Pityriasis versicolor is a superficial fungal infection of the skin, characterized by pigmentary changes secondary to the colonization of the stratum corneum by a lipophilic dimorphic fungus known as Malassezia sp. Of this genus, 7 species known as the causative agent of pityriasis versicolor, the most frequently isolated species is M. Globosa. This skin disease occurs worldwide but predominates in the tropical, warm, and humid climate. Malassezia sp classified as dimorphic fungi since it behaves as yeast in crops but is capable of producing filaments in its parasitic form. It comes with numerous hyper, hypochromic or erythematous macules, covered with fine flake that converges to form plaques of different morphologies. The most frequent topography is the trunk, the shoulders, and chest in front and back. The diagnosis is clinical, but a mycological study with direct examination must be done. Clusters of rounded or oval yeast clusters are found also fragmented short and thick filaments. The treatment is divided between specific and nonspecific antifungal agents. Recurrences are frequent, up from 60% in the first year and 80% in the second year, so it should be emphasized general measures of treatment.
Tinea versicolor, Malassezia sp
A male patient of 19-years-old, from Apatzingan, Michoacan. With a background of practice boxing the last two years, three times a week. The pathological background includes a pyloroplasty in the neonatal period by pyloric hypertrophy. He comes to the Centro Dermatológico Dr. Ladislao de la Pascua for abdominal stains of two months of evolution, which increase in number and size. Another physician started clotrimazol and dexamethasone without improvement of the lesions. The patient presented a dermatosis disseminated to the trunk and thoracic extremities. Of the first mentioned, it affects the anterior and posterior thorax and the abdomen. Of the thoracic extremities the anterior surface of the arm and forearm, including the antecubital pledges, bilaterally and symmetric. It was a monomorphic dermatosis constituted by multiple hyperchromic and erythematous stains, with furfuracea flake in the surface which is confluent forming multiple oval and circular plates, of different sizes, with a defined edge, constant evolution and asymptomatic (Figure 1). A mycologic study is performed and showed a small number of oval and circular yeast bunches, and the presence of short and thick filaments in the form of cursive S (Figure 2). With the Wood light, it presents positive yellow-golden fluorescence.
