Recently, R. Kummer, et al. [1] described a paradoxical and reproducible improvement of respiratory system compliance (Crs) after abdominal compression in seven mechanically ventilated severe COVID-19 patients. Indeed, we have also noticed these counter intuitive phenomena, since increased intra-abdominal pressure in ARDS patients is usually associated with a decrease of Crs [2]. In this brief report, we describe the case of one of our patients and suggest a possible therapeutic intervention by applying a continuous lower abdominal compression (LAC).
We report the case of sixty-years-old men who necessitated intubation and mechanical ventilation for severe COVID-19. After 3 days under mechanical ventilation, in semi recumbent position, despite being ventilated with 5.5 ml/kg/IBW and 8 cmH2O of positive end expiratory pressure (PEEP), deeply sedated and paralyzed, his plateau pressure (Pplat) was markedly elevated at 41 cmH2O. However, we noticed that placing our patient in supine position his Pplat decreased to 28 cmH2O. However, due to well-known complication associated with supine position in patients under mechanical ventilation (e.g., ventilator associated pneumonia), we couldn’t let the patient in this position [2].
In an attempt to find an explanation of these phenomena, we applied a lower abdominal compression (LAC) in semi recumbent and observed a drastically decreased of his Pplat from 41 to 24 cmH2O, returning to the previous value as soon as LAC was released. Therefore, we decided to place a bag of fluid on his abdomen in order to maintain the benefit of the LAC (Figure 1). Measuring the pressure inside the bag saline applied on the lower abdomen we measured a value of 40 cmH2O needed to improve his Pplat. For the next days, we fixed with a strap a bag of 1 liter of saline on the abdomen of the patient and let him in supine position with the net conservation of the improved Pplat and Crs.
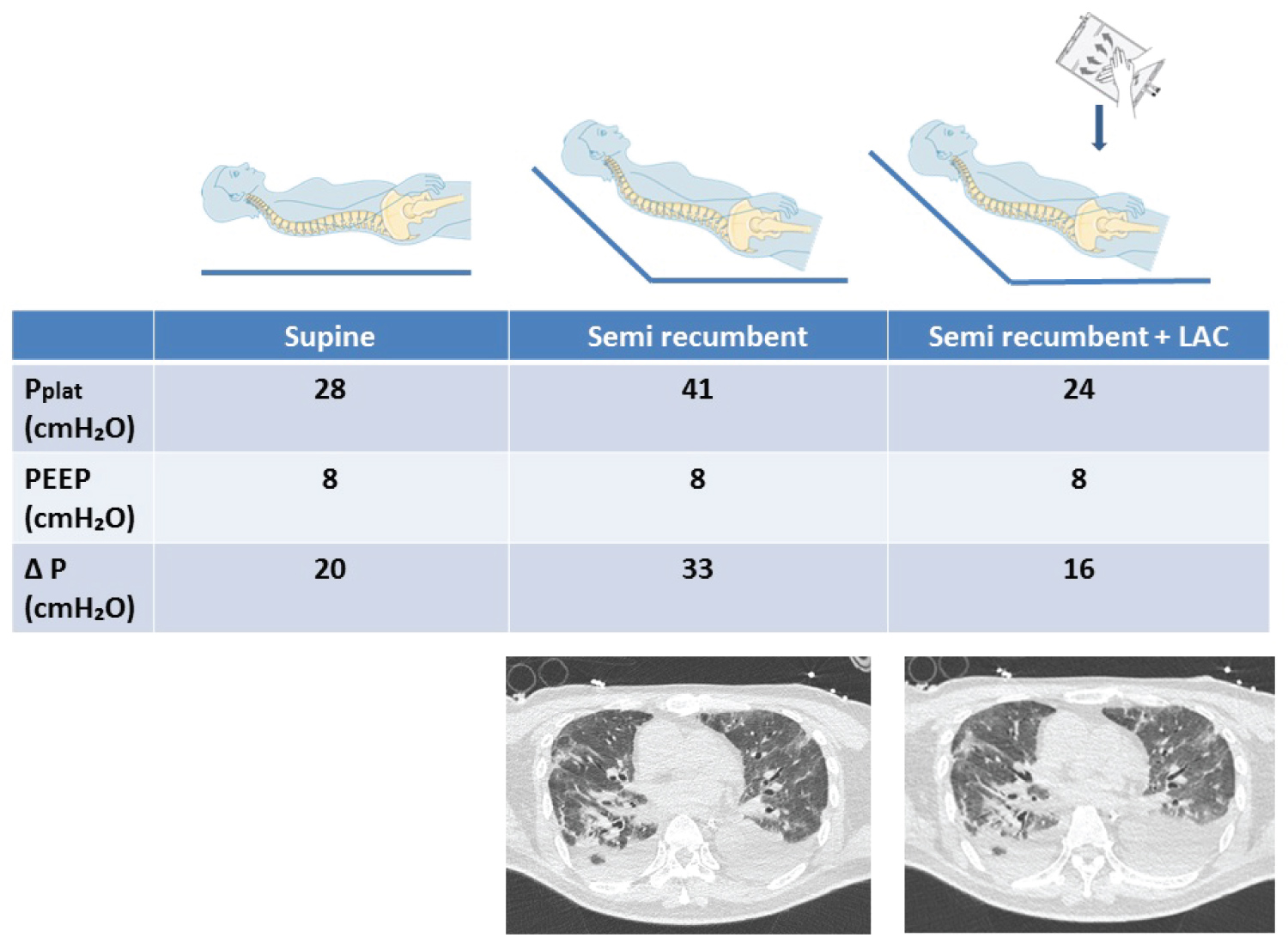 Figure 1: A lung CT scan in semi recumbent with and without abdominal compression was performed in order to assess ventilation distribution with and without LAC. View Figure 1
Figure 1: A lung CT scan in semi recumbent with and without abdominal compression was performed in order to assess ventilation distribution with and without LAC. View Figure 1
A lung CT scan in semi recumbent with and without abdominal compression was performed in order to assess ventilation distribution with and without LAC. We did not observe any difference in ventilated area with and without LAC (Figure 1).
Finally, the evolution was favorable and the patient was discharge alive from the ICU.
The significant decrease of Pplat and increase in Crs during lower abdominal compression may result from several different mechanisms as suggested by Carteaux, et al. that recently observed a similar improvement of Crs after continuous anterior chest compression [3]. LAC by increasing pleural pressure could increase the airway opening pressure of already ventilated but over distended area leading to a redistribution of tidal volume to non-aerated lung units. Indeed, Mauri, et al. have recently described an interdependence between elevated intra-abdominal, pleural, and airway pressure in severe ARDS patient [4,5].
Continuous LAC allows a sustain Crs improvement and should be try as a therapeutic option in severe ARDS patient with low Crs. However, this treatment requires further exploration of its tolerance (i.e., intra-abdominal pressure) and physiological effect in ARDS patients.
AC, VC, ED and FD designed the study and drafted the manuscript; FD drafted the manuscript; All authors approved the final version of the manuscript.
None.