Background: Malignant Ovarian Germ Cell Tumors (MOGCT) are rare and frequently occur in the young reproductive age and the oncologic and reproductive outcome after Fertility-Sparing Surgery (FSS) this disease is still limited.
Objective: To evaluate the oncology and reproductive outcome of MOGCT who underwent FSS.
Method: All MOGCT who underwent FSS defined as the operation with a preserved uterus and at least one side of the ovary at our institute between January 2005 and December 2020 were retrospective reviews.
Results: Sixty-two patients were recruited in this study. The median age was 22-year-old and over 77% were nulliparity. The three most common histology findings were immature teratoma (32.2%), dysgerminoma (24.2%), and yolk sac tumor (24.2%). The distribution of stage was as follows; stage I = 74.8%, stage II = 9.7%, stage III = 11.3% and stage IV = 4.8%. Forty-three (67.7%) patients received adjuvant chemotherapy. With a median follow-up time of 96.3 months, the ten-year progression-free survival and overall survival were 82.4% and 91%, respectively. For reproductive outcomes, 43 patients who received adjuvant chemotherapy, 18 (41.9%) had normal menstruation, and 17 cases (39.5%) resumed menstruation with a median time of four months. About 14 patients who desired to conceive, four cases were pregnant and delivered good outcomes. Only one case was aborted. Therefore, the successful pregnancy rate was 28.6%.
Conclusion: The oncology and reproductive outcome of MOGCT treated with FSS were excellent. Many patients showed a long survival time with normal menstruation. However, the obstetric outcome was not quite high.
Malignant ovarian germ cell tumor, Fertility-sparing surgery, Oncology outcome, Reproductive outcome, Pregnancy rate, Survival rate
Malignant Ovarian Germ Cell Tumors (MOGCT) occurred about 5% of all ovarian cancer and approximately 70% develop in young women [1]. With the introduction of chemotherapy consisting of Bleomycin, Etoposide, and Cisplatin (BEP) for MOGCT treatment after surgery, the outcome of this malignancy is excellent even in the advanced stage [2]. The cure rate of MOGCT in the early-stage and advanced stage was 100% and 75%, respectively [3]. Therefore, in patients who were of young and reproductive age, the role of Fertility-Sparing Surgery (FSS) defined as cytoreductive surgery with preservation of contralateral adnexa and uterus is the standard treatment for these patients [4]. We previously reported a ten-year overall survival rate as high as 86.2% but did not focus on the patients who underwent FSS [5]. Therefore, with the limited data of oncology and reproductive outcomes of FSS especially in Southeast Asia, this study was conducted to identify these outcomes of MOGCT patients who were treated with FSS.
After the protocol was approved by the local ethics committees, the medical records of the MOGCT patients who underwent FSS defined as surgical cytoreduction with preservation of the uterus and unilateral adnexa at Chiang Mai University Hospital from January 2005 through December 2020 were reviewed. The patients who developed other histologic types arising in germ cell tumors were excluded. The basic clinical data, histology, staging, type of surgery, chemotherapy regimen, and outcomes were identified. All pathology specimens were examined by gynecologic pathologists in our institute. The decision of treatment depended on the preference of the physicians.
After complete treatment, the surveillance schedule was set every three months in the first year, every four months in the second year, and every six months in the third to fifth year, then annually. At that time, all of the patients were examined for a blood test for tumors of MOGCT and were examined by gynecologic oncologists. Pelvic ultrasonography was done at each visit for unmarried patients. Other imaging such as CT-scan was utilized when clinically indicated or with a rising of tumor markers.
The Progression-Free Survival (PFS) was defined as the time between the month of the primary surgery and the month of tumor progression or recurrence detection or last contact whereas the overall (OS) was defined as the similar starting time of PFS to the month of patient death or last contact. The death data was also sought from the Thai Civil registration system via the National identification card number. Both PFS and OS were estimated by the Kaplan-Meier method using the SPSS for Windows program (Version 22; IBM Corporation, Armonk, New York, USA). Descriptive data of all studied patients were presented as means with range and discrete data were reported as numbers and percentages.
The reproductive outcome after FSS were identified by collecting the data of the menstrual status during and after treatment, the number of pregnancies and childbirth before and after treatment, the present marital status, the childbearing desire, the method of pregnancy, gestational age at delivery, birth weight of the baby and obstetrical complications from the medical records and direct contact with the patients by phone for more information.
