Type 1 diabetes mellitus (T1DM) in literature has usually been associated with laboratory decrease in pancreatic exocrine enzymes levels. Nevertheless, the exact onset of decreased pancreatic enzymes levels in sera of patients is still unknown. We measured pancreatic serum levels of trypsinogen and lipase in Egyptian children and adolescents with newly diagnosed T1DM to reveal their role in diagnosis and their relation to HbA1c as a marker of glycemic control, lipid profile and fasting c-peptide as a marker of endocrine pancreatic insufficiency.
Fifty Egyptian children with newly diagnosed T1DM were compared to age and sex matched 50 healthy controls. Full clinical history was taken including history of diabetic ketoacidosis (DKA) and that of pancreatitis. All subjects underwent full clinical examination. Anthropometric measurements were taken including weight, height and body mass index. Laboratory data of HbA1c, lipid profile and fasting c-peptide of patients with newly diagnosed T1DM were collected. Serum trypsinogen and serum lipase were collected from both patients' and control groups.
Serum trypsinogen and lipase were significantly decreased in patients with newly diagnosed T1DM compared with control group (p = 0.00028). There was no relation between the pre-mentioned pancreatic enzymes and fasting c-peptide nor with disease duration (p = 0.42).
Almost all children and adolescents with newly diagnosed T1DM had low levels of exocrine pancreatic enzymes. Nevertheless, more studies are needed to follow-up both pancreatic enzyme levels as well as exocrine pancreatic autoantibodies searching for correlations with disease development and progression.
T1DM results from disruption of pancreatic function as a result of autoimmune destruction of pancreatic tissue. The period of development of the autoimmune process and the evidence of overt clinical picture of DM varies greatly and remains unclear [1]. However, as the stage of overt clinical type 1 DM is reached, associated destruction of the exocrine pancreatic cells usually result in decreased serum pancreatic enzymes such as serum trypsinogen and serum lipase [2,3]. Accordingly, measurement of serum concentration of pancreatic trypsinogen and/or lipase can be an early clue for pancreatic disruption. The usage of pancreatic enzyme; serum trypsinogen and lipase levels as a predictive biomarker of type 1 diabetes has been evaluated [2,4]. It is suggested that analysis of pancreatic enzymes in diabetic patients could be an early marker of disease diagnosis as well as being a useful parameter in assessing the progress of illness [1]. To our knowledge, only one study [2] assessed the level of serum trypsinogen in a mixed group of pediatric and adults with T1DM and therefore, the current study assesses the levels of trypsinogen and lipase in the sera of children and adolescents with newly diagnosed T1DM and the results were correlated to demographic data, clinical history/examination, HbA1c and the level of fasting c-peptide.
This pilot Study was conducted on one hundred (100) children and adolescents recruited from Children's Hospitals, Pediatric department, Faculty of Medicine, Ain Shams University Hospitals, Cairo, Egypt. Patients' group included fifty (50) children and adolescents with newly diagnosed T1DM attending the Pediatric and Adolescents Diabetes Clinic, Ain Shams University Hospitals.
Patients diagnosed as T1DM in Diabetes Clinic according to ISPAD diagnostic criteria of diabetes [5]. Also, all patients had low fasting c-peptide levels. All patients included was diagnosed with T1DM within 90 days of data collection. Patients' ages ranged from two to eighteen years. This study did not include patients with type 2 diabetes mellitus nor other types of diabetes. Also, patients with gastrointestinal diseases such as Celiac disease, inflammatory bowel diseases, malabsorption syndromes and GIT infections were not included. The control group included fifty (50) age and sex matched healthy children and adolescents. They were recruited from Outpatient Clinic at Ain Shams University Hospitals.
Written informed consent was taken from the care givers in ages below 16, and from participants in ages equal or more than sixteen. The procedures applied in this study were approved by The Ethical Committee of Human Experimentation of Ain Shams University, and are in accordance with the Helsinki Declaration.
