In most patients, COVID-19 pneumonia initially causes significant hypoxemia but without substantial impairment of lung compliance that would increase the work of breathing (WOB). Once adequate oxygenation is established, a tool to determine WOB independent of oxygen needs can guide the decision to intubate for invasive mechanical ventilation (IMV). We monitored oxygen requirements and WOB in 10 patients admitted with severe COVID-19 pneumonia (radiographic evidence of extensive lung disease with significant hypoxemia and multiple comorbidities). Hypoxemia was successfully managed through non-invasive means, predominantly using high-flow nasal cannula. To assess WOB, we used a scale previously developed by us assigning points to the respiratory rate and use of respiratory accessory muscles (range, 1 to 7). The WOB increased consequent to increased respiratory rate but with minimal use of respiratory accessory muscles. None required intubation and all survived the ICU stay and recovered. We compared the maximal and the average WOB during their ICU stay with the WOB measured within 24 hours before intubation in four patients who required invasive mechanical ventilation. The maximal and the average WOB were lower in patients not requiring intubation (mean ± SD, maximal 4.3 ± 0.9 vs. 5.5 ± 1.0 pts, p = 0.028 and average 2.7 ± 0.6 vs. 3.9 ± 0.5 pts, p = 0.002). Accordingly, most of our patients could be managed non-invasively delivering oxygen through high-flow nasal cannula without the need to intubate for mechanical ventilation. This approach is less resource-intense and may lead to better outcomes especially at times of high disease intensity.
A primary target of SARS-CoV-2 is the lungs with COVID-19 pneumonia leading to hypoxemic respiratory failure and high mortality. Early reports of rapid deterioration in patients suffering COVID-19 pneumonia encouraged expedited intubation to avert life-threatening and more difficult to manage crises [1,2]. Less invasive interventions commonly used to support acute respiratory failure, including noninvasive mechanical ventilation and oxygen delivery through high-flow nasal cannula (HFNC), were perceived as less effective and thus potentially detrimental by delaying intubation while exposing healthcare workers to the release of aerosols containing viral particles [1,2]. These concerns resulted in a low threshold for intubation and initiation of mechanical ventilation often without concerted efforts to attempt and assess the effects of less invasive interventions. Under conditions of disease surge, and especially when resources are limited, the ability to provide safe and effective mechanical ventilation for extended periods is compromised. This might explain the high mortality in excess of 65% or even 85% reported earlier in COVID-19 patients intubated for mechanical ventilation in locations experiencing high disease intensity [3-5], exceeding the less than 50% mortality associated with the traditional acute respiratory distress syndrome [6].
As the pandemic developed, it was recognized that COVID-19 pneumonia patients mostly presented with hypoxemia but without a substantial impairment in lung compliance that would significantly increase the work of breathing (WOB) [7,8]. To help recognize the need for mechanical ventilation, we used a WOB scale that we had developed based on bedside assessment of respiratory rate and use of inspiratory and expiratory respiratory accessory muscles [9]. The scale assigns points based on the respiratory rate, presence of nasal flaring, use of sternocleidomastoid muscle, and abdominal muscles and ranges from 1 (normal resting WOB) to 7 (maximal WOB). A pocket card that can be carried by healthcare providers is shown in Figure 1.
