Ungual manifestations occurring in patients with end stage renal failure are polymorphic and diverse. The aim of our study was to assess the prevalence and characteristics of different ungual manifestations in patients end stage renal failure.
We led a transverse investigation of all patients with end stage renal failure followed in the department of nephrology of University Hospital Hassan II, during a period of three months from 01 August 2016 to 01 November 2016.
We examined 70 patients (34 men and 36 women). The renal failure duration ranged from 6 months to 13 years. A total of 56/70 (80%) patients had ungual abnormalities. These included absence of lunula, half and half nails, splinter hemorrhages, melanonychia, onycholysis, Beau's lines, koilonychias and Muehrcke lines, onychomycosis, pincer-nail deformity, brittle nails and onychogryphosis, leukonychia, longitudinal ridging, subungual hyperkeratosis, paronychia, nail clubbing. Our results find no significant relationship between the ungual disorders and patient age or duration of renal failure.
Our study found different nail changes in uraemic patients, these abnormalities varied from the most frequent (onycholysis) to rare conditions such as nail clubbing.
Clinical dermatology, End stage renal failure, Nail disorder
Chronic renal failure (CRF) is due to the progressive, usually slow, loss of renal excretory capacity. Diabetes mellitus and arterial hypertension are among the main causes that lead patients to CRF and, consecutively, to dialysis, in addition to other diseases such as systemic lupus erythematosus, amyloidosis, chronic glomerulonephritis and hereditary diseases (polycystic kidneys) [1].
In normal individuals, the glomerular filtration rate is 110 to 120 mL/min, and may fall to 10 or up to 5 mL/min in patients with advanced CRF, when dialytic treatment and renal transplantation may be indicated [1].
CRF affects almost all systems of the body, causing neurological, gastrointestinal, cardiovascular, pulmonary, hematological, endocrine, metabolic and dermatological disorders [1], the latter being caused by renal function itself and the complications inherent in its treatment, leading to xerosis, pruritus, hyperpigmentation, calcinosis, bullous diseases (pseudoporphyria), perforating dermatoses, besides the involvement of the nails [2-4].
There are reports that nail disorders occur in approximately 71.4% of uremic patients, [5] and the most frequent changes are half and half nails, absence of lunula and splinter hemorrhages [6]. Half and half nails are found in up to one-third of the patients, submitted to hemodialysis, being a characteristic feature in these patients [7]. It is characterized by proximal pallor and erythematous-brownish color in the distal portion of the nail plate [6].
The absence of the lunula is characterized by the non-visualization of the visible part of the nail matrix and the splinter hemorrhage appears as filiform longitudinal lines of dark reddish color in the distal region of the nail plate and may also be associated with the antiphospholipid antibody syndrome, bacterial endocarditis, trichinosis, onychomatricoma and external trauma [3,8].
There are several international studies reporting cutaneous and nail changes in chronic dialysis renal patients [6,9-11]. But there is no national publication that reported the prevalence of nail changes in patients with chronic end stage renal disease in a Moroccan population.
The aim of our study was to observe and analyze the spectrum and frequency of nail changes in patients with end stage renal failure undergoing or not hemodialysis (HD).
We led a transverse investigation of all patients with end stage renal failure followed in the department of nephrology of University Hospital Center Hassan II, during a period of three months from 01 August 2016 to 01 November 2016. All patients included in the study had at least 6 months of CRF duration.
The nail apparatus of the patients were examined and photographed by two dermatologists, with a phone camera of 16.0 megapixels. There was also the collection of data from the clinical history, physical and dermatological examination, through a standard questionnaire. Subsequently, the photographs were analyzed separately by three dermatologists and the changes were only considered positive when verified by at least 2 of the 3 specialists. The criteria for positivity were the description of the same nail abnormality by the two dermatologists.
We did not carry out complementary tests to confirm the diagnostic hypothesis of onychomycosis (direct mycological and/or fungal culture) due to the non consent of most patients.
Data collection and analysis was done on computer hardware (SPSS version 17.0). Data thus collected was subjected to statistical analysis for the fulfillment of aims and objectives.
We examined 70 patients (34 men and 36 women). The renal failure duration ranged from 6 months to 13 years. A total of 56/70 (80%) patients had nail abnormalities observed in fingernails and/or toenails. These included absence of lunula (51.7% of patients) (Figure 1), half and half nails (33.9%) (Figure 2), splinter hemorrhages (58.9%) (Figure 3), melanonychia (14.2%) (Figure 4), onycholysis (71.4%) (Figure 5), Beau's lines (35.7%) (Figure 6), koilonychias (Figure 7) and Muehrcke lines (7.1%) (Figure 8), signs of onychomycosis (Association of onycholysis, xanthonychia and leukonychia) (48.2%) (Figure 9), pincer-nail deformity (Figure 10), brittle nails and onychogryphosis (10.7%) (Figure 11), leukonychia (white spots) (25%) (Figure 4), longitudinal ridging (64.2%) (Figure 3), subungual hyperkeratosis (55.3%) (Figure 10), paronychia (5.4%) (Figure 12), nail clubbing (1.8%). The prevalence rates of different types of nail abnormalities detected in CRF patients are shown in Table 1.