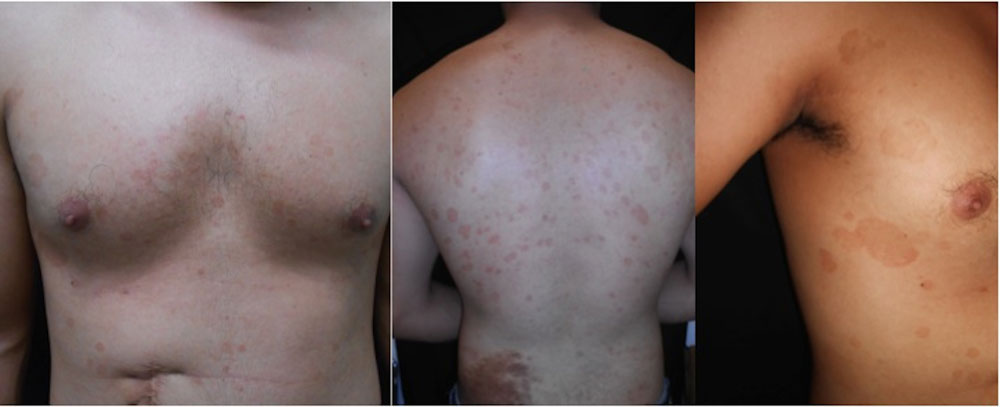 Figure 1: Antherior, posterior and lateral tórax with numerous hyperchromic and erythematous spots covered by with fine flake furfurácea, which come together to formplates. View Figure 1
Figure 1: Antherior, posterior and lateral tórax with numerous hyperchromic and erythematous spots covered by with fine flake furfurácea, which come together to formplates. View Figure 1
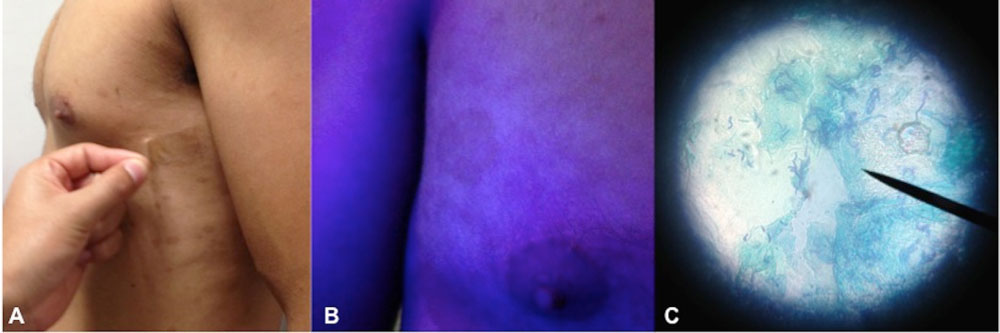 Figure 2: Diagnosis A) The simple is shown with adhesive tape; B) Wood light with golden yellow fluorescence +; C) Direct examination with few clusters of round and oval yeasts, as well as th epresence of short and thick filaments in the form of S cursive. View Figure 2
Figure 2: Diagnosis A) The simple is shown with adhesive tape; B) Wood light with golden yellow fluorescence +; C) Direct examination with few clusters of round and oval yeasts, as well as th epresence of short and thick filaments in the form of S cursive. View Figure 2
In the rest of the skin and annexes, it presented in the lumbar zone a medium congenital melanocytic nevus. The diagnosis of pityriasis versicolor variety hyperchromic and erythematous and intertrigo antecubital is realized, and treatment established with itraconazole 100 mg orally every 24 hours for two weeks and substitution for the soap of Zinc piritionato. The follow up is completed a month after with significant improvement (Figure 3).
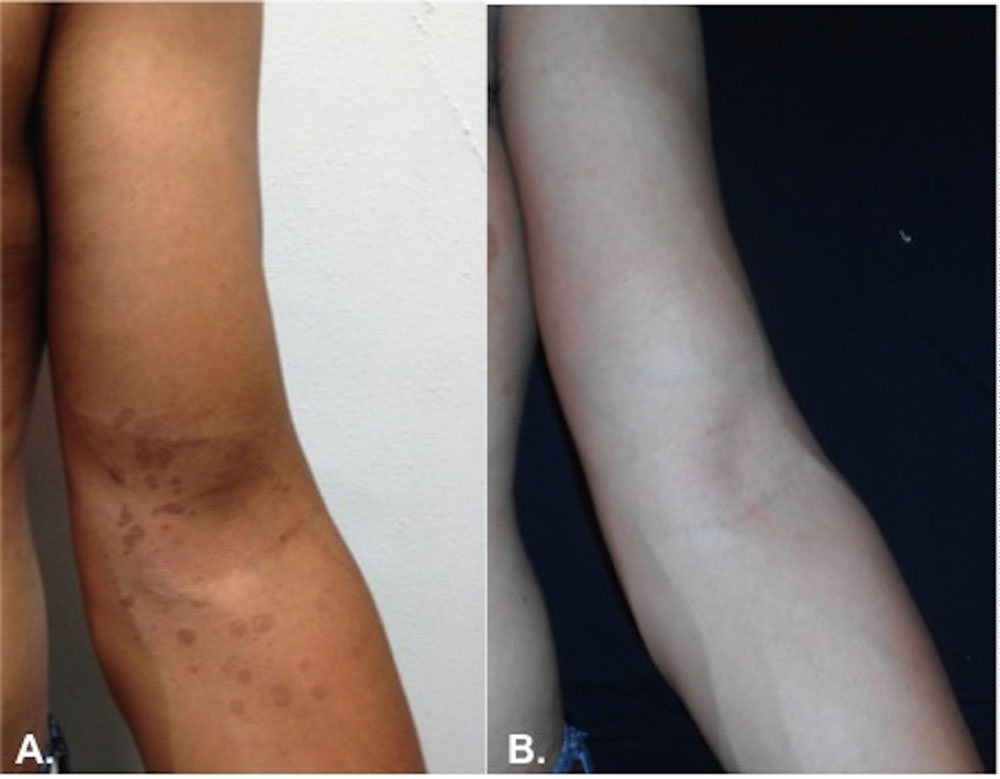 Figure 3: A) Inbreeding by Malassezia; B) Evolution after Treatment with itraconazole 100 mg orally every 24 for 2 weeks and substitute for soap with Zinc pyrithione. View Figure 3
Figure 3: A) Inbreeding by Malassezia; B) Evolution after Treatment with itraconazole 100 mg orally every 24 for 2 weeks and substitute for soap with Zinc pyrithione. View Figure 3
Pityriasis versicolor is a superficial mycosis of the skin, characterized for pigmented changes secondary to a colonization of the stratum corneum for a dimorphic and lipophilic fungus that usually is part of the healthy skin microbiota, known as Malassezia spp [1]. Some authors classified them as saprophytic mycotic infections, to specify the mild inflammatory response in the skin during this disease [2]. It is known too as tinea versicolor, cromofitosis, liver spots, ringworm, furfuracea, tinea flava, parasitic timelessness, and lovesickness [1-3].