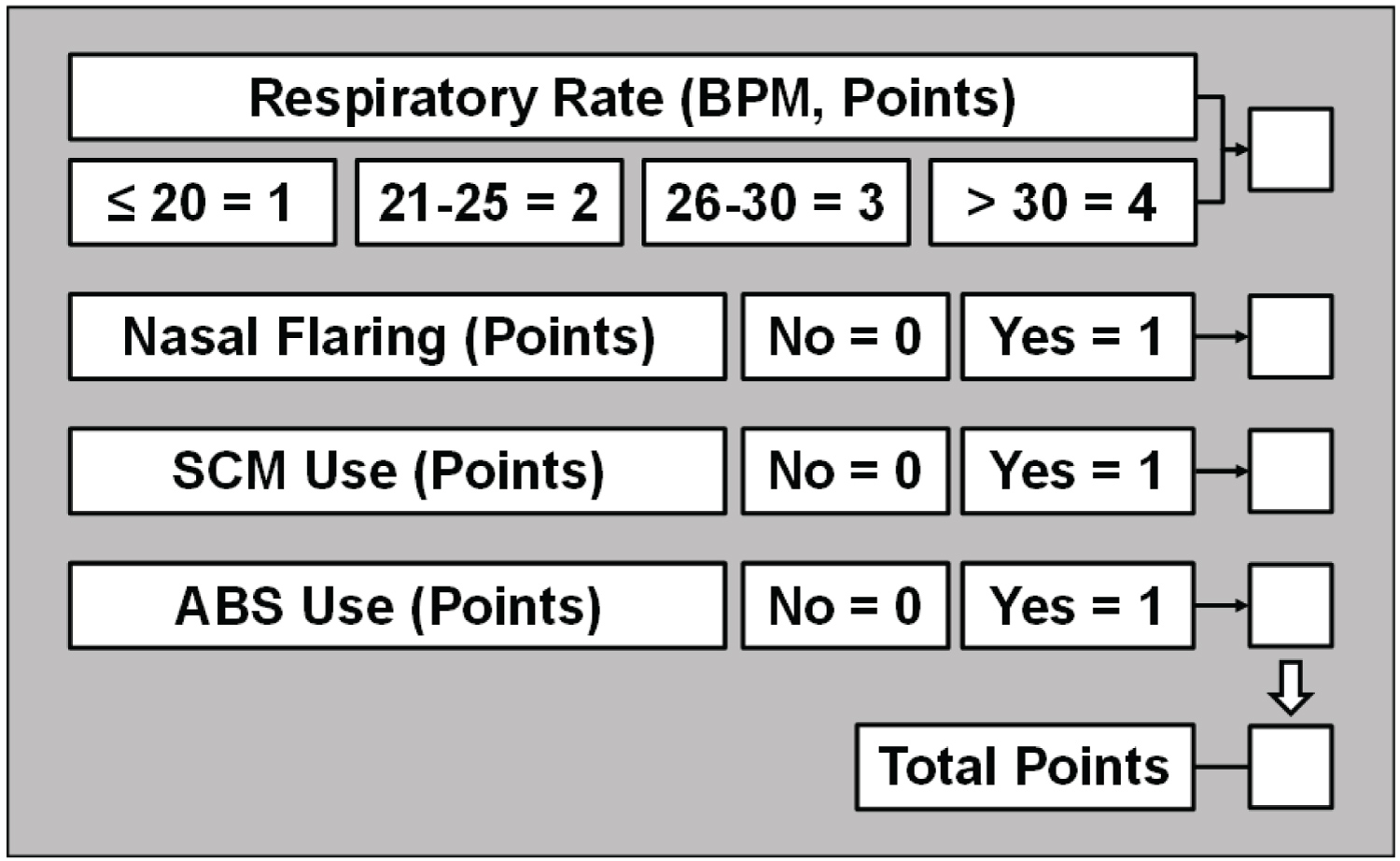 Figure 1: Work of Breathing Scale assigning points to the respiratory rate (breath per minute, BPM) and activation of inspiratory and expiratory respiratory accessory muscles. Nasal flaring is determined visually by detecting widening of the nostrils during inspiration while standing at approximately one-meter from the patient. Activation of the sternocleidomastoid (SCM) muscle is determined by gentle palpation of its clavicular insertion using two fingers from the hand ipsilateral to the patient's side noticing increased tension during inspiration. A useful way of identifying the SCM is to instruct the patient to maximally rotate his/her head away from the healthcare provider. This action prompts activation of the SCM at the end of head rotation enabling its detection with the two fingers already placed at the clavicular insertion. The patient is then instructed to turn its head to the mid-position to assess activation during inspiration. Activation of abdominal muscles (ABS) is determined by gentle palpation of the abdomen using the hand ipsilateral to the patient's side noticing increased tension during expiration. View Figure 1
Figure 1: Work of Breathing Scale assigning points to the respiratory rate (breath per minute, BPM) and activation of inspiratory and expiratory respiratory accessory muscles. Nasal flaring is determined visually by detecting widening of the nostrils during inspiration while standing at approximately one-meter from the patient. Activation of the sternocleidomastoid (SCM) muscle is determined by gentle palpation of its clavicular insertion using two fingers from the hand ipsilateral to the patient's side noticing increased tension during inspiration. A useful way of identifying the SCM is to instruct the patient to maximally rotate his/her head away from the healthcare provider. This action prompts activation of the SCM at the end of head rotation enabling its detection with the two fingers already placed at the clavicular insertion. The patient is then instructed to turn its head to the mid-position to assess activation during inspiration. Activation of abdominal muscles (ABS) is determined by gentle palpation of the abdomen using the hand ipsilateral to the patient's side noticing increased tension during expiration. View Figure 1
