The two week wait pathway initiative was proposed in 1997 to expedite referrals from general practice to dermatology and to facilitate access to timely treatment for patients with suspected skin malignancy. However, since its implementation it has come under fire for its poor specificity and case detection rate with dermatologists raising concerns about their increased workload and consequently lack of time for other urgent cases. The present study conducted at Queen's Hospital, London aimed to assess (i) The proportion of referred patients seen within two weeks and treated within 62 days (ii) The proportion of patients referred for suspected malignancies that were subsequently confirmed and (iii) What benign skin lesions were most commonly referred to dermatology. We audited 83 patients who were referred to Queen's Hospital between April to June 2019 under the two-week wait pathway. Data was collected using patient notes, EPro, Cyberlab, and BlueSpier.
The results show that two-week wait referrals for suspected skin cancer from GP's have a low diagnostic accuracy and this may be contributing to delayed patient care within the hospital setting. In previous studies conducted in the United Kingdom, approximately 20% of GP referrals for squamous cell carcinoma or melanoma using the two-week wait proforma are later diagnosed through histopathology. In this study, 13.2% of patients referred were found to have squamous cell carcinoma, basal cell carcinoma or melanoma. The three main diagnostic groups in this study were: Seborrhoeic keratosis (26.5%) benign naevus (20.5%) and basal cell carcinoma (9.6%). Furthermore, only 65% of patients referred had a dermatology appointment within 14 days of referral and 75% of patients requiring treatment were treated or scheduled to be treated within 62 days. These results suggest that greater knowledge and confidence is required amongst GP's in the Queen's Hospital catchment area to improve diagnostic accuracy in patients with skin cancer. It is likely that a combination of education and resources will be required to meet the demands of this population effectively.