According to Gougerot, the Britannic dermatologist William described it in 1801, taking the Word "pityriasis" derived from the Greek "pitiryon", that refers to the image of wheat bran, to designate the characteristic lesions with a delicate and transparent scale [4].
The presence of yeast in pityriasis versicolor was described first by Eichstedt in 1835 [1]. In 1847 Sluyter described it like a disease secondary to the contact with a parasitic plant [3]. Secondary to the difficulty to obtain a culture, for a long time the identification and taxonomic location of this fungus was delayed [5]. Robin, in 1853-1857 considered that the fungus in the lesions with scales was a dermatophyte and call it Microsporum furfur, and the disease was known as tinea versicolor [3]. Castellani, and Chalmers were who culture for the first time the fungus in 1913 and was called Pityrosporum ovale [1]. Panja in 1928 was the first to obtain the P. Ovale and M. Furfur in a culture of Petroff modified medium [6]. When the cultures were realized and confirmed by the lipophilic nature of those structures, different researchers saw the change of a morphologic type to another, concluding that P. orbiculare, P. ovale, and M. furfur are variants from the same species [3]. In a review by Sloof in 1970, it was established that the difference between the yeast that lives in the skin and the ones that produce seborrheic dermatitis or pityriasis capitis, determining that the species Malassezia furfur is the etiological agent of pityriasis versicolor [6]. In the taxonomic review by Yarrow and Ahearn in 1984 [1], the division Basidiomycota and the family cryptococcaceae were considered in the gender Malassezia [3]. Malassezia furfur was considered the only valid number after [1]. The term Malassezia-Pityrosporum have been used, calling it Pityrosporumovale and orbiculare to the yeast and Malassezia to the mycelial phase, but actually, they are synonyms [7].
Based on the genomic differences, in 1990 Simmons and Guèho described a third species, M. sympodialis and in 1996, with the new molecular techniques, serologic and ultrastructural studies, they described 4 more species [2]. In 2002 Sugita, et al. [6] thanks to the molecular techniques for DNA sequence have added M. dermatitis and M. Japónica [2] In 2004, Harai and cols described M. Nana, and two years after, the same group identify M. Yamatoensis, (in seborrheic dermatitis) M. Equina and M. Caprae, in horses and goat respectively [7]. Species of Malassezia gender are recognized as the causal agent of pityriasis veriscolor [1,7]. Traditionally M. furfur was considered the principal causal agent, but the more common species were M. Globosa in 55% to 84% of the cases, followed by M. sympodialis, M slooffiae, M. Restricta, M furfur, M. Pachidermatis, and M obtuse [3,7]. In 1999, Crespo Erchiga, et al., after two studies in Málaga determine that M. globosa was the predominant species in the pityriasis versicolor lesions, confirmed by Nakabayashi and cols. in Japan in 2000 and Aspiroz, y cols., in Zaragosa in 2002, and Hernández, et al. in México in 2003 [2]. Martín González and cols, in 2010, studied 150 patients with pityriasis veriscolor, founding that M. globosa was the principal agent in 54.7% of the cases, followed by M. sympodialis in 13.3% of the cases, without significant differences between the species and the clinical presentation or topography [8]. Epidemiologic studies realized in Canada and Buenos Aires reveal that M. Sympodialis is more common (more than 50%) followed by M. globosa (19.6%) and M. furfur (10.9%) [9].
The status of the species was confirmed in 1990 by an estimation of the percentage of Guanine and Cytokine in the DNA and by reassociation of DNA between the different isolated species [6]. Cunningham and cols. shows that M. furfur is divided into A, B, and C, based in the surface specific antigens. All the yeast was classified by comparison of sequences of RNA subunits (Table 1) [10].