All patients had confirmed COVID-19 by real-time polymerase chain reaction. Admission to the ICU in all 10 patients who did not require intubation was deemed appropriate based on the need to increase oxygen flow via nasal cannula to maintain a pulse oximetry ≥ 92% and/or because the WOB increased above 3 using our bedside scale. Each of these patients at some point during their ICU stay met one or several criteria previously recommended for intubation (i.e., persistent respiratory rate > 25 bpm, failure to increase the oxygen saturation above 90% despite supplemental oxygen, bilateral infiltrates on chest imaging, or sepsis physiology) [1]. All 10 patients were male and the first 6 received hydroxychloroquine before it was discouraged by FDA. The last 2 patients received remdesivir.
As shown on Table 1, their age ranged from 33 to 89-years-old and had multiple comorbidities associated with increased severity and mortality of COVID-19 [2]. They stayed in ICU between 3 and 14 days. Nine of 10 patients received oxygen through HFNC for most of their ICU stay with a median maximal flow rate of 50 l/min (IQR; 45, 60) and a median maximal inspired oxygen of 65% (IQR; 50, 80). One patient received BiPAP for a few hours followed by oxygen through nasal cannula. IL-6 was measured in 9 patients showing markedly elevated levels. All patients had the characteristic bilateral patchy ground glass lung opacities visualized in CT scans and/or chest-X-rays. Representative images from two patients with long ICU stays are shown in Figure 2 and Figure 3. All 10 patients gradually improved surviving the ICU stay and recovered. For comparison, we assessed the WOB scale in four patients with COVID-19 pneumonia who required intubation for mechanical ventilation. We compared the maximal and the average WOB scale (and its individual components) during the entire ICU stay for the 10 patients who did not require intubation and for the preceding 24 hours in the four patients who required intubation. As shown in Figure 4, there was a statistically significantly higher maximal and average WOB level in patients who require intubation. Breakdown of the various WOB components demonstrated a statistically significantly higher average but not maximal respiratory rate in patients who required intubation. Yet, the maximal and average use of respiratory accessory muscles use (assessed as their aggregate sum) was statistically significantly higher in patients who required intubation.