 Figure 1: Absence of lunula. View Figure 1
Figure 1: Absence of lunula. View Figure 1
 Figure 2: Half and half nail (clinic and dermoscopy). View Figure 2
Figure 2: Half and half nail (clinic and dermoscopy). View Figure 2
 Figure 3: Splinter hemorrhages and longitudinal ridging. View Figure 3
Figure 3: Splinter hemorrhages and longitudinal ridging. View Figure 3
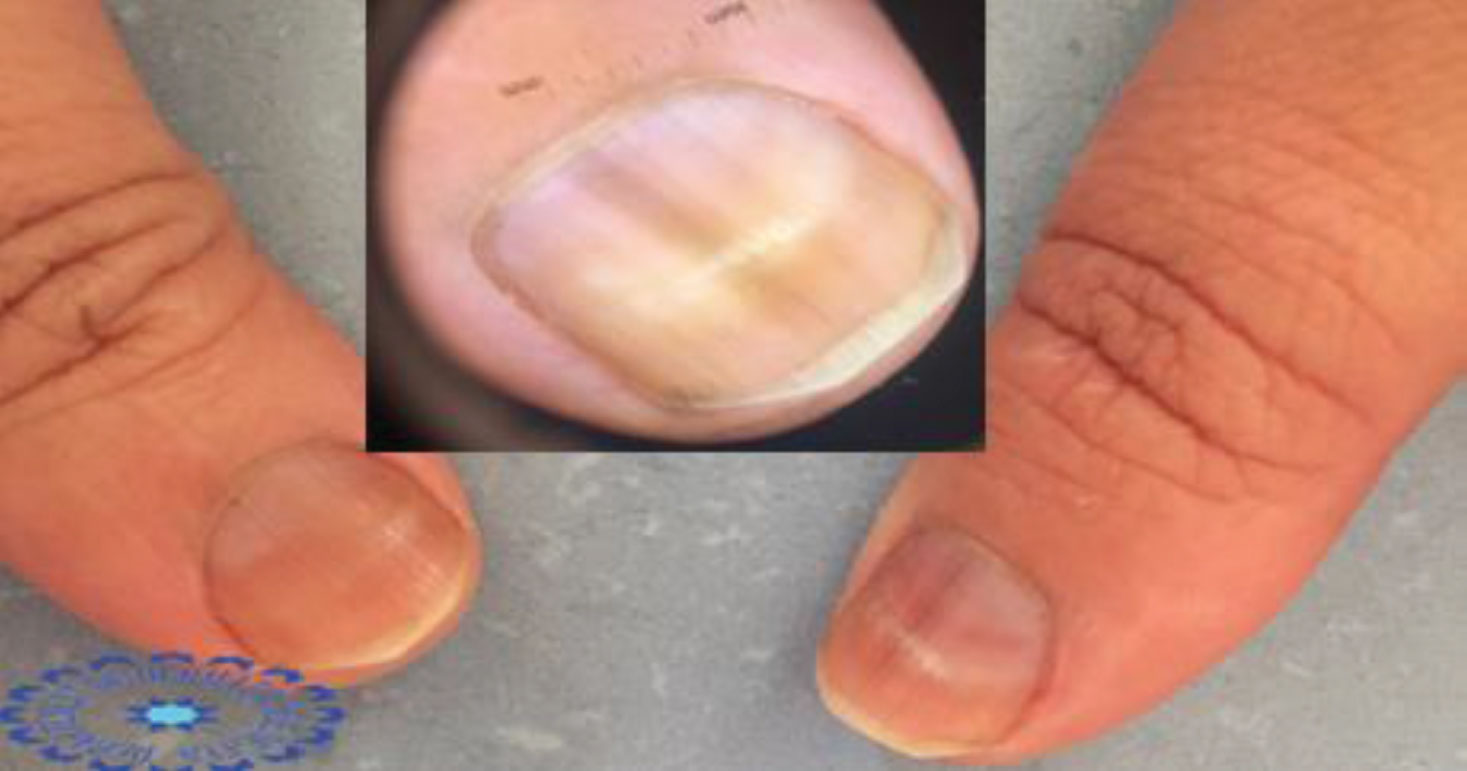 Figure 4: Melanonychia and leukonychia. View Figure 4
Figure 4: Melanonychia and leukonychia. View Figure 4
 Figure 5: Onycholysis (clinic and dermoscopy). View Figure 5
Figure 5: Onycholysis (clinic and dermoscopy). View Figure 5
 Figure 6: Beau's lines. View Figure 6
Figure 6: Beau's lines. View Figure 6
 Figure 7: Koilonychia. View Figure 7
Figure 7: Koilonychia. View Figure 7
