Renal cell carcinoma (RCC) associated with Xp11.2 translocation/TFE3 gene fusion (Xp11.2 RCC) is a rare subtype of RCC which is delineated as a distinct entity in the 2004 World Health Organization renal tumor classification.
To highlight a rare case, with few publications on the topic, in addition to providing scientific explanations about it.
This is a case report of a 58-year-old white male with the diagnosis of renal clear cell carcinoma (RCC). The immunohistochemistry was performed and showed positivity for anti-CD10, vimentine and antibody TFE-3, corresponded to Xp11.2 RCC. For the case report writing we performed a Fluorescence in situ hybridization (FISH) that was negative for the diagnosis of Xp11.2 RCC.
Since the translocations lead to over expression of the TFE3 protein, immunohistochemical staining for TFE3 is widely used as a surrogate marker for the Xp11.2 translocations. However, recent studies have found that the positive predictive value of positive TFE3 staining for Xp11.2 RCC is very low as well as highly false positive results.
It's recently know that TFE3 is an immunohistochemical marker of metastasis and poor survival. That fact it's an important explanation of the prognosis and findings of our case report and others published wrongly as Xp11.2 translocations. With this article we intend to bring that into evidence.
Translocation, Genetic, Carcinoma, Renal cell, In situ hybridization, Neoplasms
Renal cell carcinoma (RCC) associated with Xp11.2 translocation/TFE3 gene fusion (Xp11.2 RCC) is a rare subtype of RCC which is delineated as a distinct entity in the 2004 World Health Organization renal tumor classification. Its morphology and clinical manifestations often overlap with those of conventional RCCs [1]. Children are more affected by this subtype than adults, accounts for 20-40% of pediatric RCC and 1-1.6% of RCC in adults [2]. The exact incidence of TFE3 translocation renal cell carcinoma among adults remains debatable but estimates range from 1 to 4% of all renal cell carcinoma, with approximately 2500 new cases diagnosed every year [3-5].
A subset of patients might also develop translocation renal cell carcinoma after chemotherapy and/or treatment for neuroblastoma [6]. Although chemotherapeutic agents have varying mechanisms of action, most cytotoxic agents cause DNA damage that might consequently initiate a repair process that in turn could facilitate a chromosomal translocation [1,2]. In adults, TFE3 translocation renal cell carcinoma is an aggressive tumor with overall survival similar to that of clear cell renal cell carcinoma [4,7,8]. The incidence of TFE3 RCC is higher in children than in adults; its prognosis is also better in children [1,9].
Clinically, patients with Xp11.2 translocation RCC are typically admitted to the hospital because of hematuresis, abdominal pain, or an abdominal mass, and the presence of occupying lesions is confirmed using radiography, kidney color doppler ultrasonography, and CT. As this presentation is similar to that of common adult RCC subtypes such as conventional clear cell RCC and papillary RCC (PRCC), the frequency of Xp11.2 translocation RCCs in adults may be underestimated. One single-institution study subjected 433 adult patients to cytogenetics and TFE3 immunohistochemical analyses and found that Xp11.2 translocation RCCs accounted for 1.6% of the cases [10]. With that in view Xp11.2 translocation RCC should be considered when tumors exhibit a suspicious pattern [11]. But as shown by a systematic review and meta-analysis of observational studies, no significant differences were observed in the prognosis between children and adults, and between female and male [12] (Figure 1 and Figure 2).