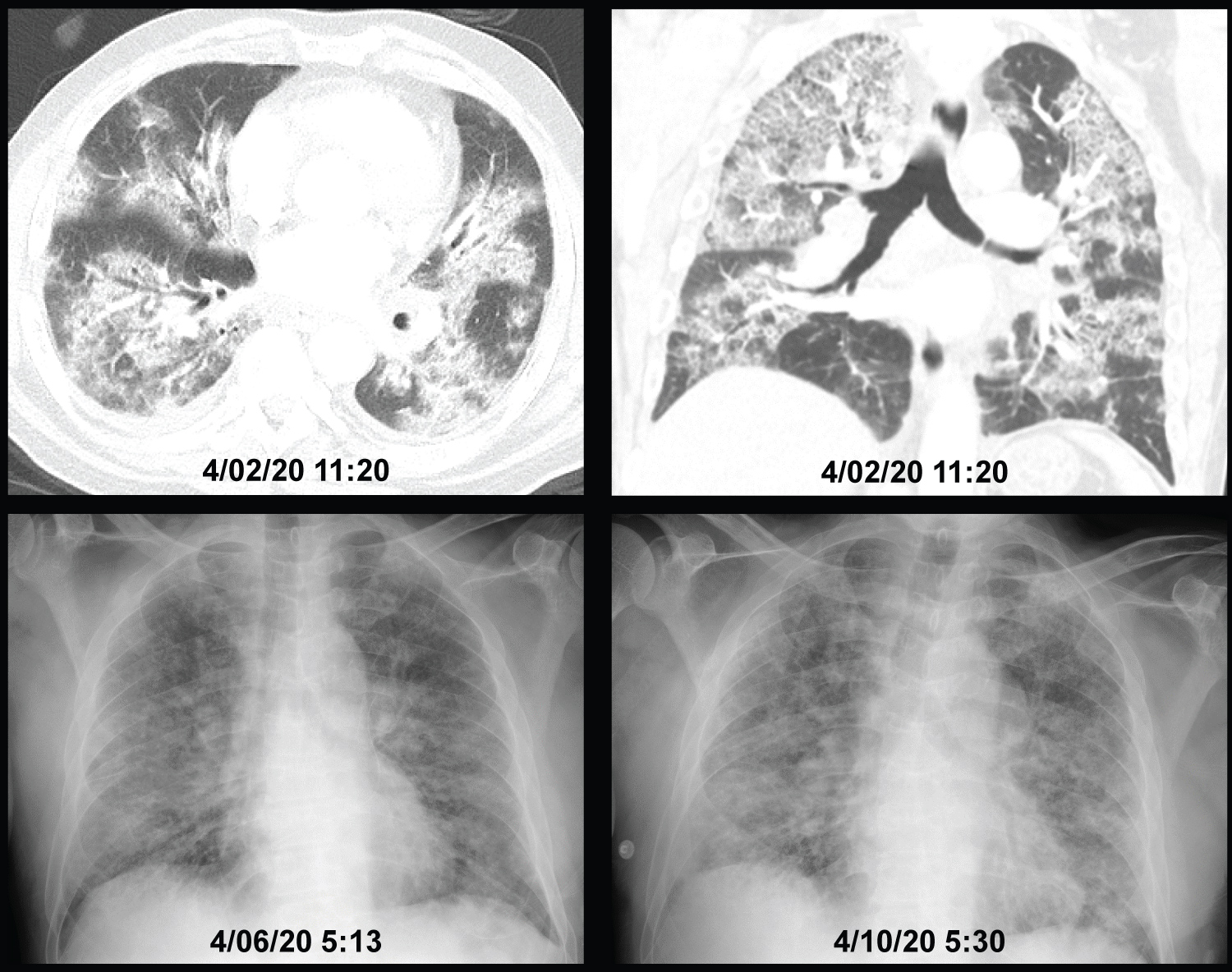 Figure 2: Patient #2, showing a CT of the chest on the day of ICU admission and chest X-rays on ICU days 4 and 8. The patient spent 9 of 10 days in ICU receiving oxygen via high-flow nasal cannula at 40 l/min throughout his stay and oxygen concentration between 70% and 80% during the initial 7 days decreasing to 40% for the last 2 days. His work of breathing averaged 3 (range 2-4) during the first 6 days improving gradually to an average of 2.5 (range 2-3) toward the end of his ICU stay without appreciable change in the chest X-ray. He was discharged from ICU once he was able to oxygenate adequately receiving oxygen through a simple nasal cannula without significant increase in the work of breathing at rest. View Figure 2
Figure 2: Patient #2, showing a CT of the chest on the day of ICU admission and chest X-rays on ICU days 4 and 8. The patient spent 9 of 10 days in ICU receiving oxygen via high-flow nasal cannula at 40 l/min throughout his stay and oxygen concentration between 70% and 80% during the initial 7 days decreasing to 40% for the last 2 days. His work of breathing averaged 3 (range 2-4) during the first 6 days improving gradually to an average of 2.5 (range 2-3) toward the end of his ICU stay without appreciable change in the chest X-ray. He was discharged from ICU once he was able to oxygenate adequately receiving oxygen through a simple nasal cannula without significant increase in the work of breathing at rest. View Figure 2
