We present a case of a 66-year-old man who presented with a history of Right Hemianopia and Right sided facial droop and weakness. CT and MRI brain imaging demonstrated areas of infarction affecting the vascular regions supplied by Left Middle Cerebral Artery and Left Posterior Cerebral Artery circulation. Carotid Duplex Arterial imaging demonstrated moderate Left Internal Carotid Artery Stenosis and CT Angiography demonstrated a dominant Left Posterior Communicating Artery. The origin of the multi-territory Stroke as demonstrated on the MRI scan was his underlying Carotid disease. The patient underwent a successful Left Carotid Endarterectomy.
This case highlights the fact that patients presenting with isolated Posterior Cerebral Arteryterritory stroke or mixed Posterior Cerebral Artery and Middle Cerebral Artery territory strokes and ipsilateral Internal Carotid Artery stenosis, should have a low threshold to be assessed with CT or MR Brain Angiography to determine if variants in Cerebral Circulation exist.
Ischaemic stroke, Carotid artery stenosis, Foetal variant posterior, Communicating artery
Stroke is a common condition with multiple underlying aetiologies. Multi-territory Stroke involving both Anterior and Posterior Cerebral circulation is normally attributed to Cardio-embolic disease. In a small but significant proportion of the adult population there is a Foetal variant Posterior Communicating Artery [PCOM] which supplies the Posterior Cerebral Artery [PCA] from the Anterior Cerebral circulation [1]. In these patients symptomatic ipsilateral Carotid Artery disease can present with both Anterior Cerebral circulation and PCA territory Stroke [2].