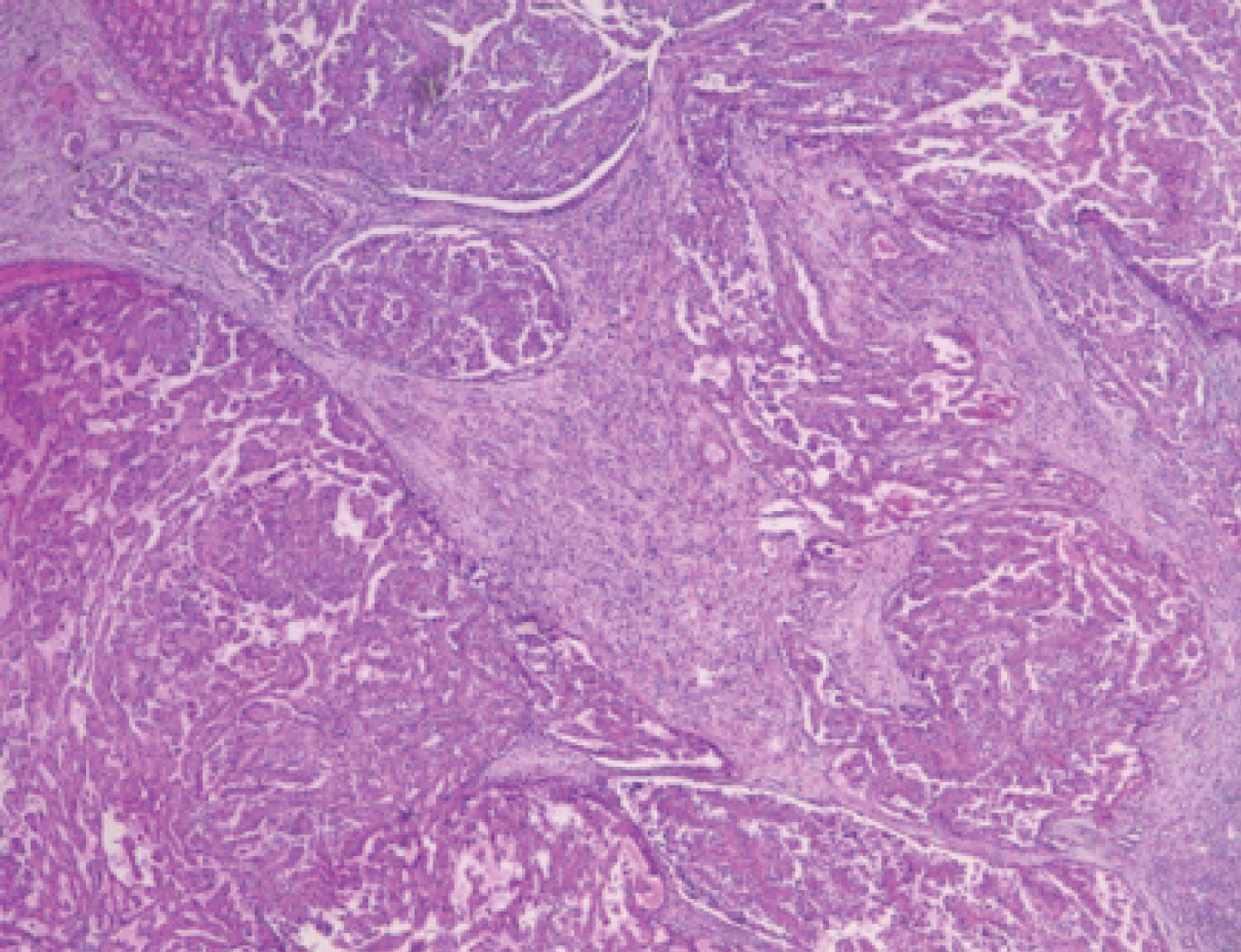 Figure 1: Microscopic appearance of renal cell carcinoma (RCC) with typical papillary architecture.
View Figure 1
Figure 1: Microscopic appearance of renal cell carcinoma (RCC) with typical papillary architecture.