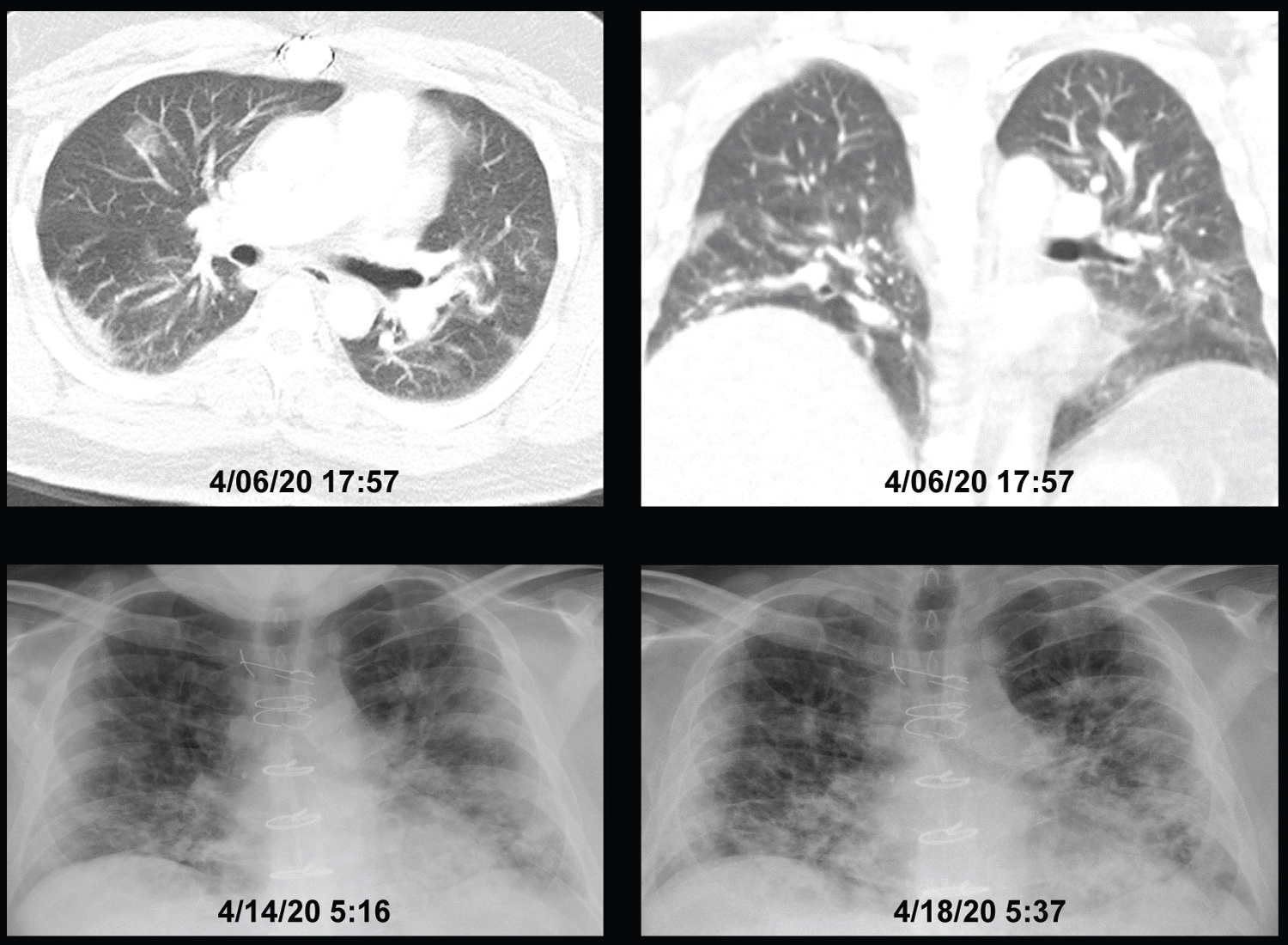 Figure 3: Patient #3, showing a CT of the chest 4 days before ICU admission and chest X-rays on ICU days 4 and 8. The patient spent 7 of 8 days in ICU receiving oxygen via high-flow nasal cannula between 50 l/min and 60 l/min and oxygen concentration between 50% and 65% during the initial 5 days and 50% for the last 2 days. His work of breathing averaged 3.5 (range 3-5) during the first 4 days improving gradually to an average of 2.5 (range 1-3) toward the end of his ICU stay without appreciable change in the chest X-ray. He was discharged from ICU once he was able to oxygenate adequately receiving oxygen through a simple nasal cannula without significant WOB increase at rest. View Figure 3
Figure 3: Patient #3, showing a CT of the chest 4 days before ICU admission and chest X-rays on ICU days 4 and 8. The patient spent 7 of 8 days in ICU receiving oxygen via high-flow nasal cannula between 50 l/min and 60 l/min and oxygen concentration between 50% and 65% during the initial 5 days and 50% for the last 2 days. His work of breathing averaged 3.5 (range 3-5) during the first 4 days improving gradually to an average of 2.5 (range 1-3) toward the end of his ICU stay without appreciable change in the chest X-ray. He was discharged from ICU once he was able to oxygenate adequately receiving oxygen through a simple nasal cannula without significant WOB increase at rest. View Figure 3