Data collected from all patients in the study included detailed medical history taking with special stress on: Demographic data: Name, age, sex, family history of diabetes, disease duration, history of DKA development, symptoms suggestive of pancreatitis e.g. epigastric pain radiating to the back associated with nausea and vomiting and symptoms of pancreatic insufficiency e.g. offensive bulky stools, weight loss.
All subjects included in the study had a thorough full clinical examination laying stress on: Assessment of anthropometric measures including weight in Kilograms (Kg) and height in centimeters (cm). Body mass index was calculated as Kg/m2 and plotted on the age -and sex-standard percentiles according to WHO growth charts for weight, height and BMI Z scores [6].
Under complete aseptic conditions, 10 mL of fasting venous blood were obtained by a clean venipuncture, two milliliters were placed in EDTA tube for subsequent assay of HbA1c, while the rest was evacuated in two plain test tubes. The serum was separated by centrifugation (1000x g for 15 minutes). Serum of one tube was immediately assayed for lipid profile, while the serum collected in the other tube was divided in three aliquots and stored at -20 ℃ for subsequent assay of fasting C-peptide, serum lipase and trypsinogen. Hemolysed samples were discarded. Repeated freezing and thawing was avoided.
HbA1c was assayed by high performance liquid chromatography (HPLC) technique on the Bio-Rad d-10 hemoglobin testing system (Bio-Rad Laboratories, Inc., 4000 Alfred Nobel Drive, Hercules, California 94547, USA). Serum samples were assayed for lipid profile on the Beckman AU-680 system auto-analyzer (Beckman Coulter, Inc. Diagnostics Division Headquarters 250 South Kraemer Boulevard Brea, California 92821-6232 USA) using reagents supplied by the company. Triglycerides (TG) and total cholesterol were measured on AU680 is based on enzymatic colorimetric method, high density lipoprotein cholesterol (HDL-cholesterol) assay was based on precipitation of low density lipoprotein cholesterol (LDL-cholesterol) and very low density lipoprotein cholesterol (VLDL-cholesterol) and then the cholesterol in the HDL cholesterol fraction which remains in the supernatant is assayed by a timed endpoint method. LDL cholesterol calculated according to "Friedwald equation": LDL-cholesterol = Total cholesterol-(HDL-C+TG/5), provided that serum TG is ≤ 400 mg/dL, samples with TG > 400 mg/dL are diluted according to its concentration.
Serum lipase was assayed by lipase quantitative kinetic assay Kit supplied by Biochemical Enterprise (S.r.l. - via Toselli, 4 - 20127 Milano - Italy). Serum trypsinogen was assayed by commercially available ELISA kit supplied by Bioassay Technology Laboratory (1008 Junjiang Inter. Bldg, 228 Ningguo Rd, Yangpu Dist, Shanghai, China). Fasting serum c-peptide was measured by commercially available Enzyme Linked Immunosorbent Assay (ELISA) kit supplied by R & D Systems (USA & Canada, R&D Systems, Inc. 614 McKinley Place NE, Minneapolis, MN 55413, USA).
All statistical analyses were done using software version IBM SPSS (Statistical Package for the Social Sciences) statistics (Version 25.0, IBM Corp., USA, 2017-2018). Data were expressed descriptively as Mean ± standard deviation (SD) for quantitative parametric data, median and interquartile range (IQR) for quantitative non parametric values and as percent for qualitative data. Comparative statistics were done using Independent Student t test for parametric data and the Mann-Whitney test for non-parametric data. Chi square test was used for comparison between two independent groups as regards the categorized data. Correlation analysis was performed using Pearson's correlation coefficient for parametric data and Spearman′s rank correlation coefficient for non-parametric data. Receiver operator characteristic (ROC) curves were constructed and optimal cut-off values for serum trypsinogen and serum lipase were established by the best sensitivity and specificity where the right angle at the upper left corner is the best diagnostic threshold (cut-off) of the parameter being varied. Odds ratio measures the association between an exposure and an outcome and how many times the risk was present among diseased individuals compared to that among non-diseased ones. In all statistical analyses, P-value < 0.05 was considered significant.
