Goltz syndrome (focal skin hypoplasia) is a genetic disorder that primarily affects the skin, skeletal system, eyes and face. People with Goltz syndrome have birth defects. These disorders include very thin skin veins (skin hypoplasia), pink yellow nodules, subcutaneous fat, lack of upper skin layers (aplasia cutis), small clusters of superficial skin vessels (telangiectasia), and veins in dark skin Or bright. Goltz syndrome is caused by mutation genes PORCN, TWIST2, HCCS.
Goltz syndrome, PORCN, TWIST2, HCCS genes, Skin and Skeletal disorders
Goltz syndrome (focal skin hypoplasia) is a genetic disorder that primarily affects the skin, skeletal system, eyes and face. About 90 percent of people with Goltz syndrome are women, and men with symptoms usually have fewer symptoms and symptoms than women. It should be noted that some people with Goltz syndrome also have intellectual disabilities [1] (Figure 1).
 Figure 1: Images of a newborn with Goltz syndrome associated with related disorders in the skin.
View Figure 1
Figure 1: Images of a newborn with Goltz syndrome associated with related disorders in the skin.
View Figure 1
People with Goltz syndrome have birth defects. These disorders include very thin skin veins (skin hypoplasia), pink yellow nodules, subcutaneous fat, lack of upper skin layers (aplasia cutis), small clusters of superficial skin vessels (telangiectasia), and veins in dark skin Or bright. These skin changes may cause pain, itching, irritation, or skin infections. Papillomas, such as zygomatic mice, are not usually present at birth, but appear as adults grow up in the Goltz syndrome. Papillomas are usually formed around the nose, the lips, the anal holes and the genitals of women with Goltz syndrome. In addition, papillomas may be present in the throat, especially in the esophagus or larynx, and can cause swallowing, respiration or sleep poisoning. The papillomas can be removed if necessary by surgery from the growing regions. People with Goltz syndrome may have small and abnormal nails on the toes. In addition, hair in the scalp of these people can be weak or fragile or not [2] (Figure 2).
 Figure 2: Images of a newborn with Goltz syndrome associated with related disorders in the skin.
View Figure 2
Figure 2: Images of a newborn with Goltz syndrome associated with related disorders in the skin.
View Figure 2
Many people with Goltz syndrome also have hand and foot disorders, including abnormalities such as oligodactyly in fingers and toes, fingers and legs (cindactyly) or ecd rhodactyly. X-rays can show veins of modified bone density called osteopathia striata [3] (Figure 3).
 Figure 3: Images of the organs of a person with Goltz syndrome associated with focal hip hypoplasia, dental dysfunction, oligodactyly, synodactyly, and octreotiline on the fingers and legs.
View Figure 3
Figure 3: Images of the organs of a person with Goltz syndrome associated with focal hip hypoplasia, dental dysfunction, oligodactyly, synodactyly, and octreotiline on the fingers and legs.
View Figure 3
Eye disorders are common in people with Goltz syndrome and include symptoms such as abnormal (microphalomatic) eyes, unexplained eyes (anophthalmia), sight (strabismus), eyelid splint (ptosis), rapid pupil eye movement (nystagmus) and tear problems are also common. In addition, people with Goltz syndrome may have defects in the sensitive light tissue behind the eye (retina) or nerve that transmits visual information from the eye to the brain (the optic nerve). This abnormal growth of the retina and the optic nerve may cause a chunk of the eye structure called coliboma. It should be noted that some of these abnormalities in the eye do not affect visual acuity, while others may also experience diminished vision or blindness [4] (Figure 4).
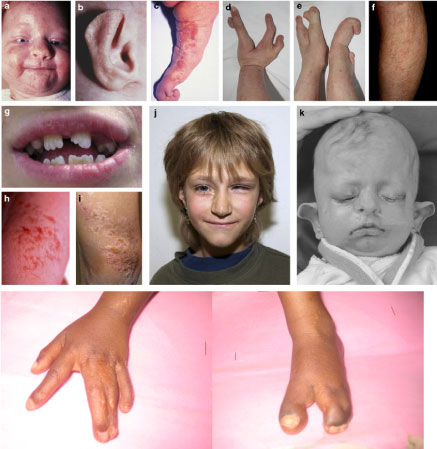 Figure 4: An overview of Goltz syndrome disorder.
View Figure 4
Figure 4: An overview of Goltz syndrome disorder.
View Figure 4
People with Goltz syndrome may have facial features. The injured people often have a small, thin thumb, small ears, nasal holes that are smaller than normal, asymmetry left and right in the face (face asymmetry). These facial features are usually very delicate. In addition, cleft palate and cleft palate may also occur in people with Goltz syndrome [5] (Figure 5).
 Figure 5: An overview of Goltz syndrome disorder.
View Figure 5
Figure 5: An overview of Goltz syndrome disorder.
View Figure 5
About half of the patients with Goltz syndrome have dental disorders, in particular enamel dysfunction. Kidney and gastrointestinal disorders are also common in Goltz syndrome. The kidneys may also fuse with people who have kidney infections that are susceptible to kidney disease, but typically do not cause significant problems in their health. The main gastrointestinal disorder that occurs in people with Goltz syndrome is an ampholecole, which is a hole in the abdominal wall and allows abdominal organs to escape through the umbilical cord. It is worth noting that the symptoms of Goltz syndrome are very different, although almost all people with this syndrome experience skin disorders [6].