Table 1: Malassezia. View Table 1
The fungus structures are round and globose (M. Globosa and M. furfur), ovoid (M. sympodialis, M. slooffiae, M. restricta, M. furfur) or cylindric (M. obtusa, M. furfur) [3,6]. The only non-lipophilic species is Malassezia pachydermatis because the other require medium and long chain fatty acids as carbon source, the M. pachydermatis was isolated for the first time in the skin of a rhino and have been identified in the dog's ears [1]. The principal lipidic components in the tallow are: Squalene (cholesterol precursor), esters and triglycerides, the components derived from the corneocytes membrane are phospholipids [11]. From the skin surface lipids, the fraction of fatty acids is relatively reduced in polyunsaturated fatty acids. Typically, the tallow is rich in fatty acids of a long chain, with at least 26 carbon atoms, and responsible for the antimitotic and antibacterial properties of the skin [11]. The average percentage of squalene from the total lipids in the skin Surface is 12 to 20% in adults. The high production of squalene in the sebocytes could be by the altered expression of 2 enzymes regulated by oxygen, involved in the metabolism of the squalene, the squalene synthase, and squalene cicloxidasa because in the sebaceous gland the environment is anaerobic [11].
This dermatosis has a worldwide distribution, but is more frequent in tropical zones [7], with warm and wet weather, where have been reported in 40% of population [2]. In México, pityriasis is frequent in the coasts, and in Venezuela have a prevalence of 15.52%. It is developed in any socio-economic level and races [6].
In the statistics of the Micology Unit of the Dermatology Service of the Hospital Regional Universitario Carlos Haya, in Málaga, Spain, it represents a 10% of the cutaneous mycosis [2]. In a study developed in the Centro Dermatológico Dr. Ladislao de la Pascua, in México during 1980, an increased incidence in July and August was reported, with 44% of the cases registered from February to September [4]. In 2005 this dermatosis had an 8.33% of the surface mycosis in this center [3].
It presents more frequently in young men, between 18 to 24 years old, the age with more activity in the sebaceous glands [5,7,9]. It is unusual in adulthood by the diminished production of the tallow. In the newborns or younger than 2-years-old and the pediatrics is very unusual too [1]. It has been related to the gestational age, hospital stay, time in the incubator, and antibiotics administration [5]. The hospitalized patients could have some risk factors like immunocompromise, more significant sweating, shower with less frequency, and clothes change [1].
Malassezia includes a group of lipophilic yeasts with natural habitat in the human skin and other mammals [2]. It is located in the seborrheic skin, and the most frequent location is the scalp, forehead, external auditive conducts, nasolabial folds, and trunk [1,6]. The density of the population vary between 104 units colony forming units (UFC)/cm2 in the trunk and 102 UFC/cm2 in the extremities. It has been observed an increase in childhood and adolescence, and diminishes in the senescence [1]. The fungus can be located in the air follicles inside or between the keratinocytes; it is suggested that only hifas invaded the cells and can be observed at any level in the corneal layer, being more frequent in the inferior layers. Around the fungus, lost of quarantine structure is appreciated, and it is not known yet if it is by a mechanical rupture or chemical rupture [1,6].
They are classified as dimorphic fungi since in crops they behave like yeast and are capable of producing filaments in their parasitic form. It is found as a saprophyte on the skin in the form of spherical and oval blastoconidia; when conditions are favorable, it becomes pathogenic [1]. It has been classified as Basidiomycota in the family Cryptococcaceae [6]. The monopolar budding typical of Malassezia yeasts allows the identification of the genus. The identification in vitro can be carried out by simple techniques, based on the study of the macro and microscopic morphology of the colonies, the reaction of catalase and beta-glucosidase (escualin test) as well as the study of the pattern of requirement or assimilation of different lipids such as Tween 20, 40, 60, 80 and cremophor EL [2].