The two-week wait pathway was first introduced in the U.K in 1997, in a bid to expedite the referral of suspected cancer patients from primary care to specialists and thus improving survival. This was also thought to help alleviate psychological distress associated with diagnostic uncertainty in patients. Under this initiative, the NHS cancer referral timeline stipulates that general practitioners (GPs) are to refer patients to specialists via a standardised faxed proforma within 24 hours of the consultation, following which consultations with specialists are to take place within 2 weeks of referral and treatment is to commence within 62 days [1]. As of April 2020, a new goal is being introduced which aims for patients who are referred for investigation of suspected cancer to receive a diagnosis within 28 days (Figure 1) [2,3].
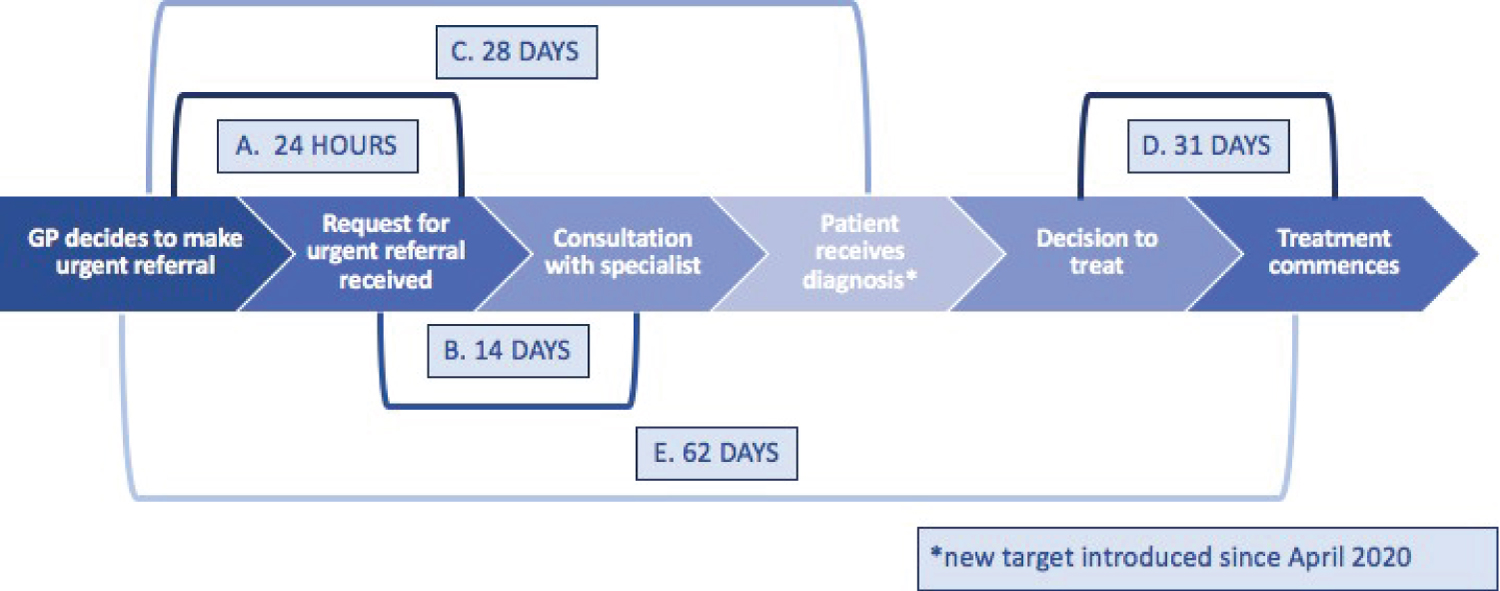 Figure 1: A schematic to show the NHS time targets in the two week wait referral pathway. Adapted from [3].
View Figure 1
Figure 1: A schematic to show the NHS time targets in the two week wait referral pathway. Adapted from [3].
View Figure 1
Amongst skin cancers, squamous cell carcinomas and melanoma are referred through this two-week wait pathway to specialist departments including dermatology, plastic surgery and maxillo-facial surgery [4]. Since 2015, NHS guidelines recommend that suspected melanoma cases should be referred via the two-week wait pathway if they score greater than 3 on the weighted seven point checklist (Figure 2) [5].
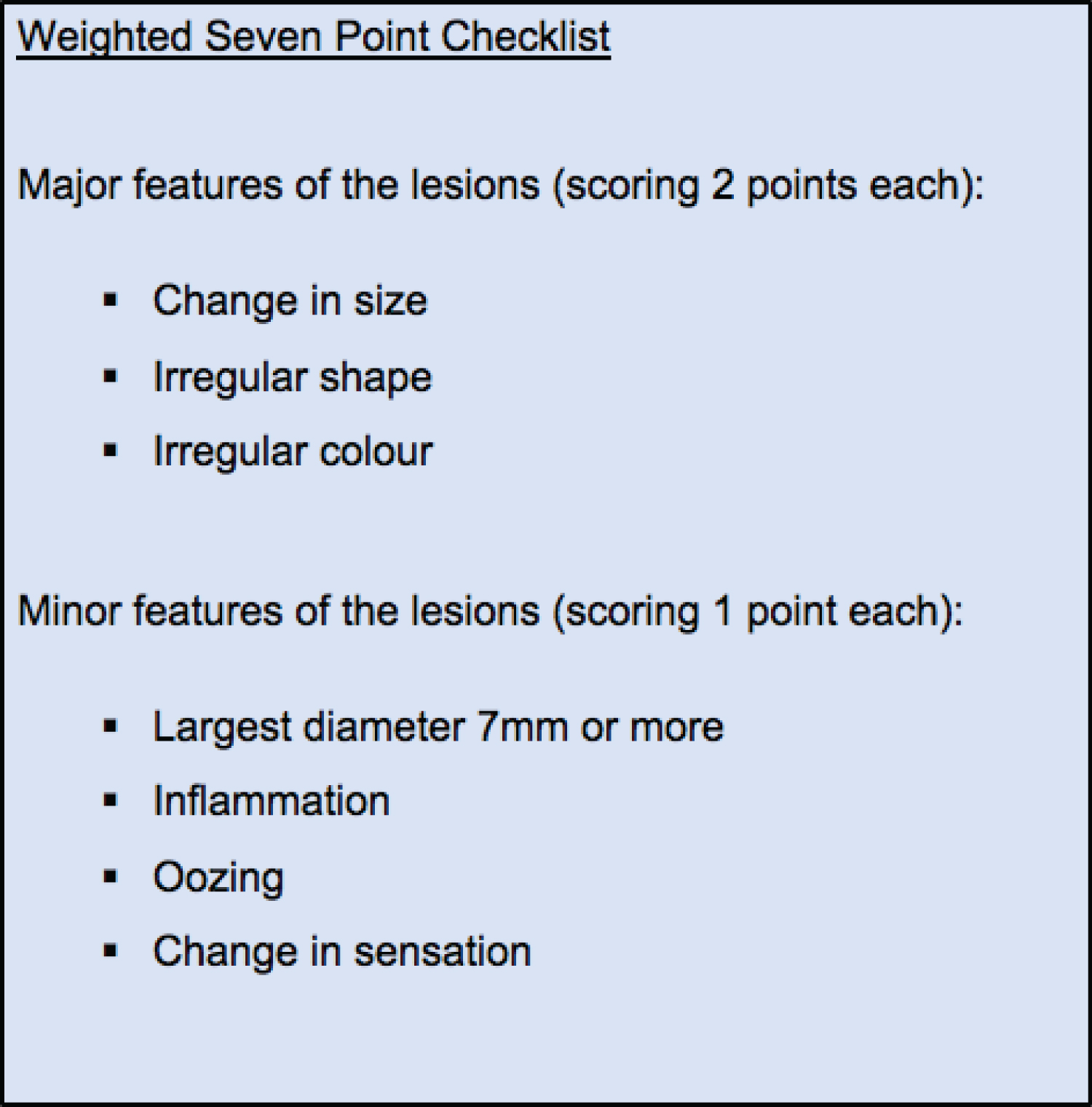 Figure 2: The criteria in the weighted 7 point checklist for diagnosing melanoma. Adapted from [5].
View Figure 2
Figure 2: The criteria in the weighted 7 point checklist for diagnosing melanoma. Adapted from [5].
View Figure 2
Suspected squamous cell cancer is to be referred via the two week wait pathway if the lesion 'raises suspicion' of this condition [5]. Basal cell carcinomas (BCC) are only referred through this mechanism if it is deemed that a delay in referral will significantly worsen the outcome, based on lesion size and site. This is because basal cell carcinomas are often indolent and rarely metastasize [5-7].