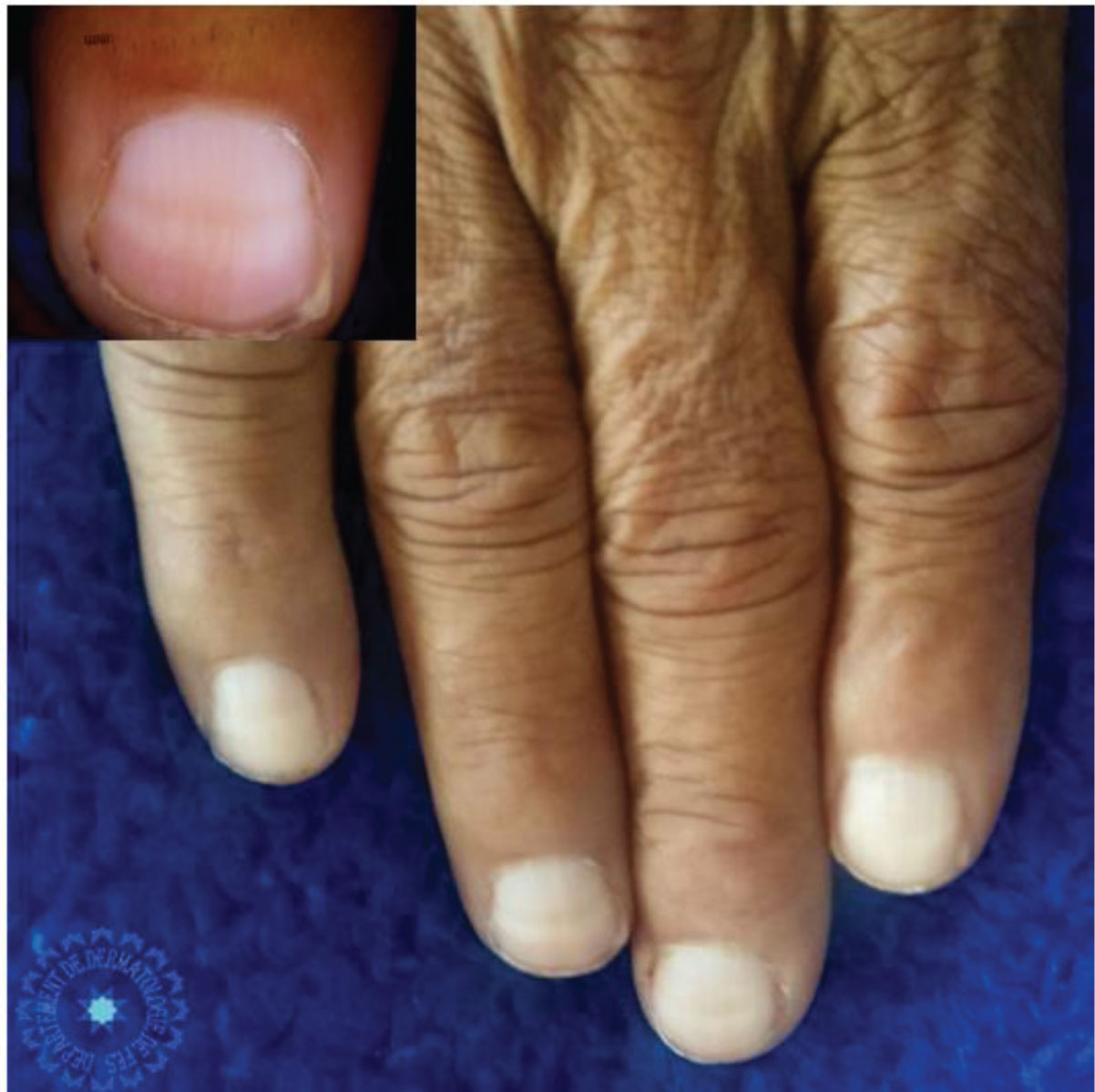 Figure 8: Muehrcke lines (clinic and dermoscopy). View Figure 8
Figure 8: Muehrcke lines (clinic and dermoscopy). View Figure 8
 Figure 9: Signs of onychomycosis (clinic and dermoscopy). View Figure 9
Figure 9: Signs of onychomycosis (clinic and dermoscopy). View Figure 9
 Figure 10: Pincer-nail deformity and subungual hyperkeratosis. View Figure 10
Figure 10: Pincer-nail deformity and subungual hyperkeratosis. View Figure 10
 Figure 11: Onychogryphosis. View Figure 11
Figure 11: Onychogryphosis. View Figure 11
 Figure 12: Paronychia. View Figure 12
Figure 12: Paronychia. View Figure 12
Table 1: Prevalence of different types of nail abnormalities detected in CRF (Chronic renal failure) patients. View Table 1
Our results find no significant relationship between the nail disorders and patient age or duration of renal failure.