The factors that participate in the conversion of one phase to another can be divided into exogenous and endogenous [1]. The first are sun exposure, high temperatures, and environmental humidity, so the disease is more frequent in the tropics and during the summer in template climates. The use of clothing with synthetic fibers, therefore, through an increase in the production of CO2, with subsequent modifications to the cutaneous pH and alterations in the microbiota that lead to greater development of Malassezia species. Sports activities, sweating, use of oils and bronzers, use of topical or systemic corticosteroids, and oral anticoagulants [1,2,6,7]. Endogenous factors include chronic infections, use of systemic or immunosuppressive steroids, oral contraceptives, hyperhidrosis, malnutrition, Cushing's syndrome, use of lithium, seborrheic dermatitis, the body's altered immune response, as in acquired immunodeficiency syndrome and in visceral leishmaniasis, where pityriasis versicolor may be more prevalent and manifest with forms or locations that are infrequent or more severe. A family history of mycosis has been described in approximately 17% of patients [1,7].
It presents as a dermatosis with many patches of variable color, either hyper or hypochromic or erythematous, with fine furfuraceous scale, which converges to form plates of different morphologies, from dotted, nummular, lenticular, reticular or follicular [1,3]. The color of the lesions can vary from pink, light brown, brown, hypochromic, or even achromic. They may have the same hue or present different colors in the same patient [1]. The pink and brown tonality is more frequent in covered areas, in exposed areas the most frequent are whitish lesions [2]. The clinical presentation is asymptomatic or with scarce pruritic, chronic evolution, and recurrent [3,7].
The most frequent topography is in the trunk, shoulders, and thorax, being more abundant in the back according to the distribution of sebaceous glands [1,7]. Followed by proximal segments of arms, thighs and neck [7]. It can occur in areas covered by the clothes, less frequently the popliteal and antecubital folds, armpits, penis or in a field of radiation. It has also been reported on the scalp [1]. During infancy, it is most frequently found on the face, on the forehead, cheeks, intraciliary region, preauricular, perioral and nasolabial grooves, especially in the hypochromic variety [7]. A topography that is infrequently affected is the antecubital, axillary, and inguinal folds. When these are involved, it is called intertrigo by Malassezia, which was described in 1988 by Katoh, et al. in Japan and is characterized by asymptomatic erythematous patches [3].
Depending on the color, it can be classified as hypochromic, hyperchromic, or erythematous, being the first the most frequent [3,7]. According to the form: Vitiligo (acromial), dermatofitoid (with active pseudo border) and atrophic (a complication of therapy with fluorinated corticosteroids) [3,7]. According to Tosti, et al., the alterations caused by Malassezia settle in the outer two-thirds of the stratum corneum, with which the function of the skin barrier is diminished, allowing greater penetration of the steroids [6].
In hypopigmented lesions, there are few spores, and little inflammatory infiltrate. The indole pigment synthesized by M. furfur is probably a powerful ultraviolet filter, although it has not been possible to demonstrate that this substance blocks UV light and hypopigmentation occurs in this way since lesions develop even in non-photo exposit areas [1]. Once the mycelia are arranged in the stratum corneum, by lipoperoxidation, they produce dicarboxylic acid and azelaic acid, which act by inhibiting dopa tyrosinase [6,12]. A direct cytotoxic effect on the melanocytes has also been proposed, which explains the dyschromia in the hypochromic variety. The size and distribution of melanosomes can be modified in both melanocytes and keratinocytes, those melanosomes, very small; they translate into hypopigmentation [13]. The pathogenesis of hyperpigmentation is not yet fully understood. Several theories are postulated: it is proposed that the stratum corneum is more thickened and both spores and hyphae are more numerous, presenting a denser lymphocytic inflammatory infiltrate, acting as a stimulus for the melanocytes [12]. Hyperpigmentation may be the result of changes in the formation of melanosomes, which are observed larger [1]. Another proposal is the interaction of Malassezia with its microenvironment in which, the yeast would stimulate the production of pigment using as a resource the tryptophan content in sweat; although it has been observed that Malassezia by itself, in vitro, is capable of producing a pigment similar to melanin. Microscopically, large melanosomes are observed, and desquamation appears to be a consequence of the keratolytic activity of the fungus. 6 Merkel cells in hyperpigmented skin contain melanosomes, and secretory granules combined, suggesting an increase in their activity. The erythematous variety is possibly due to a mild inflammatory reaction, which can cause changes in skin color and melanocytes can be stimulated by it [1]. There is a form called "Tinea Rosea de Castellani" or flava, which is a yellowish variety, frequent in South Asia, with more frequent topography on the face. Cases of pityriasis versicolor "nigra" or "nevoid" have also been described [4]. In dark-skinned infants, especially in the tropics, a clinical variant is usually observed, where the infection begins in the areas covered by the diaper and extends in rapid form causing depigmentation. This clinical form is called parasitic acromia or pityriasis versicolor alba [3].