View Figure 1
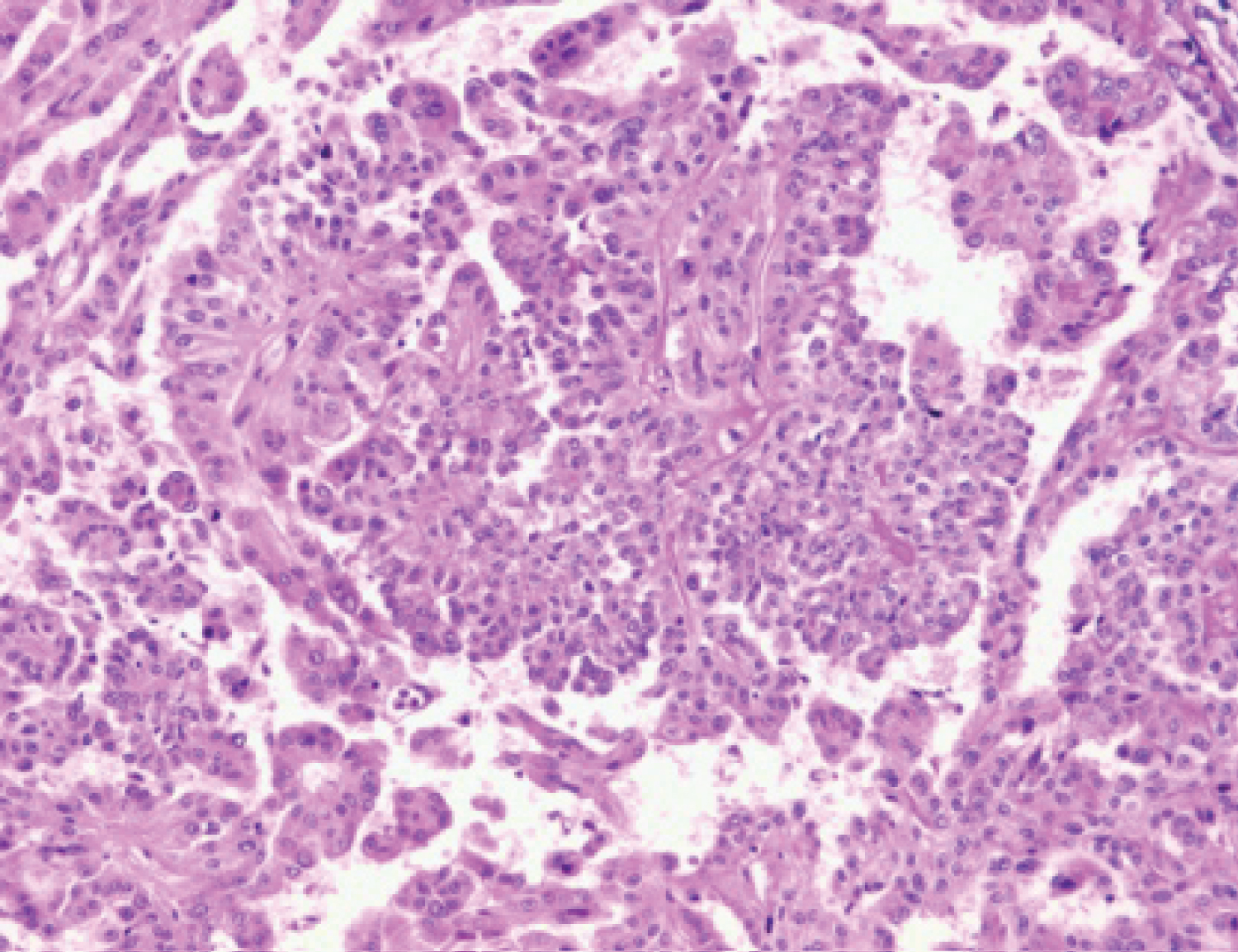 Figure 2: Microscopic appearance of renal cell carcinoma (RCC) with typical papillary architecture.
View Figure 2
Figure 2: Microscopic appearance of renal cell carcinoma (RCC) with typical papillary architecture.
View Figure 2
This is a case report of a 58-year-old white male, previously healthy, which presented hematuria. The macroscopy search, product of left nephrectomy, revealed a renal mass of 9.5 × 6.0 × 5.0 cm located on the middle third of the kidney with dissemination for the renal cortex and peri-renal fat and renal sinus. With a total of 60% of necrosis area. As a microscopy find analysis by immunohystochemistry was seen a micropapilar pattern characterized as stage 3 Fuhrman nuclear, in addiction a positivity for anti-CD10, vimentine and antibody TFE-3, corresponded to Xp11.2 RCC. The results came to a diagnosis conclusion of renal clear cell carcinoma (RCC) with lymphnode metastasis, established as pT3N1MX. Three months later, the patient followed with dyspnea, in consequence a pleural biopsy was made and revealed malignant neoplasm confirmed as RCC metastasis. The patient passed away follow seven days, after presenting signs of ascites due to peritoneal carcinomatosis. For the case report writing it was performed Fluorescence in situ hybridization (FISH) that concluded negative for the diagnosis of Xp11.2 RCC (Figure 3).