Our study demonstrates the polymorphism and frequency of nail abnormalities in patients with CRF. It is known that CRF is related to many skin and nail changes. In our study, 80% of CRF patients had at least one nail abnormality. In studies published previously in the literature, these values ranged from 52-82% [11].
The pathogenesis of these abnormalities remains uncertain: Some of them may be directly related to kidney damage, others seem to be related to its complications or to different therapies received. They are essentially represented by the appearance half and half nail, the absence of lunula and subungual haemorrhage [11,12]. Our results found no significant relationship between nail involvement and patient age or duration of renal failure. This has also been described in other studies [6,9,11]. Some authors have shown a positive correlation between nail changes and duration of haemodialysis [10]. Anaemia is an important etiological factor [13]. Hypoalbuminemia is a known complication of chronic renal failure and suggested to be an etiological factor of nail changes [14]. Several studies found no significant relationship between hypoalbuminemia and nail disorders [9,11].
Onycholysis was the most frequent nail abnormality (71.4%), found in CRF patients. Onycholysis is common in chronic renal failure and can be attributed to different local and systemic causes [11]. Some drugs can also induce photo-onycholysis such as cephalordin or cloxacillin [11,13]. In 75% of cases, it is an infection with Trichophyton rubrum [6].
Splinter hemorrhages are seen in 11-12% of haemodialysis patients [9,11,15]. It is an extravasation of blood from parallel longitudinal vessels of the bed of the nail. It is often seen as the result of microtrauma. The exact pathogenesis remains unclear, but the capillary fragility and Platelet dysfunction, common in chronic renal failure, may contribute to the development of these haemorrhages [11].
Longitudinal ridging are indentations or projections in the relief of the nail plate due to trauma, physiological or secondary alterations to diseases such as: Lichen planus, rheumatoid arthritis, Darier's disease, peripheral vasculopathies and genetic abnormalities. They can also occur due to tumors, near the area of the matrix, that exert compression in the same, leading to changes in the relief of the blade [16,17]. In our study, this change was seen in 64% of CRF patients.
Absence of lunula was a frequent nail abnormality (51.7%), found in CRF patients in our study. Saray, et al. also reported the absence of lunula as the most frequent alteration (31.9%) and suggested that the absence of lunula reflects a variety of conditions in dialysis patients, including metabolic alterations and anemia [9]. It is likely that this change is more related to conditions imposed by CRF than to HD. In our study, the prevalence rate was as high as that found in Martinez MAR's study [18]. However, the absence of lunula can be seen in normal subjects, without any renal insufficiency [19].
Other studies, in contrast, reported the half and half nail, such as the most frequent nail abnormality, in patients with CRF in HD [1,6,20,21]. It was seen in 33.9% among CRF patients in our study. The etiology of this nail change remains unknown [6,22]. Previous studies have observed that the average frequency does not increase with the time of dialysis [6,9] and patients with CRF would already present it before being submitted to HD and may be related to uremia caused by CRF [6]. In other publications, its rates ranged from 7.7% to 50.6% [6,9,10,20,22,23]. Renal transplantation may reduce the rates of this nail disorder [9]. In 1982, Lubach, et al. [22] noted that half and half nail disappeared completely after 2 to 3 weeks of a successful kidney transplant, and Bencini, et al. [20] documented that there was no case through a group of 105 renal transplant patients [9]. It can be found in other diseases such as Kawasaki disease, liver cirrhosis, zinc deficiency, Crohn's disease and pellagra [11].
Leukonychia is seen in cases of acute or chronic renal failure, in cirrhosis of liver, in case of typhoid fever, in patients receiving chemotherapy, and it is the most common nail disorders in renal transplant patients [9,11,24].
Our study found different nail changes in Moroccan uraemic patients, these abnormalities varied from the most frequent (onycholysis) to rare conditions such as nail clubbing. However, the cause of them remains obscure and could not be traced to a particular abnormality in the renal condition, medication or the procedure itself and it needs further investigations to clear up the actual mechanism of their occurrence. The treatment is in most cases symptomatic. Finding pathogenesis of these changes would help us to prevent them.
The study has been approved by the ethics committee of faculty of medicine of fez. An informed consent to participate in the study was obtained from all participants.
Written informed consent was obtained from the patients for publication of this study and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Not applicable.
The authors declare that they have no conflicts of interest.
The authors declare no fundings.
All the authors contributed for the acquisition, analysis, interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and the final approval of the version to be published; and the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Not applicable.