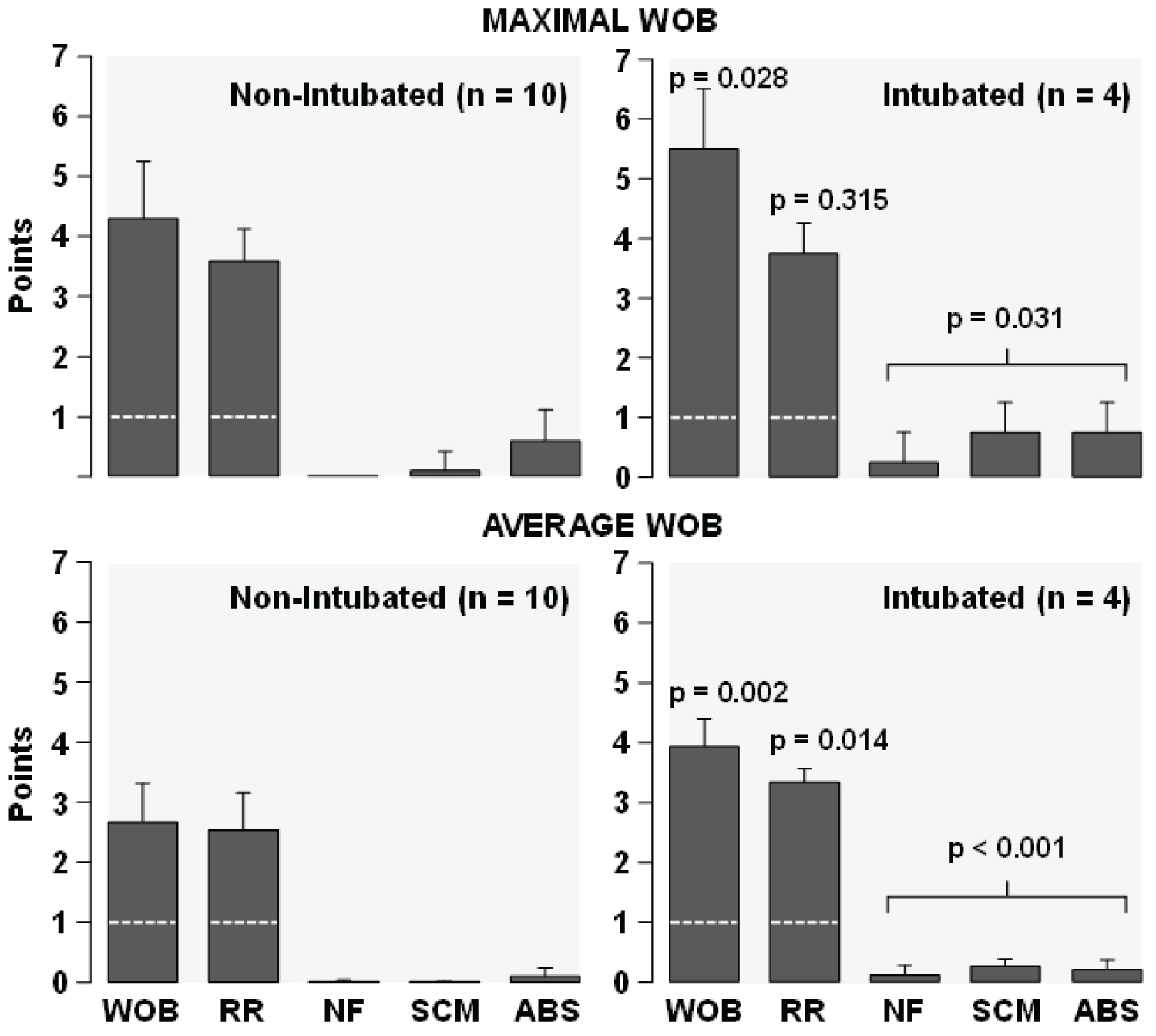 Figure 4: Maximal and average work of breathing (WOB) measured during the ICU stay in 10 patients who did not required intubation and in 4 patients who needed intubation. In non-intubated patients, the maximal and the average WOB refer to values measured through the entire ICU stay. In intubated patients, the maximal and the average WOB refer to values measured during the 24 hours preceding intubation. The discontinued line shown on the WOB scale and the respiratory rate (RR) bars represent the normal values resulting from a normal respiratory rate of 20 breath per minute or less without use of respiratory accessory muscles.
Figure 4: Maximal and average work of breathing (WOB) measured during the ICU stay in 10 patients who did not required intubation and in 4 patients who needed intubation. In non-intubated patients, the maximal and the average WOB refer to values measured through the entire ICU stay. In intubated patients, the maximal and the average WOB refer to values measured during the 24 hours preceding intubation. The discontinued line shown on the WOB scale and the respiratory rate (RR) bars represent the normal values resulting from a normal respiratory rate of 20 breath per minute or less without use of respiratory accessory muscles.
NF: Nasal Flaring; SCM: Sternocleidomastoid Muscle; ABS: Abdominal Muscles. Shown are means ± SD. The p-values indicate comparison between intubated and non-intubated patients for the WOB, the RR, and the aggregate points of NF, SCM, and ABS by one-tailed t-test.
View Figure 4