Among 98 MOGCT, 62 patients underwent FSS in the studied period. The clinical data were presented in Table 1. The median age of these patients was 22 with a range of 4-34years old. Over 77% of them were nulliparity and the three most common presentations were pelvic mass, abdominal pain, and abdominal distension. The tumor side was located on the right side about 54.8% and on the left side was 41.9%.
Table 1: Clinical Data (N = 62). View Table 1
The detail of FSS was as followed; unilateral Salpingo-Oophorectomy (SO) in 49 cases, unilateral ovarian cystectomy in four cases, and unilateral SO with contralateral ovarian cystectomy in the rest. The frozen section was done in 26 cases. About staging procedures, the peritoneal cytology was done in 39 cases with ten cases revealing positive malignancy cells while the omentectomy was done in 44 cases with positive in four cases and lymphadenectomy was performed in 30 cases with positive in four cases. Half of the studied patients underwent an appendectomy. Regarding the surgical outcomes, 75.8% was complete resection.
The three leading histology were immature teratoma (32.3%), dysgerminoma (24.2%), and yolk sac tumor (24.2%). The majority of the patients were in stage I (74.2%) and about 4.8% were in stage IV. Nearly 70% of the patients were given adjuvant chemotherapy. All except one was bleomycin + etoposide + cisplatin (BEP) regimen. Onlyone case was given etoposide+methotrexate+actinomycin D+cyclophosphamide+vincristine (EMACO). This case was diagnosed with stage IV choriocarcinoma. About one-third of the patients received four to six cycles of chemotherapy. Concerning the long-term side effect of chemotherapy, numbness occurred in three cases, lung fibrosis occurred intwo cases, and hearing problems in two cases. Five patients died. Two cases died from neutropenic sepsis and the rest from the progression of the disease.
With the median follow-up time of 96.3 months, the ten-year PFS and OS were 82.4% and 91% as shown in Figure 1 and Figure 2, respectively. However, 62.9% did not continue regular follow-up.
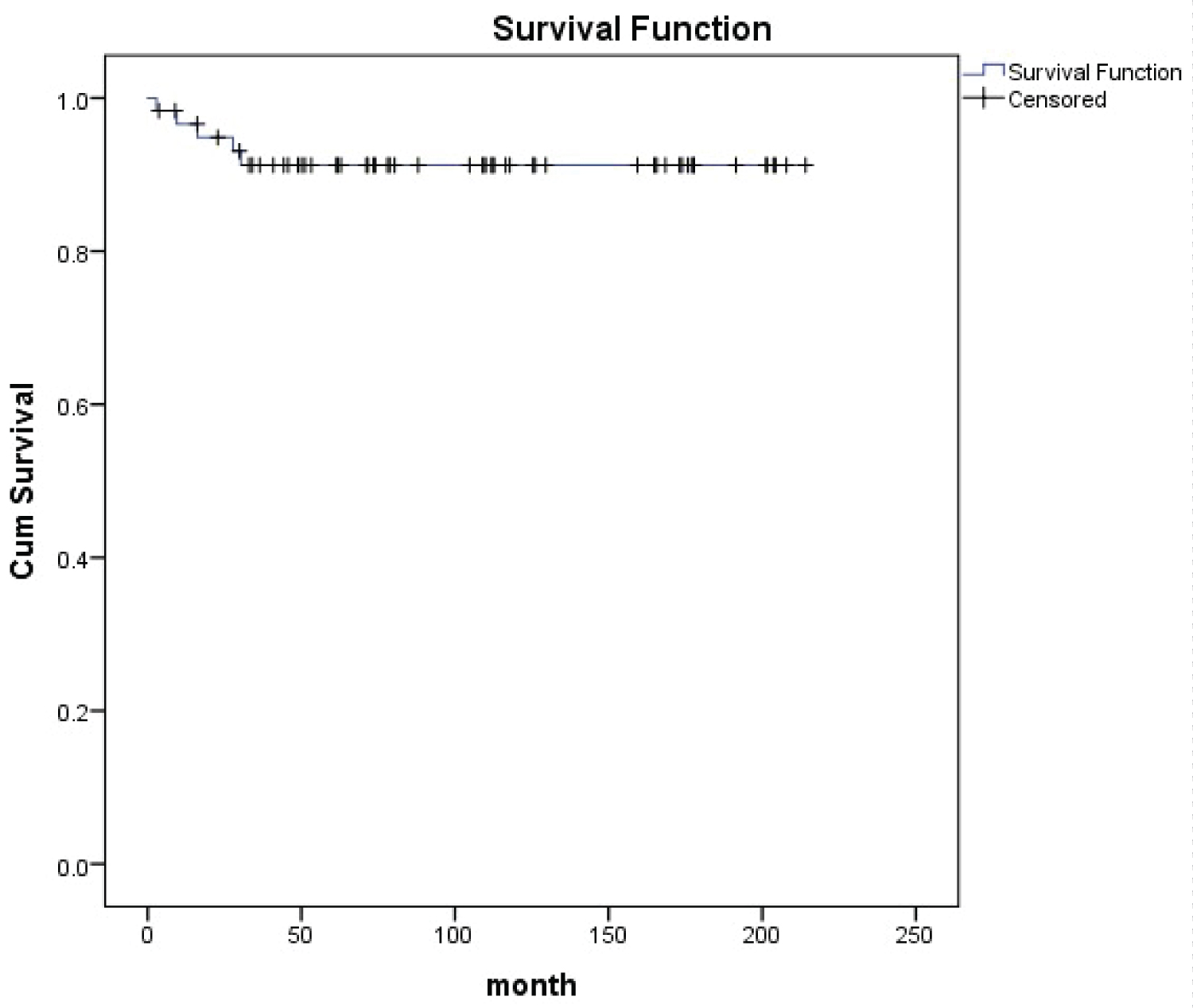 Figure 1: Overall Survival (OS).
Figure 1: Overall Survival (OS).
5 years OS = 91.2%
10years OS = 91%
Median follow uptime 96.38 months (3-214 months)
View Figure 1
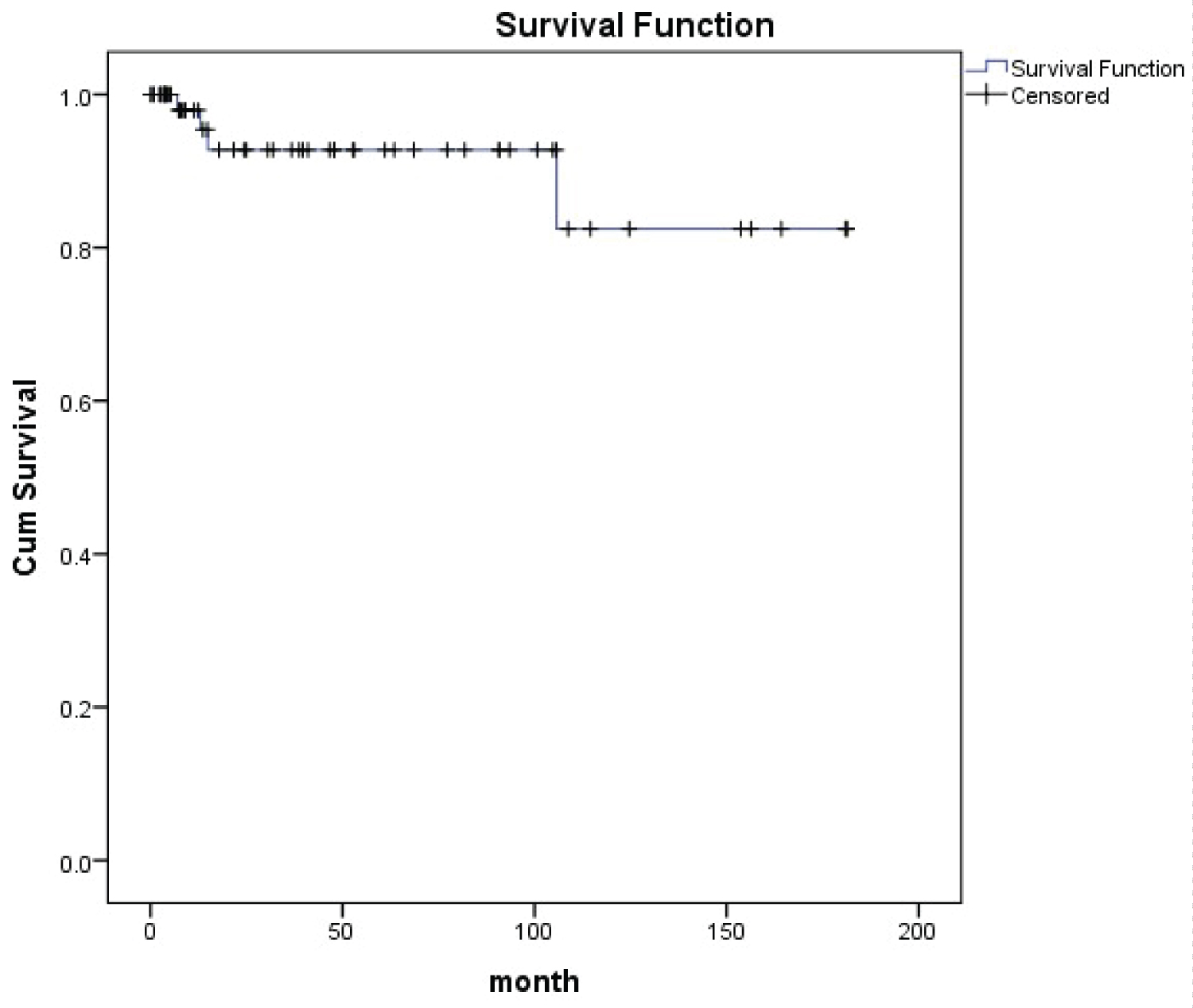 Figure 2: Progression Free Survival (PFS).