Serum trypsinogen and serum lipase were found to be significantly decreased in our patients (p = 0.00028) Figure 1. None of our patients suffered symptoms of exocrine pancreatic insufficiency. Also, only four of our patients suffered from symptoms suggestive of pancreatitis at the time of diagnosis. Similarly, studies with wider scope showed similar low levels of pancreatic enzymes without clinical symptoms of malabsorption [2,3]. There was no relation between the pre-mentioned pancreatic enzymes and fasting c-peptide nor with disease duration. The Odds ratio for serum trypsinogen and serum lipase in patients with newly diagnosed T1DM showed that decreased serum lipase levels denotes higher risk for development of T1DM than decreased serum trypsinogen shown in Table 1. ROC curve analysis for diagnostic performance of serum trypsinogen and serum lipase in patients with T1DM in Figure 2 revealed that serum trypsinogen and serum lipase cut off value ≤ 40 ng/dl and ≤ 14.9 U/L respectively could differentiate between children with newly diagnosed and those without T1DM with a sensitivity of 96.00% and 69.39% respectively and specificity of 100% for both. The efficacy of trypsinogen and lipase are 98.9% and 90.1%, respectively. Comparison between patients with newly diagnosed T1DM and control group is shown in Table 2; patients' group had lower Z score for weight and BMI than healthy controls (p = 0.026). This can be attributed to the loss of weight which occur due to polyuria and vomiting presenting just before diagnosis due to hyperglycemia, osmotic diuresis and the development of DKA (56% of our patients developed DKA at