Whilst proponents of the two week wait pathway note that it facilitates referral decisions for G.Ps and decreases waiting times for patients, a growing concern amongst specialists that this has overburdened the system without improving the cancer detection rate, has been reported since its inception [8,9]. It has led to a high rate of referral of benign lesions. Critics have argued that this has increased the rate of referrals without a commensurate increase in resources and staffing. Other concerns include the displacement of other cases due to the increased referral volume and the lack of ability for specialists to prioritise referrals based on their expertise [10].
In this clinical audit, we aimed to investigate the efficiency of this referral mechanism 20 years on from its introduction. Our study is the first to evaluate the diagnostic accuracy of skin cancer referrals using the two-week wait pathway following on from the 2015 update in the NHS guidelines to change the melanoma checklist, from unweighted to weighted.
Our study had 3 objectives to assess if the two week wait targets were being achieved as well as the diagnostic accuracy of this referral mechanism.
The objectives were (i) To determine the proportion of referrals seen in the dermatology department within the target of two weeks of the General Practitioner's (G.P.) urgent referral (ii) To assess the diagnostic accuracy of skin lesion referrals and (iii) To ascertain which benign lesions were most commonly referred through this pathway.
Local ethical approval from the Clinical Auditing Team at Queen's Hospital was obtained prior to the study.
The study site was Queen's Hospital, London, a teaching hospital in Barking, Havering and Redbridge University Hospitals NHS Trust, which serves a population of 750,000 [10]. The dermatology department at Queen's Hospital is led by five consultants and an associate specialist [11].
Data pertaining to the demographic details, reason for referral, histological diagnosis and outcome was collected from patient notes and software programmes EPro, Cyberlab, and BlueSpier and cleaned. Cases were excluded if referrals were not for a two week wait condition or if information pertaining to the dates of referral, histological diagnosis and dermatology consultation were omitted from records (Figure 3). Different subtypes of the same condition were classed as a single category (eg. all forms of benign naevi were grouped together in the final outcome).