Figure 2: Progression Free Survival (PFS).
5 years PFS 92.8%
10 year PFS = 82.4%
Median follow up time 27.78 months (1-181 months)
View Figure 2
Four cases developed progression after primary FSS. The details of these patients was summarized in Table 2. One of them lived while the others died from the disease progression during treatment. This survived case was 17-year old stage IC1 grade 2 immature teratoma. The primary surgery was right SO and appendectomy with pelvic recurrence after operation for three months. She underwent tumor debulking and received six cycles of BEP regimen. She is still alive without disease with an overall survival of 109 months. The other three cases were stage IV. The histology was a yolk sac tumor in two cases with the remainder of choriocarcinoma. All of them underwent FSS and received multiple chemotherapy regimens with unfavorable outcomes and died of disease after primary surgery at 16,28, and 30 months. One case developed lung fibrosis after being administered two cycles of BEP regimen.
Table 2: Progression Cases (N = 4). View Table 2
Regarding 4 patients who underwent only a cystectomy. The pathology was immature teratoma in two cases (stage IA grade 2 and IC grade1), papillary thyroid cancer arising from mature teratoma (1), carcinoid tumor (1). Only one case of stage IA grade 2 immature teratoma received four cycles of BEP regimen while the other received only an operation. All of them are still alive at present with overall survival of 44-173 months.
Of 62 patients, 43 patients were received adjuvant chemotherapy with BEP in 41 cases and EMACO in the rest. The menstrual history of these patients was summarized in Table 3. About 42% of them had menstruation while receiving chemotherapy while 39.5% resumed menstruation after complete treatment with a median resumption time of four months. One case was five years old at the treatment time with menarche at age 12 (seven years later).
Table 3: Menstrual Data of Studied Patients Who Received Chemotherapy (N = 43). View Table 3
Eight patients were without menstruation after chemotherapy. The one case without menarche at presentation was 12 years old. She was diagnosed with stage I mixed MOGCT and received six cycles of BEP regimen after undergoing right SO at five years of age. She was followed regularly with no evidence of recurrence. The remaining seven patients developed premature menopause. One case was diagnosed as stage IIA endodermal sinus tumor at 29 years old. She received six cycles of BEP regimen after undergoing right SO and omentectomy on January 1, 2017. One year after that, she developed a left ovarian tumor 10x15 cm and carried out hysterectomy with left SO. The final pathology revealed rade 1 endometrioid CA. The patient was given six cycles of carboplatin with a disease-free survival of 61 months and received estradiol valerate 2 mg as hormonal therapy. The other two patients underwent FSS and received three and six cycles of BEP, respectively. Both cases did not resume menstruation after completing treatment.One case received hormonal therapy. However, both cases were followed up only one year after FSS. Four cases died, two from neutropenic sepsis and two cases from disease progression after multiple chemotherapy regimens. The details of these patients was summarized in Table 4.
Table 4: Details of Premature Menopausal Patients (N = 7). View Table 4
Regarding 19 patients who underwent only FSS without adjuvant chemotherapy. One case was lost to follow up since surgery while the remaining 18 cases had no problem with menstruation. One case was diagnosed with stage I immature teratoma and received left SO with omentectomy and appendectomy at four-years-old. At 15-year-old, her menarche occurred.