Table 1: Clinical features of 10 patients with COVID-19 pneumonia treated in our ICU without intubation for mechanical ventilation. View Table 1
Recent clinical observations have shown that COVID-19 pneumonia presents in most patients, at least early on, with scattered areas of lung involvement displaying ground glass opacities dispersed within apparently healthy lungs. This pattern is accompanied by hypoxemia and tachypnea but with relatively minor reductions in lung compliance and therefore relatively minor increases in WOB not initially requiring invasive mechanical ventilation [7,8]. Hypoxemia is presumed to result from vasoplegia in the affected lung areas precluding hypoxic vasoconstriction and therefore increasing venous admixture [7].
The main reasons for intubation in patients with COVID-19 pneumonia once adequate arterial oxygenation is established is worsening lung compliance prompting WOB increase with two deleterious effects. First, respiratory muscle fatigue progressing to hypoventilation and hypoxemic cardiac arrest. Second, ventilation with increased transpulmonary pressure causes lung stress, which has been suspected as a mechanism for patient self-inflicted lung injury (P-SILI) [10]. Mechanical ventilation can alleviate these two deleterious effects, first by providing needed respiratory muscle support and second by enabling lung recruitment using PEEP and selection of optimal tidal volumes to reduce the transpulmonary pressure fluctuation minimizing additional lung injury.