The Gougerot classification, divided into 7 groups: 4
1. Squamous or Pityriasis (non-erythematous)
2. Nummular erythematoscamosa, variety of points
3. Erythematosquamous ring and circinate
4. Nummular erythematosus
5. Nummular and circinate erythematosus
6. Alba with adherent scales
7. Leucomenanodermic
Classification of Saints in 1971:
a) By coloration: hyperchromic, hypochromic or erythematous
b) By extension: localized or generalized
c) By the shape of the lesions: In drops, in plates or annular.
It is mainly clinical. The desquamation of the lesions is manifested by scraping the skin with a curette or directly with the nail, called the Besnier sign or the nail, or, with transparent adhesive tape (Scotch tape test), the pressure is applied on them to make the flake adhere [1]. Samples are taken from the desquamating edges of the lesion since in this area there is a higher number of microorganisms. Direct examination is performed, adding 10% potassium hydroxide or Albert's solution (toluidine blue, malachite green, glacial acetic acid, ethanol, and distilled water) 3 or "Parker" blue ink is used or stained with Gram [1,3]. Purple structures are observed which are oval or rounded, clustered, yeast yeasts measuring from 4 to 8 μm, as well as short, thick, septate and sinuous fragmented filaments, in the form of cursive S of 2 to 4 μm [5,7]. If these elements are presented together they give an image called in "meatballs and spaghetti" [1]. The culture is not necessary for diagnosis, but it is done with Dixon's medium (peptone, bacteriological agar, dried bile, Tween 40, glycerol monooleate), [6] olive oil and oleic acid, glycerol monostearate, Tween 80, bile salt lipids and cow's milk have been used in solid media. M. pachydermatis, which is not lipo dependent, grows in conventional media such as Sabouraud added with antibiotic [1].
They are incubated at optimum temperatures of 30 to 35℃ with a humid atmosphere; the plates are wrapped in plastic bags to ensure the right degree of humidity and to avoid drying the medium [1,2]. In 7 to 8 days, yellowish-white colonies develop, creamy, with irregular edges. In the mycology laboratory of the Ladislao de la Pascua Dermatological Center, 46.3% isolation was reported in Mycosel cultures added with olive oil, from lesions of pityriasis versicolor [3]. The catalase reaction is determined using a 10-volume drop of hydrogen peroxide on the smear or the slide. The production of gas bubbles indicates oxygen release; it is considered positive. For M. pachydermatis, the catalase reaction is usually adverse or very weak, whereas M. restricta is the only lipid-dependent species that do not have this reaction [6]. We can support with Wood's light (filtered UV light with a peak at 365 nm) to identify subclinical plates. Yellow-gold or yellow-green fluorescence is observed, which is present in only one-third of cases, of which the majority is caused by Malassezia furfur. 1-3 Fluorochromes, especially pityria lactone, are responsible for the fluorescence of the lesions. The intensity of the fluorescence is not proportional to the degree of the lesions. It is negative, especially when the skin is wet with sweat [3].
Skin biopsy is rarely required; the direct examination is better and more accurate than histopathological study [6]. The stratum corneum is full of hyphae and cellular, rounded, fungal elements that are more visible with PAS staining or Silver methenamine; some of these elements can be located within the keratinocytes. Hematoxylin-eosin stain shows orthokeratotic hyperkeratosis, absence of the granular layer and acanthosis of the epidermis, perivascular lymphocytic infiltrates, plasma cells and histiocytes in the dermis [1]. Electron microscopy shows large swollen melanocytes, vacuolation of the mitochondria and severe degeneration of some cells in the hypopigmented areas. Also, in hyperpigmented lesions, there are abnormal melanosomes of considerable size, and in hypopigmented ones, they are smaller than the standard size [6].
1. Pityriasis Rosada de Gilbert. The presence of heraldic medallion and the subsequent acute outbreak of erythematous lesions should be investigated. Besides, this picture is self-limited, which does not happen with pityriasis versicolor, which tends to be chronic and recurrent [4].
2. Vitiligo. Especially in its early stages, when it can be presented with hypochromia, rather than with acromia, in addition to not presenting the characteristic scale on the spot [1-4].