For pregnancy outcome, the data was available in 30 patients and revealed that 14 cases attempted to become pregnant and four of them (28.6%) succeeded in delivering a term baby after one year for two cases and six years for one case. One patient was known to give one term birth due and unavailable for contact details. Three cases underwent unilateral SO and the rest carried out unilateral ovarian cystectomy. The histology of these four cases was grade 1 carcinoid tumor neuroendocrine tumor (1), dysgerminoma (2), grade 1 immature teratoma (1). Moreover, one case developed a spontaneous abortion two years after treatment and never pregnant again. She was diagnosed with a steroid cell tumor. None of the patients who attempted to conceive actively tried to become pregnant by going to an Infertility Clinic. The details of these patients were noted in Table 5.
Table 5: Pregnancy outcome. View Table 5
The outcome of62 MOGOT patients who were treated with FSS in the present study was excellent with the ten-year PFS and OS being 82.4% and 91%, respectively. This results were close to the previous reports. Zamani, et al. [6] studied 79 MOGCT over 15 years and showed the ten-year OS as 94.4%. This study recruited only S stages I-III while our study recruited all stages including three progressed cases of tage IV. Another study from Korea [1] studied 171 MOGCT who underwent FSS for 23 years (1992-2015). They reported the five-year PFS and OS as 86% and 97%, respectively. About 14.6% developed recurrent disease and the death rate of disease was 2.9%. This recurrence rate was higher than our study which showed progression of disease only in 1.6%. However, due to over two-thirds of our patients without regular follow-up, the actual number of recurrence patients might be missed. However, the death rate of this disease from our study was 4.8% near the Korean report. In addition, Bercow, et al. [7] reviewed eight retrospective studies comparing FSS with the conventional operation for MOGCT patients and found that both types of surgery were not significant for the recurrence.
Regarding ovarian cystectomy in MOGCT, although this operation was not the standard of FSS, Beiner, et al. [8] showed an excellent outcome in eight patients who were diagnosed as early-stage immature teratoma treated with ovarian cystectomy. Five patients received chemotherapy. With a median follow-up time of 4.7 years, all patients were still free of disease. The authors suggested that cystectomy followed by adjuvant chemotherapy showed impressive outcomes for early-stage MOGCT, especially in immature teratoma. For our study, four cases underwent ovarian cystectomy with one case of stage IA grade 2 immature teratoma received adjuvant chemotherapy. All of them were still alive at the duration time of 44-173 months from surgery.
About 70.8% of the patient who had no menstruation during treatment with FSS and chemotherapy in this study were resume the menstruation with a median time of four months. The true premature ovarian failure from chemotherapy occurred in only two cases (3.2%). Both of them underwent unilateral SO with three and six cycles of BEP regimen. Tamauchi, et al. [9] used the Tokai Ovarian Tumor Study Group database on ovarian cancer patients and selected 110 MOGCT patients who received FSS with the median follow-up period of 10.4 years for study. In this Japanese report, 63.9% of the patients received BEP regimen and about 30.6% received cisplatin+vincristine + bleomycin (PVB) regimen. They revealed premature menopause which was close to our study as 2.9%.
Regarding the obstetric outcome, our study reported the rate of term pregnancy was 28.6%. This result was different from a Japanese study [9]. The authors revealed 45 patients attempts to become pregnant with 40 patients succeedingin deliveries with total pregnancies as term deliveries in 54 cases (83.1%), pre term delivery two (3.2%), abortion 12 (18.5%). Seven cases received fertility treatment. A publication from Iran reported that 19 of 26 (73%) MOGCT patients who underwent FSS were successful in delivery without infertility treatment [6]. In addition, Mikus, et al. [10] reported the pregnancy rate in 20 German patients with MOGCT who desired to become pregnant of their series was 50%. The pregnancy rate from previous studies was higher than our study which showed the successful pregnancy rate was only 28.6%. The difference might be from the current trend of Thai culture to have fewer children, the missing data from the patients unable to be contacted, and those non-actively who tried to conceive in our patients.
The strength of our study was the real-world series of patients with MOGCT treated with FSS in a single institute to show the oncology and reproductive outcome. However, with the limitation of retrospective study nature, about two-thirds of the patients were not followed for a long. Therefore, some data were missed.
In conclusion, the oncology and reproductive outcome of MOGCT treated with FSS were good. Many patients showed a long survival time with normal menstruation. However, the obstetric outcome in patients who attempt to conceive was not quite high.
The study was approved by Chiang Mai University Ethic Committees.
7736 Study Code : OBG-2563-07736.
The authors declare no potential conflict of interest.