presentation), but unfortunately weight loss measurements were not accurately available in the DKA presentation history of our patients. Correlation studies in Table 3 between lipid profile and both demographic and laboratory parameters in patients with type 1 diabetes showed significant positive correlation between serum cholesterol and BMI Z score (p = 0.018). Several studies in literature had similar results indicating a strong link between blood levels of lipid profile and BMI Z score which later correlates to increased risk of atherosclerotic cardiovascular diseases [7].
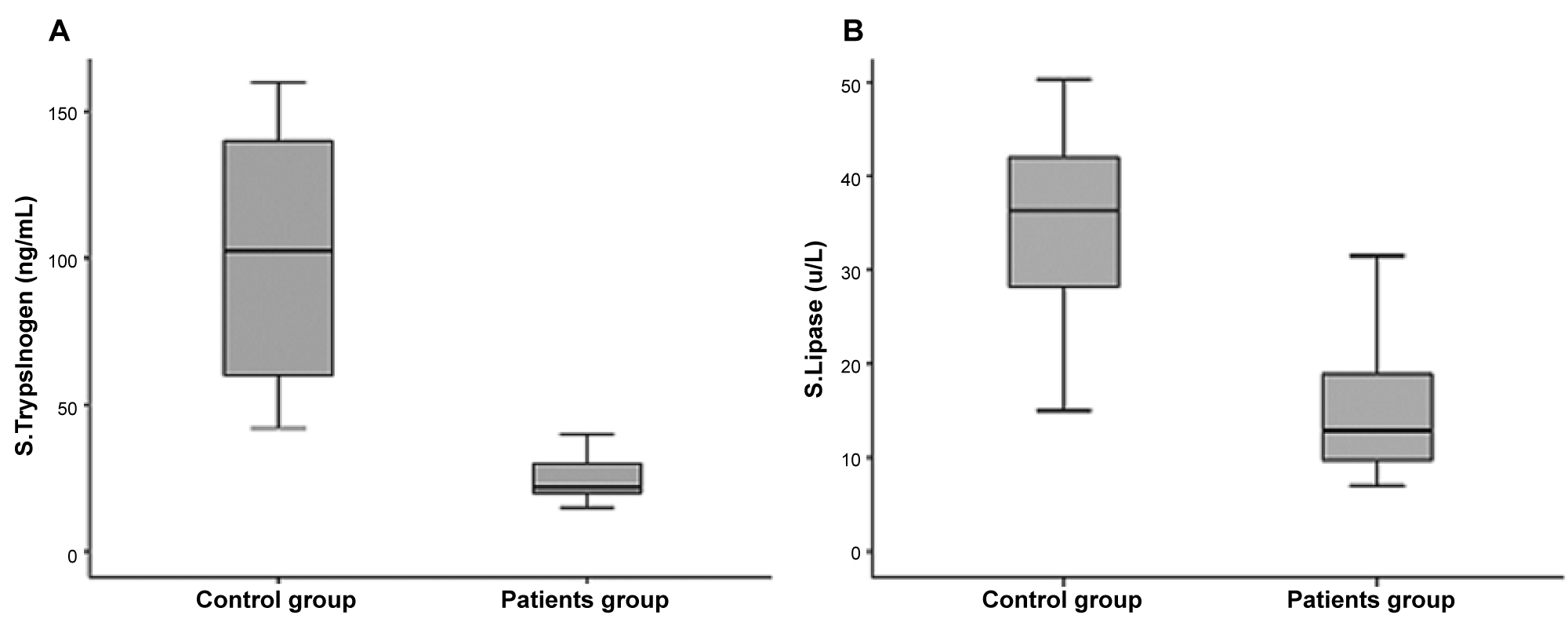 Figure 1: A) Comparison of serum trypsinogen between type 1 diabetic patients and control group; B) Comparison of serum lipase between type 1 diabetic patients and control group.
View Figure 1
Figure 1: A) Comparison of serum trypsinogen between type 1 diabetic patients and control group; B) Comparison of serum lipase between type 1 diabetic patients and control group.
View Figure 1
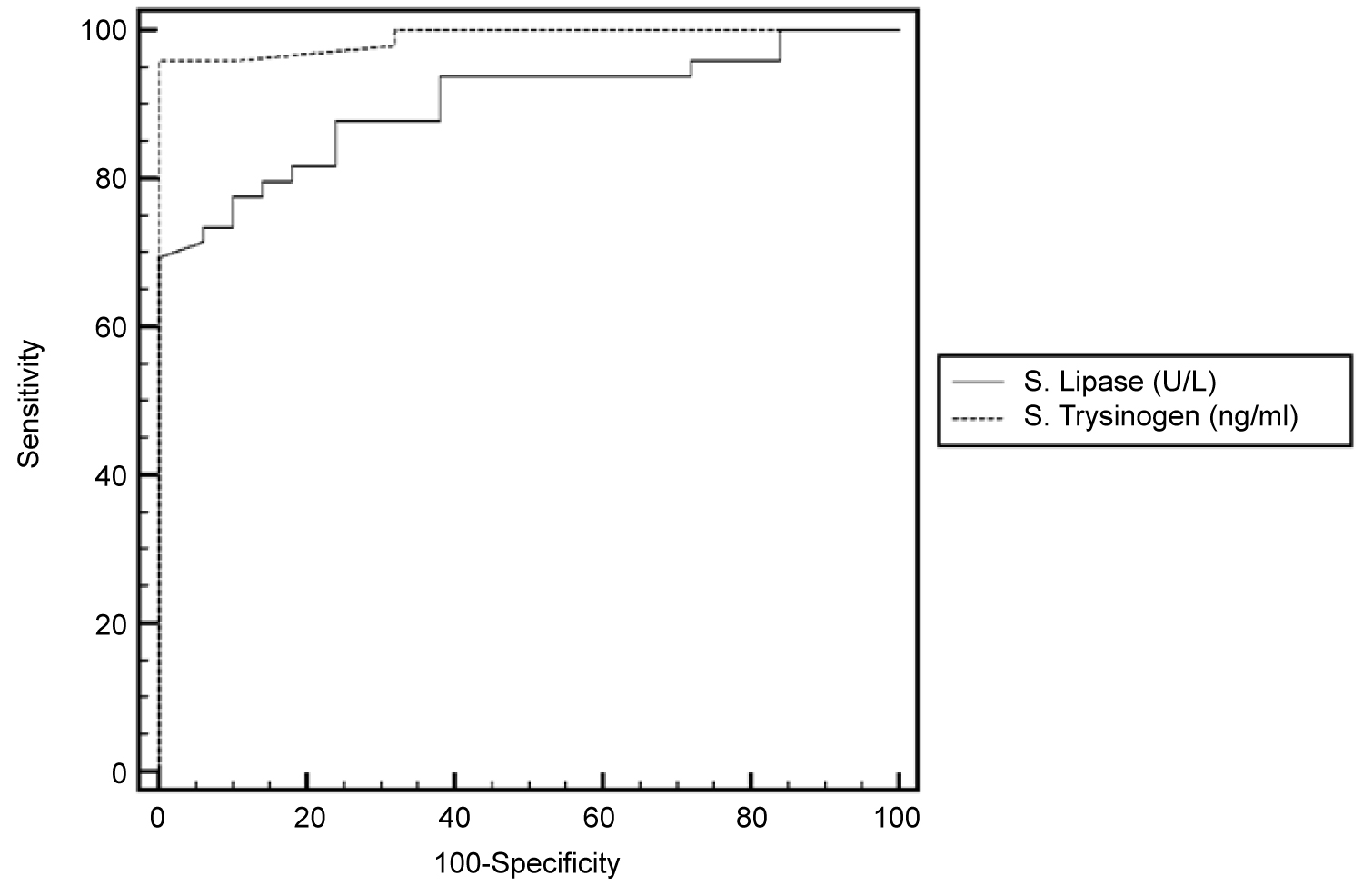 Figure 2: Receiver Operating Characteristic (ROC) curve analysis of serum trypsinogen and serum lipase as a biomarkers in type 1 diabetes.
View Figure 2
Figure 2: Receiver Operating Characteristic (ROC) curve analysis of serum trypsinogen and serum lipase as a biomarkers in type 1 diabetes.
View Figure 2
Table 1: Odds ratio for serum trypsinogen and serum lipase in patients with T1DM. View Table 1
Table 2: Anthropometric characteristics of patients with T1DM compared with control group. View Table 2
Table 3: Correlation between lipid profile and demographic and laboratory parameters in patients with T1DM. View Table 3