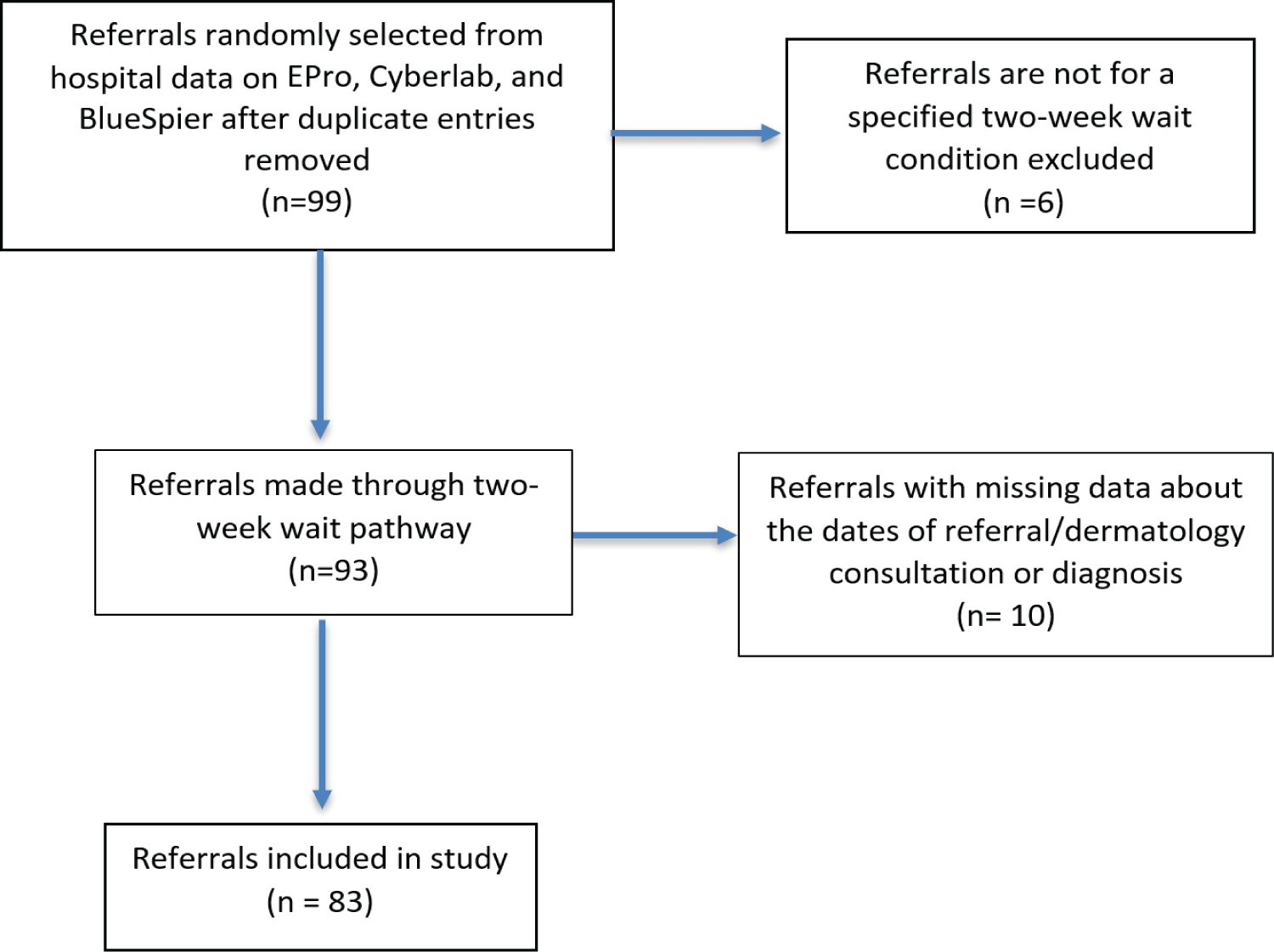 Figure 3: PRISMA diagram explaining the criteria for inclusion in the study.
View Figure 3
Figure 3: PRISMA diagram explaining the criteria for inclusion in the study.