About 90% of the cases of Goltz syndrome are due to the mutation of the PORCN gene, which is based on the X-linked limb X-chromosome arm Xp11.23. This gene contains the instructions for protein synthesis that is responsible for changing other proteins, which is called the WNT protein. The WNT protein is involved in the chemical pathways of body signaling, which regulates the growth of the skin, bones and other structures of the body before birth. About 10% of cases of Goltz syndrome are due to mutations in TWIST2 and HCCS genes. The TWIST2 gene is positioned in the long arm of chromosome number 2 as 2q37.3, and the HCCS gene is based on the x-ray x-chromosome short arm Xp22.2 [7] (Figure 6).
 Figure 6: Schematic view of the X chromosome X, which is based on the PORCN gene in the short arm of this chromosome as Xp11.23.
View Figure 6
Figure 6: Schematic view of the X chromosome X, which is based on the PORCN gene in the short arm of this chromosome as Xp11.23.
View Figure 6
The mutation in the PORCN gene seems to eliminate the production of PORCN protein. The researchers believe that the WNT protein of the cell will not be released without the PORCN protein. When the WNT protein is not able to leave the cell, they can not participate in chemical signaling pathways that are critical to natural development. It is worth noting that the various symptoms and symptoms of the Goltz syndrome are due to the unusual signaling of the WNT protein during the development of embryonic development [8].
Most cases of Goltz syndrome in women are caused by new mutations in the PORCN gene, which in fact, the syndrome in women does not follow any patterns and is sporadic. But Goltz syndrome in men follows the dominant X-pattern inheritance. Because men have an X chromosome, mutations in any of the X-linked chromosome genes will result in men's disease, and since women have two X-chromosomes, a mutated gene in one of these chromosomes, the disease phenotype Because healthy X-rays of chromosomes cover the mutated allele and women are considered as carriers of the disease [9] (Figure 7).
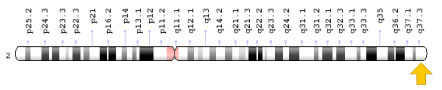 Figure 7: Schematic view of chromosome number 2, the TWIST2 gene located in the long arm of this chromosome 2q37.3.
View Figure 7
Figure 7: Schematic view of chromosome number 2, the TWIST2 gene located in the long arm of this chromosome 2q37.3.
View Figure 7
Goltz syndrome is a rare genetic disorder that is unclear in the world. So far, about 200 to 300 cases of Goltz syndrome have been reported from medical literature throughout the world, and only 10% are men who have been born alive [10].
Goltz syndrome is diagnosed based on the clinical and physical findings of the patients and some pathological tests. Using radiological techniques such as kidney ultrasound, abdominal MRI, x-ray, eye test, and auditory assessment are also effective in detecting Goltz syndrome. The most obvious method for detecting Goltz syndrome is the molecular genetic testing of the PORCN gene to investigate the presence of possible mutations [11] (Figure 8).
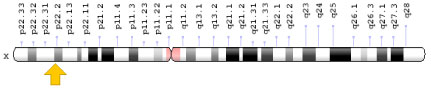 Figure 8: A schematic view of the X chromosome X that the HCCS gene is based on in the short arm of this chromosome as Xp22.2.
View Figure 8
Figure 8: A schematic view of the X chromosome X that the HCCS gene is based on in the short arm of this chromosome as Xp22.2.
View Figure 8
The Goltz syndrome treatment and management strategy is symptomatic and supportive. Treatment may be undertaken by a team of professionals including pediatricians, eye specialists, ENT specialists, dermatologists, nephrologists, and other healthcare professionals. There is no definitive treatment for Goltz syndrome and any clinical measures are needed to reduce the suffering of the sufferers. Genetic counseling is also a special place for all parents who want a healthy baby [12,13] (Figure 9 and Figure 10).
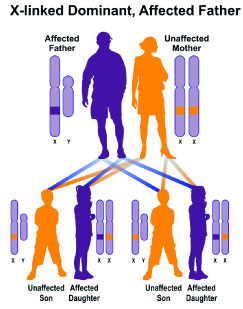 Figure 9: A schematic view of the X-dominant hereditary pattern (patient's father) that Goltz syndrome complies with this pattern.
View Figure 9
Figure 9: A schematic view of the X-dominant hereditary pattern (patient's father) that Goltz syndrome complies with this pattern.
View Figure 9
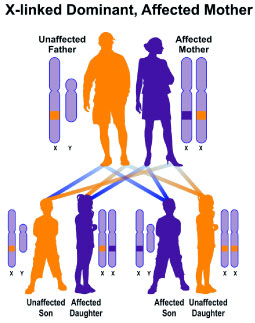 Figure 10: Schematic view of the X-dominant hereditary pattern (patient's mother), which follows the Goltz syndrome.
View Figure 10
Figure 10: Schematic view of the X-dominant hereditary pattern (patient's mother), which follows the Goltz syndrome.
View Figure 10
Goltz syndrome was first reported in 1962 by Dr. Robert Goltz, a dermatologist from Chicago, USA [14] (Figure 11).
 Figure 11: The image of Dr. Robert Goltz, Discoverer of Goltz syndrome.
View Figure 11
Figure 11: The image of Dr. Robert Goltz, Discoverer of Goltz syndrome.
View Figure 11
Goltz syndrome (focal skin hypoplasia) is a genetic disorder that primarily affects the skin, skeletal system, eyes and face. People with Goltz syndrome have birth defects. These disorders include very thin skin veins (skin hypoplasia), pink yellow nodules, subcutaneous fat, lack of upper skin layers (aplasia cutis), small clusters of superficial skin vessels (telangiectasia), and veins in dark skin Or bright. Goltz syndrome is caused by mutation genes PORCN, TWIST2, HCCS. There is no definitive treatment for Goltz syndrome and any clinical measures are needed to reduce the suffering of the sufferers.