The main purpose of our study was assessing pancreatic exocrine enzymes levels by measuring serum trypsinogen and lipase in newly diagnosed children with T1DM and correlating the results with several different parameters. Decreased pancreatic enzymes in newly diagnosed T1DM has been attributed to several reasons; the loss of trophic action of insulin on exocrine pancreatic cells, hyperglycemia leading to osmotic diuresis and renal loss of pancreatic enzymes [8,9] and simultaneous involvement of the pancreatic exocrine tissue in the autoimmune destruction of islet cells [10,11]. Some evidence supports that exocrine pancreatic injury may be a trigger for disease development [12-14]. Bacterial dysbiosis and alteration of the gut microbiome in patients with T1DM is another rising possible trigger for disease development and autoimmunity [15]. No studies were found in literature were able to report when exactly the levels of pancreatic enzymes begin to decrease even in studies which included the presence of pancreatic autoantibodies with or without overt clinical DM [2]. Further studies for follow-up of serum trypsinogen and other exocrine pancreatic enzymes during established disease is also recommended. Nevertheless, applying measurement of pancreatic enzymes for early diagnosis of T1DM can't be validated without ruling out other causes of low levels of pancreatic enzymes such as other causes of pancreatitis, GIT abnormalities and malabsorption disorders.
All authors declare that there is no financial or institutional conflict of interest. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.