The clinical challenge is to identify the risk of developing these two conditions and act promptly without delaying intubation. Experts have pointed to measurements of intrathoracic pressure fluctuation between inspiration and expiration using an esophageal balloon to recognize increased WOB and increased transpulmonary pressures [7,8]. With this approach, initiation of mechanical ventilation is suggested when the intrathoracic pressure fluctuation exceeds 15 cmH2O [11]. However, placing an esophageal balloon in the non-instrumented and awake patients is not a practical option, especially outside the intensive care unit and for extended periods. Under these constraints, Gattinoni, et al. recommended careful clinical assessment of respiratory drive and inspiratory efforts and to strongly consider intubation if signs of respiratory distress are present to avoid or limit transition to P-SILI [12]. Accordingly, an approach to monitor WOB at the bedside would be helpful to identify patients who are likely to benefit from mechanical ventilation.
The WOB scale that we developed ranks WOB from 1 (normal at rest) to 7 (maximal) as shown in Figure 1. We confirmed that our WOB scale is easy to teach, and its use is associated with high interrater agreement [13]. More recently, we developed a reflex WOB in which the assessment of respiratory accessory muscles is prompted only if the respiratory rate exceeds 20 bpm [14].
As shown in Figure 4, the maximal WOB level at rest in our patients during their ICU stay averaged 4.3 ± 0.9 pts. Its main contributor was the respiratory rate (3.6 ± 0.5 pts) with relatively infrequent use of respiratory accessory muscles. In contrast, the maximal WOB level within the 24 hours preceding intubation in the four additional patients who required mechanical ventilation was 5.5 ± 1.0 pts. The respiratory rate component (3.8 ± 0.5 pts) was similar as in non-intubated patients but the use of respiratory accessory muscles was significantly higher. Accordingly, in our patients with COVID-19 pneumonia who did not require intubation, the WOB increase stemmed predominantly from tachypnea with only minimal use of respiratory accessory muscles. Our data illustrates a pattern in which the initial response to COVID-19 lung injury is tachypnea without or with only transient use of respiratory accessory muscles. This condition, provided adequate oxygenation can be maintained, can be sustained for long periods of time without need to escalate. However, as the lung injury progresses, increased respiratory rate does not suffice and recruitment of respiratory accessory muscle occurs. When this response is sustained over time (e.g., hours not days) despite noninvasive means to support WOB, intubation for mechanical ventilation becomes necessary. Our WOB scale becomes a useful tool to assist in the decision when to intubate.
A concern when treating COVID-19 patients is the generation of aerosols and potential disease transmission to healthcare workers, especially at the time of intubation or when noninvasive supportive means are used. The previous SARS-CoV outbreak showed the highest risk during intubation and extubation when personal protective equipment (PPE) was not appropriately used [15]. Noninvasive mechanical ventilation has also been associated with aerosol generation, but studies have not provided clear evidence of increased disease transmission to healthcare workers [16]. Use of HFNC has also created concerns, but there is no evidence of increased risk of transmission compared to other means of oxygen delivery [17].
The experience learned from a small case series is difficult to generalize to a larger patient population. We also acknowledge that our WOB scale is grounded on respiratory physiology but without direct WOB measurements. Yet, the experience gained in COVID-19 pneumonia patients suggests that levels of 4 and higher despite use of non-invasive interventions could be used to assess need of intubation for mechanical ventilation. Further refinement on the interventions recommended based on specific WOB level and other modifying factors are awaited.
Successfully securing adequate arterial oxygen oxygenation without having to intubate for mechanical ventilation is advantageous and likely associated with favorable outcomes as our case series suggests. Use of non-invasive mechanical ventilation or HFNC is less resource intense and enables the management of a larger number of patients by the same healthcare team. Thus, once the oxygen requirements are met, we recommend routine and systematic WOB assessment upon presentation and throughout the clinical course to recognize the need for invasive mechanical ventilation and correspondingly plan for orderly nonemergent intubations.
None.
None.
None.