3. Psoriasis. In the cases in drops and little scattered. The sign of Auspitz could be orientador [4].
4. Eritrasma. In hyperpigmented pityriasis versicolor lesions, it is difficult to distinguish it from erythrasma, which is why it has been called Pityriasis veriscolor erythrasmoide [2]. Although Wood's light examination allows differentiating them due to the characteristic fluorescence of each entity, the direct examination will clarify the diagnosis [6].
5. Dermatophytosis. In them is the characteristic active edge; they have an eccentric growth and healing is observed in the central area [4].
6. Indeterminate cases of leprosy, it should be taken into account that lesions of leprosy will present dysesthesia and anhidrosis [3,4].
Progressive macular hypomelanosis of the trunk must be differentiated from the hypochromic variety. This entity is characterized by hypopigmented lesions of variable size, which are located mainly in the trunk, lower back, buttocks, upper chest, abdomen, flanks, and upper extremities. It appears without a history of previous skin damage, infection or inflammation, its etiology is not clear although the participation of P. acnes is mentioned [6]. Other: pityriasis alba, seborrheic dermatitis, reticulated and confluent papillomatosis of Gougerot-Carteaud, hypochromic solar dermatitis, remaining spots [1,3].
Those that do not possess antifungal activity, act by physical or chemical removal of the infected stratum corneum or interfering with cell turnover [1].
1. Selenium sulfide: 2.5% in lotion, cream or shampoo for a week and day 1 and 3 of each month for 6 months. The disadvantage, bad smell, is not cosmetic [13].
2. Propylene glycol: Acts as keratolytic, effective dissolved in 50% water. It is applied every 12 hours for 2 weeks [13].
3. Unnthement of Whitfield, constituted by benzoic acid (fungistatic) and salicylic acid (keratolytic) in proportion 2: 1 [13].
4. Preparation of 25% sodium thiosulfate with 1% salicylic acid. Others, such as benzoyl peroxide and tretinoin, povidone iodine [13].
1. Halprogina. Halogenated phenolic ether, with fungicidal activity against Malassezia, which has shown effectiveness in the disease [13].
2. Zinc pyrithione: It is used as a 1% shampoo for 2 weeks, leaving it to act for 5 minutes [13].
3. Tolcylate: It belongs to the group of thiocarbamates. Tolcylate blocks the biosynthesis of sterol by inhibition of squalene epoxidase. It can be used in 1% cream or lotion.
4. Cyclopiroxolamin: It is a hydroxypyridone with broad-spectrum antifungal action, it is used in 1% cream [13].
5. Azoles: They are fungistatic, inhibit the biosynthesis of ergosterol, and thus alter the formation of the cell membrane. 1% bifonazole, 1% clotrimazole, 2% fluconazole, 2% ketoconazole, 2% miconazole, 2% sertaconazole, 1% sulconazole and 1% tioconazoleare used. They are used every 12 or 24 hours for three to four weeks [3,13].
6. Griseofulvin is not useful systemically [13].
7. Terbinafine: It belongs to the allylamines. The 1% solution is effective applied once a day for 2 weeks or 2 times a day for 7 days. It is not effective when used systemically [13].
8. Lithium succinate: molecule especially effective against Malassezia, use not only in pityriasis versicolor but also in facial seborrheic dermatitis [13].
It is preferred to reserve it for cases that involve a large body surface when the disease is recurrent if topical medications have failed or according to the patient's preference. Its main advantages are improving patient satisfaction, optimizing compliance and reducing the time needed for the patient's healing [1].
Ketoconazole, itraconazole and fluconazole are the main used drugs in those cases with specific sensibility for some species of Mallazesia [6,13].
The recurrence rate can be as high as 60% in the first year and 80% in the second year [1]. Badillet and Sene found M. furfur in smears of the nasal mucosa, suggesting that this location could be a refuge not accessible to topical therapy and that it would cause recurrence [6]. The importance of endogenous factors and the environment make recurrences frequent [1]. Ketoconazole has been used to prevent relapse in doses of 400 mg once a month or 200 mg a day for 3 consecutive days once a month. Itraconazole at 400 mg in a single dose once a month for 6 months was effective in prophylaxis for pityriasis versicolor than placebo [1]. Either the use of shampoo with Zinc pyrithione during bathing [3]. After treatment, hypochromia may remain residual for several months [6].