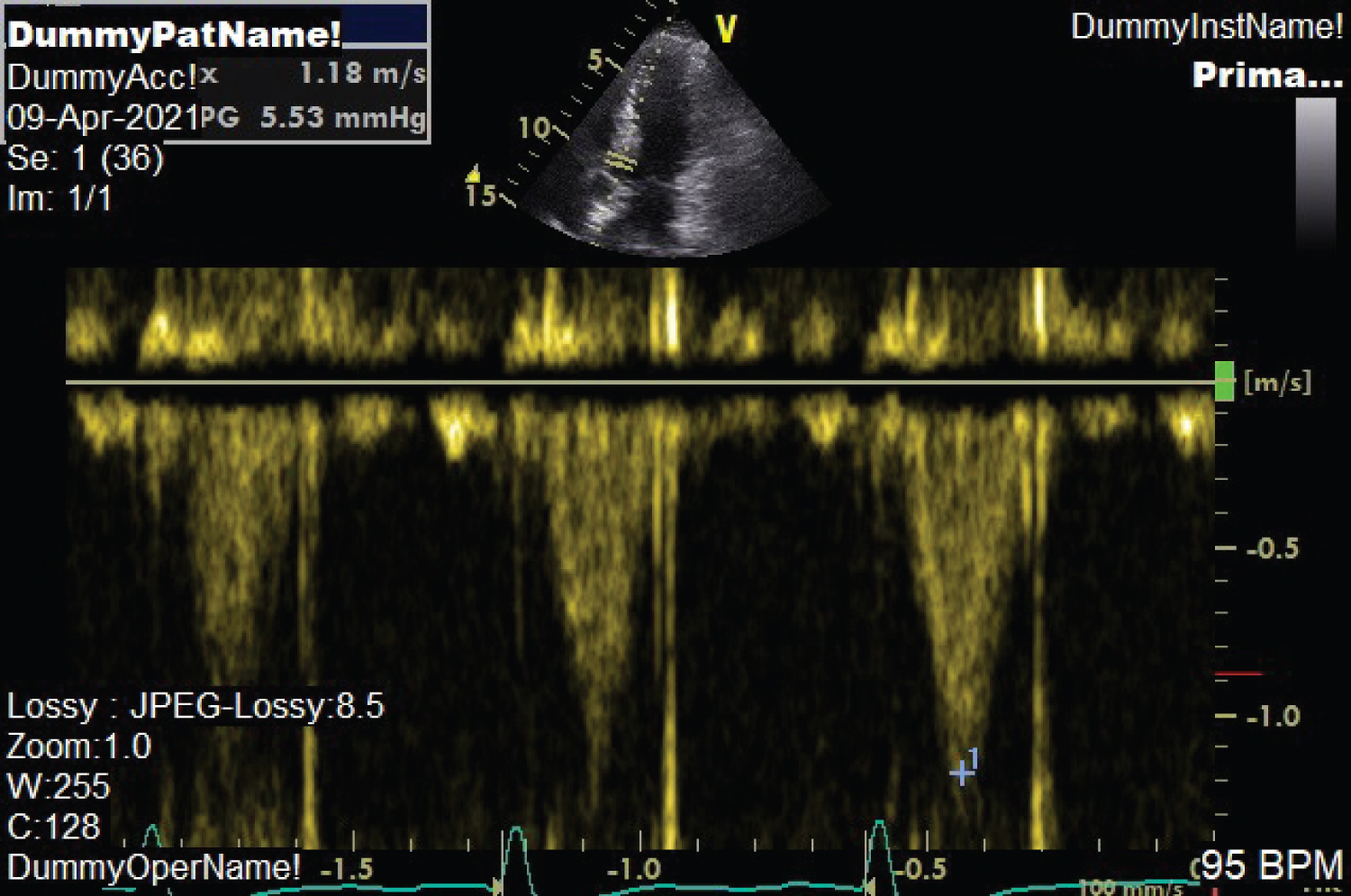 Figure 3: Resolution of LVOT peak gradient to 5 mmHg. View Figure 3
Figure 3: Resolution of LVOT peak gradient to 5 mmHg. View Figure 3
Video 5: Apical 3-chamber view showed normal wall motion with mild chordal SAM. View Video 5
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient.
We present a case of refractory cardiogenic shock due to dynamic LVOTO worsened by IABP counterpulsation. The major tool for assessment of LVOTO, however, is echocardiography. The spectral Doppler waveform in our patient fits with the typical late peaking or dagger shape pattern found in dynamic LVOTO [5].
Numerous reports have highlighted the occurrence of dynamic LVOTO as a complication of ST-Elevation myocardial infarction (STEMI) [6,7]. The actual incidence of these findings is unclear, but it may be significantly underdiagnosed and can indeed mimic cardiogenic shock in an acute-care setting. Failure of the anterior mitral valve leaflet to coapt with the posterior leaflet in systole results in MR. The degree and duration of mitral SAM determine the severity of the dynamic LVOTO gradients and MR [8-10]. Although classically described in hypertrophic cardiomyopathy, SAM and LVOTO can result from various clinical settings. We speculated that compensatory basal LV hypercontractility based upon mild LV narrowing led to SAM, and initiation of IABP further deteriorated dynamic LVOTO, which result in intractable cardiogenic shock. Loss of normal ventricular geometry may also affect the tension and position of the mitral valve apparatus making SAM more apparent. In addition, the right coronary artery was supplying collaterals to the chronically occluded left anterior descending artery. Loss of flow in most of the LV myocardium precipitated the ventricular arrhythmia as well as cardiogenic shock.
The inotropic effects of most vasopressors and the stress of critical illness in the setting of a low intravascular volume state may provoke LVOTO in susceptible patients [11,12]. Inotropes also promote hypercontractility [13,14], accelerate blood across the LVOT and worsen SAM of the anterior mitral valve leaflet. Unrecognized LVOTO may lead to a spiral of inappropriate vasopressor/inotrope use resulting in severe hypotension, collapse, and death. In many patients the onset of LVOTO is unexpected and gradients can vary significantly over a short period of time [15]. Given its unpredictable nature, the presence of dynamic LVOTO in a hypotensive critically ill patient should always be considered. Correct therapy involves avoidance of hypovolemia, using beta blockers to reduce the hypercontractile state and alpha agonist (Phenylephrine) to increase the systemic vascular resistance and reduce the LVOT gradient.
Clinical suspicion, early recognition, and appropriate management of LVOTO, along with addressing of STEMI, would significantly improve the outcome in this critically ill patient. In our patient, we showed that withdrawing inotropes and IABP timely improved his hypotension markedly.
The authors have completed the CARE reposting checklist.
All authors report no conflict of interest.
This report was in accordance with institutional ethical standards and in accordance with Helsinki Declaration. This case report has non-identifiable clinical data of our patient.
None declared.