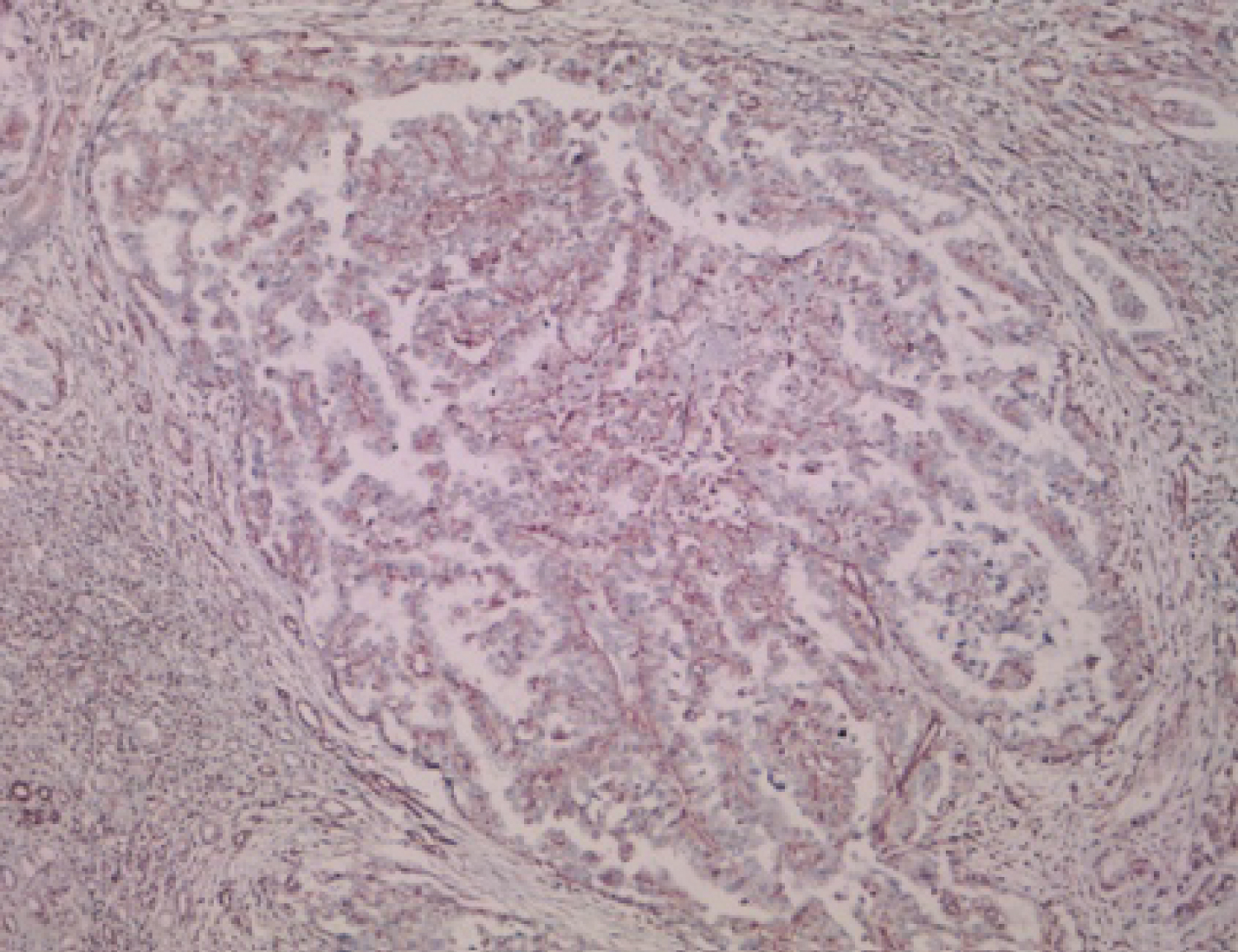 Figure 3: Immunohistochemistry shows immunopositivity for anti-CD10, vimentine and antibody TFE-3.
View Figure 3
Figure 3: Immunohistochemistry shows immunopositivity for anti-CD10, vimentine and antibody TFE-3.