View Figure 3
For cases that were included, time between the referral being made by the G.P. and the consultation with the dermatologist as well as the time between referral and treatment commencing were compared against the NHS cancer referral timeline and the agreement between G.P. and histopathological diagnosis was assessed to determine diagnostic accuracy. The overall rate of malignancy amongst the total referrals was also determined. The benign lesions most commonly referred through this pathway were identified.
102 referrals for skin lesions, made via the two week wait pathway between April and June 2019 to the Dermatology department at Queen's Hospital, were selected for audit at random. Of the 83 cases eligible for inclusion in the study, 48 were female and 35 were male. The mean age of the cases included in this study was 57.9 years with a range between 22 and 90 years.
In this study, 83.1% of referred patients were diagnosed with a benign condition, whilst 9.6% had BCC and 3.6% had SCC (Figure 4). No patients were found to have melanoma. A further 3.6% of patients were found to have dysplasia. The overall prevalence of malignancy amongst referrals in the study was 13.2%. Overall the top three main diagnostic categories were Seborrhoeic Keratosis (26.5%), Melanocytic Nevus (20.5%) and BCC (9.6%) (Table 1).
Table 1: Conditions according to final outcomes and referral. View Table 1
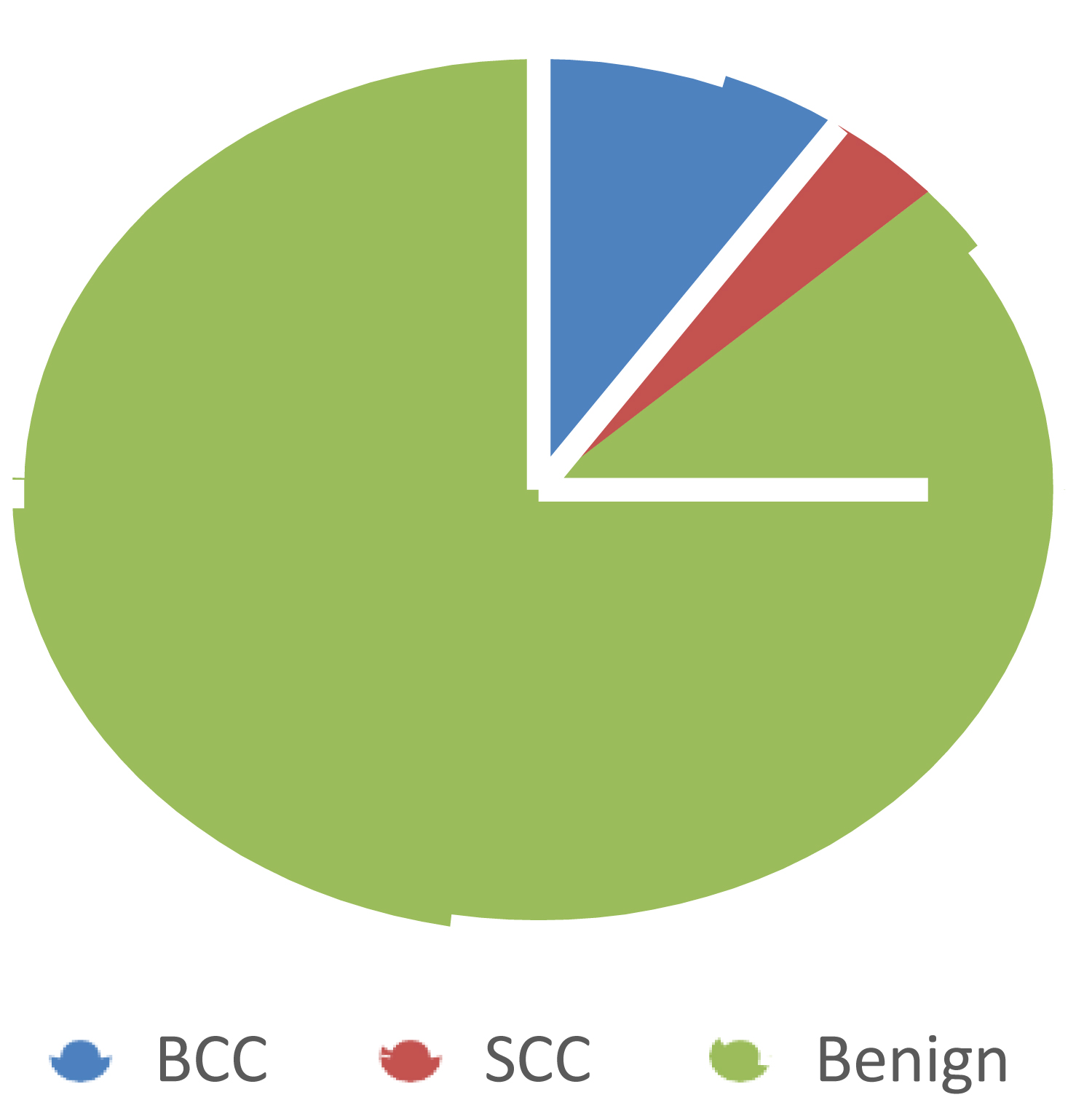 Figure 4: Proportion of Benign to Malignant Diagnoses.
View Figure 4
Figure 4: Proportion of Benign to Malignant Diagnoses.
View Figure 4
Overall 4.8% of the referrals, comprising 2 cases for each of BCC and SCC, were correctly identified by the GP.
Only the positive predictive value (PPV) was calculated in the study since it was not possible to ascertain the number of patients who had been seen by the G.P and were not subsequently referred because they were deemed not to have a malignancy i.e. the false negative and true negatives.
Although melanoma was the most common reason for referral, no patients were histologically confirmed with this in this study. The most common diagnosis amongst referrals for melanoma were seborrheic keratosis (34%) followed by benign naevus (30.2%) (Table 2).
Table 2: Histological diagnoses for suspected melanoma referrals. View Table 2
BCC was the most frequently histologically identified malignancy, comprising 9.6% of all diagnoses. The PPV of suspected BCC was higher than SCC and melanoma at 40%. Moreover, on 5 occasions, referral for another 2 week wait condition was later histopathologically confirmed as BCC. Conversely, 1 referral for BCC later was diagnosed as SCC (Table 3).
Table 3: Histological Diagnoses for Suspected BCC Referrals. View Table 3
Only 2 out of 24 suspected cases of SCC identified by the GP were later histopathologically confirmed. This is reflected in the low PPV of 8.3%. The most common misdiagnoses amongst referrals for SCC were BCC, actinic keratosis, dermatitis and seborrhoeic keratosis (Table 4).
Table 4: Histological Diagnoses for Suspected SCC Referrals. View Table 4
Whether a malignancy was correctly identified by GPs despite the specific condition being wrong was also assessed. Amongst 53 referrals for melanoma, 2 non-melanoma malignancies were identified by GPs. Likewise amongst 24 referrals for SCC, 2 malignancies that were not SCC were picked up. 1 case of SCC was diagnosed out of the 5 referrals for BCC.
65% of patients had a dermatology consultation within 14 days of their GP referral. The mean number of days between the GP referral and dermatology consultation was 16.9 days (Table 5).
Table 5: The distribution of cases referred within each time period. View Table 5
The mean wait between referral and consultation for suspected melanoma, SCC and BCC was 16.5 days, 14.8 days, 18.7 days respectively. The mean wait for a case later diagnosed as SCC and BCC was 13.5 and 19.1 days respectively whilst for dysplasia it was 16.3 days.
28 patients underwent procedures or were scheduled appointments for procedures following their histological diagnosis. The target for time from initial GP referral to treatment commencing is 62 days. 21 of the 28 (75%) patients underwent or were booked appointments for procedures within 62 days of the GP referral. The mean duration of the wait between GP referral to date of procedure was 44 days. A further 8 patients underwent simple procedures such as routine excision and cryotherapy, although the date of the procedure was not recorded. Another 7 patients were still awaiting an appointment for a procedure at the time of the data collection. Of those who did not undergo or were not scheduled to undergo any procedures, 28 patients were discharged whilst 10 were scheduled for follow up and monitoring.
The mean wait between referral to procedure for histologically diagnosed SCC was 80 days whilst for BCC and dysplasia it was 72 and 49.5 days respectively.
The current system of dermatology referrals from primary care is designed to be sensitive, facilitating rapid assessment of suspected skin malignancies in dermatology clinics, at the expense of specificity. However research has shown that this has led to the overburdening of dermatology departments with benign lesions, a finding which has been corroborated by the present study [1,12].