View Figure 3
Xp11.2 RCC is a rare subtype of RCC which results from gene fusions between the transcription factor E3 (TFE3) gene and at least 5 fusion partners including ASPL-TFE3, PRCC-TFE3, PSF-TFE3, CLTC-TFE3, and Nono -TFE3 [13,14]. Due to the translocations lead to overexpression of TFE3 protein, detection of TFE3 protein by IHC assay is currently the most commonly used diagnostic technique in clinical practice [10]. Gaillot-Durand, et al. showed that nuclei stained with an intensity of ++ to +++ in IHC assay was necessary to suspect the diagnosis of Xp11.2 RCC [15]. However, recent studies have found that the positive predictive value of positive TFE3 staining for Xp11.2 RCC is very low as well as highly false positive results [16]. In that way, definite diagnosis of Xp11.2 RCC should be not only made by IHC assay but also by such strict criteria as FISH assay and other molecular biology [16].
So it's know that Xp11 translocation renal cell carcinoma is cytogenetically characterized by chromosomal translocations involving breakpoints in the TFE3 gene, which maps to the Xp11.2 locus. Histologically, a wide spectrum of morphology has been described in these tumors, emphasizing the need to consider these carcinomas in the differential diagnosis of unusual renal cell carcinomas occurring in either children or adults [3]. Strong nuclear TFE3 immunohistochemical expression is a reasonably sensitive and specific marker for Xp11 translocation renal cell carcinoma [17]. However, fluorescence in situ hybridization (FISH) assays have been demonstrated to be more reliable [18].
The gross features of Xp11.2 translocation RCC are similar to those of conventional clear cell RCC. Macroscopically, the cut surfaces of the tumors are greyish-yellow in color and exhibit hemorrhaging and necrosis. Morphologically, the tumors comprise a combination of nested and papillary structures with clear-to-granular eosinophilic cytoplasm [11]. In contrast, the different subtypes of Xp11.2 translocation RCC are histopathologically distinct. Typically, cells of the alveolar soft part sarcoma chromosome region (ASPSCR)-TFE3 subtype are characterized by a higher amount of clear-to-eosinophilic cytoplasm relative to the other subtypes, and exhibit discontinuous cell boundaries, vesicular nuclei, and obvious nucleoli. In contrast, the typical features of PRCC-TFE3 Xp11.2 translocation RCC include a diminished cytoplasm, fewer psammoma bodies and hyaline globules, and a more nested structure [19].
Because of the rarity of Xp11.2 translocation RCCs, the prognosis and outcome in these patients are not fully understood. In addition, for the same reasons, there is currently no standard treatment strategy for this malignancy [20]. In contrast to conventional RCC, the appropriate treatment strategies for Xp11 translocation RCC remain unclear, because the natural course of this tumor is not yet fully understood. However, there is a general agreement that Xp11 translocation RCC is associated with a high malignant potential and poor prognosis [21]. The treatment results of patients with Xp11 translocation RCCs have been previously reported [22-24]. However, although various treatments have been applied, no effective treatment has yet been established. In short, adequate prolongation of survival by cytotoxic chemotherapy, radiation, and/or immunotherapy has never been accomplished. Moreover, there is one previous report of over expression of phosphorylated S6, a marker of elevated mammalian target of rapamycin (mTOR) pathway activation, and increased levels of stable HIF1α in Xp11.2 translocation RCC [25]. Furthermore, Xp11.2 translocation/TFE3 gene fusion has been reported to up regulate the mesenchymal-epithelial transition tyrosine kinase receptor, consequently leading to the activation of the phosphatidylinositol-3 kinase and mTOR pathways [26,27]. Considering these reports, it has been suggested that mTOR inhibitors may be effective for Xp11.2 translocation RCC. Moreover, it has been speculated that targeted agents such as sunitinib, sorafenib, and everolimus may be effective and improve progression-free survival for Xp11.2 translocation/TFE3 gene fusion RCC [28]. However, more detailed information regarding treatment strategies are necessary [27]. Furthermore, based on the specific pathological pathways involved in Xp11.2/TFE3 gene fusion, elaborate treatment strategies should be developed to improve the prognosis of these patients, owing to their molecular and genetic heterogeneity [21].
We declare no financial support and no material support.
All authors declare that there are no conflicts of interest. All authors had an equally contribution.