The overall pick-up rate for malignancies in this study was 13.2% which is similar to previous studies in the UK where the pick-up rate was 19% [13], 10% [4], 12% [9, 22% {Matteucci, 2011 #2}] and 34.5% [14]. As in previous studies , seborrhoeic keratoses and benign naevi were the most common benign conditions amongst GP referrals for melanoma, indicating that these are conditions that GPs often find difficult to distinguish from melanoma, likely because they can also be pigmented [13,15].
Only 4.8% of the referrals made in this study by the GP were later histologically proven to be correct. This is significantly lower than other studies in the UK and in Ireland where 45% and 22% of malignancies were correctly referred by the GP respectively [16,17].
As in previous papers, BCCs were the most commonly diagnosed malignancy and had the highest diagnostic accuracy at 40% [15]. It can be speculated that the reason for diagnostic accuracy being the highest for BCC is due to the fact that it is the skin malignancy that GPs encounter most frequently owing to its prevalence. It is notable that 6 out of 8 histological diagnoses of BCC were initially referred for a different 2 week wait condition. BCCs should only be referred via the two week wait pathway if the size or location of the lesion is clinically concerning. Further educating GPs to distinguish between different malignancies could help decrease potentially unnecessary urgent referrals for BCC which are often indolent tumours that rarely metastasise. SCC was the second most commonly diagnosed malignancy. As in previous studies, the PPV of SCC was lower than that of BCC but higher than that of melanoma [4,18]. The PPV of SCC in the present study at 8.3% was lower than other studies where it has ranged from 17.6% to 21.9% and 33.3% [4,14,15]. Actinic keratosis and BCC represented the most common misdiagnosis amongst SCC referrals consistent with findings in previous studies [15,18]. Despite malignant melanoma being the most common reason for referral, no cases were identified in the study. It is probable that our small sample size and the low incidence of melanoma (16,175/100,000 per year) contributed to the paucity of cases identified [19]. Other studies have shown mixed results with regards to the diagnostic accuracy of melanoma which has ranged from 7.8% to 36.8% [4,9,14,15].
The two week wait referral system is premised on the fact that earlier detection, diagnosis and thus treatment will lead to improved outcomes for patients. However the present study has shown that the majority of referrals made through this system are benign lesions. ¾ of dermatologists in a past study expressed that they thought too many benign lesions were being referred [10]. In one department, the increase in two week wait referrals has doubled the waiting times for other referrals [8,9]. The present study was not able to ascertain the number of skin cancer referrals made through other referral routes and to other departments such as plastic surgery, but in previous studies this has represented as high as 50% of melanoma diagnoses and 92% of SCC diagnoses [4]. Based on the volume of benign lesions picked up by the two-week wait proforma, it can be surmised that some referrals made through other routes which subsequently turn out to be cancer and, more generally, other urgent conditions may be delayed. The two week wait system can only be justified if the majority of malignancies are diagnosed within this group and not in cases referred through other routes.
Assessing the number of patients who were not referred by the GP but subsequently developed skin malignancies was beyond the remit of a study. Such a study would necessitate long term follow up to identify the false negative cases. Had it been possible to have done so, this would have allowed determination of the sensitivity of the proforma. A retrospective study of colorectal cancer patients found that 30% of cases would not have met the two week wait referral criteria [20]. It is unknown whether this is similar for skin malignancies. Moreover, cases who do not meet the referral criteria are often those with lower risk symptoms that could have a better prognosis with treatment [8].
In this study, 65% of referrals met the NHS target of being seen in the dermatology department within 14 days and 75% of patients were treated or scheduled to be treated within 62 days.
During the period April to June 2019 in England, 90.2% of all referrals to specialists suspected of malignancy were seen within two weeks and treatment within 62 days of referral was achieved in 77.3% of cases [21]. A previous study in dermatology departments found that the two week target was being met in 90% of the cases and the 62 day target in 97% of cases [14]. Another similar study found the two week wait target was being achieved 83% of the time [13]. Our findings, based on a small-scale study, deviate from these past results, particularly with respect to the two week target. It was not possible to determine the reasons for the delays in referral found in this study. Prior studies have found that this may be due to rejection of the soonest available appointment date within 2 weeks by the patient, the patient missing their appointment or the GP making a routine referral that was subsequently regraded to a two week wait referral [13,14]. As this study did not assess whether the referrals to dermatology were made within 24 hours of the GP consultation as per NHS targets, failure to achieve this target may also explain the overall delay from referral to dermatology consultation.
The severity of the malignancy appeared to have little bearing on the mean number of days to the dermatology consultation: Whilst melanoma typically progresses faster than SCC, it was on average seen within 16.5 days whilst SCC was seen within 14.8 days. It is pertinent to note that there were different numbers of referrals for each condition which could influence the mean number of days. Dermatologists have voiced concerns over their inability to use their clinical expertise to prioritise referrals due to the current referral system [9]. A system which allows for more detailed information to be recorded by the GP, beyond what is provided in the proforma, could enable dermatologists to prioritise cases. Furthermore, it is well-established that patients that meet referral criteria are often deemed to not be appropriate referrals in the opinion of the consultants [8]. Allowing dermatologists the liberty to prioritise cases might prove to be a sound strategy to improve efficiency.
The NHS indicators for evaluating the two week wait system are based entirely on whether the timeline targets are being met. This has been subject to critique since the shortcomings of this system, highlighted in this study and in others, have resulted in benign cases comprising the overwhelming majority of referrals [9]. Updating these targets to include measures of diagnostic accuracy would be a more accurate reflection of the success and efficiency of this system.
Alongside patient pressure and concerns over prolonged wait times for routine referrals, clinical uncertainty has been identified as contributing to over-referral by GPs, who may have little post-graduate training in dermatology [9,22]. Therefore, more rigorous training on recognising malignant skin lesions and distinguishing between malignancies and common misdiagnoses such as seborrhoeic keratoses or benign naevi, may hold promise in improving efficiency of referrals. This has been successful in the past: following a 4 hour module, GPs in Italy were able to identify malignant cases with increased specificity whilst maintaining sensitivity [23]. With the rapid technological developments occurring, there could also be a role for computer aided decision support for GPs.
A contributing factor to the high volume of referrals for benign lesions in this study is that guidelines from National Institute of Clinical Excellence (NICE) encourage GPs to refer uncertain lesions via the two week wait pathway for biopsy by a specialist [24]. Options to overcome this include training GP's to perform biopsies of suspicious lesions which can subsequently be sent to histopathology for diagnosis, reducing the numbers of potentially non- malignant lesions being reviewed in dermatology. Another alternative could involve utilising online services for rapid dermatologist review for remote assessment of suspicious skin lesions where there is uncertainty to determine if requirements for skin cancer pathway referral are met. This could present an effective strategy given that specialists such as dermatologists and plastic surgeons have consistently achieved better diagnostic accuracy compared to GPs with rates between 66% and 100% [9,14,25-27].
Recent reports have alerted GPs to the rising number of missed diagnosis of malignant melanoma. Between 2017-2018, 79 incidents related to delayed and missed diagnoses of melanoma were filed with the Medical Defence Union, 80% of which were against GPs [28]. Further training on how GPs can document their decisions to protect themselves against medical negligence suits where patients do not present with clinical symptoms suggestive of cancer but subsequently develop it, may equip GPs with the confidence to diagnose lesions as benign. GPs currently practicing revealed another medico-legal factor potentially influencing GP referral of suspected skin malignancy: Large indemnity fees. GPs who err on the side of caution are often rewarded with lower premium rates, influencing GPs to make more referrals.
Discrepancy in the number of referrals achieving the two-week wait targets in this study compared to the national statistics could be explained by the amount of deprivation within the catchment area of Queen's Hospital. Barking and Dagenham is one of the most deprived boroughs in London and has the lowest average life expectancy compared to any other London borough. Using specialist GP's in dermatology for the diagnosis of skin cancers in the area as well as taking biopsies in the community may also ameliorate the current situation.
These results suggest that greater support is required amongst GP's in the Queen's Hospital catchment area to improve diagnostic accuracy in patients with skin cancer. It is likely that a combination of education and increased resources will be required to improve diagnostic accuracy of 2-week-wait referrals.