A 66-year-old man presented with a one day history of Right Hemianopia and a 6 hour history of Right sided facial droop and weakness. His risk factors included Hypertension, Hypercholesterolaemia and a 50 pack year smoking history. Clinical examination confirmed above findings and initial Brain Computed Tomography [CT] scan demonstrated areas of low attenuation in the left Cerebral Hemisphere, involving the left Caudate Nucleus, left Occipital Lobe and left Parietal Lobe posteriorly (Figure 1). Brain Magnetic Resonance Imaging [MRI] confirmed CT findings and demonstrated multiple areas of infarction affecting the vascular regions supplied by Left Middle Cerebral Artery [MCA] and Left PCA circulation (Figure 2). The suggestion that these Infarcts were more than likely to represent a Cardio-Embolic source was mooted and appropriate Cardiac investigations were instituted.
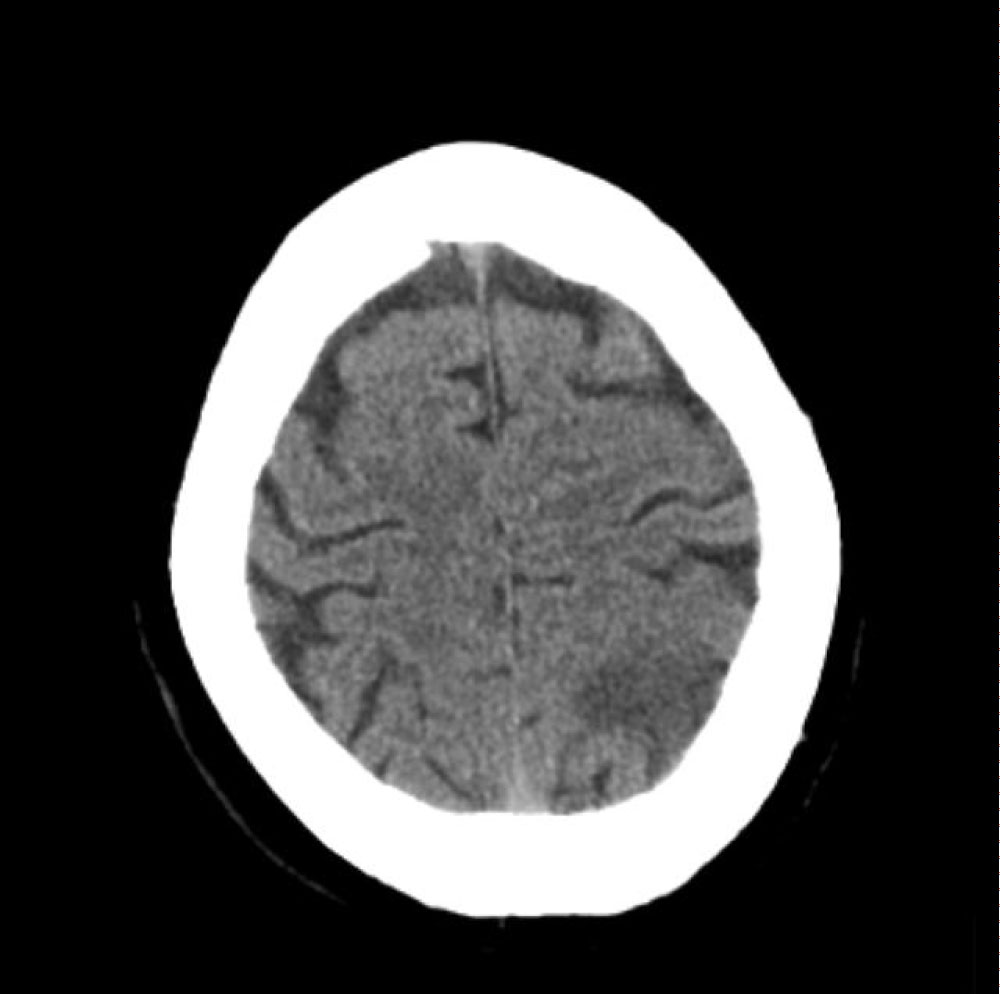 Figure 1: CT Brain scan demonstrating low attenuations in the Left Occipital Lobe and Left Parietal Lobe posteriorly. View Figure 1
Figure 1: CT Brain scan demonstrating low attenuations in the Left Occipital Lobe and Left Parietal Lobe posteriorly. View Figure 1
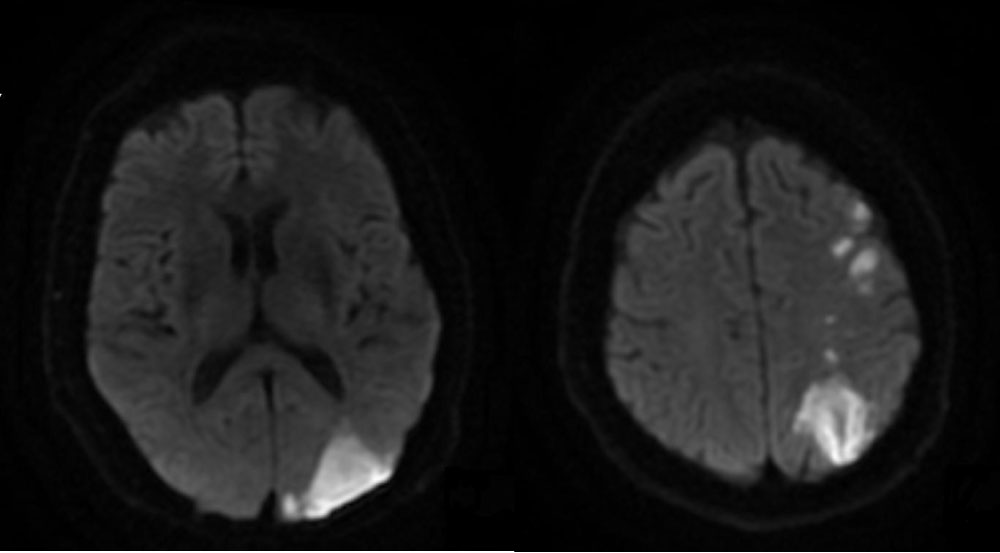 Figure 2: MRI Diffusion Weighted Imaging of the Brain demonstrating multiple areas of infarction affecting the vascular regions supplied by Left MCA and Left PCA circulation. View Figure 2
Figure 2: MRI Diffusion Weighted Imaging of the Brain demonstrating multiple areas of infarction affecting the vascular regions supplied by Left MCA and Left PCA circulation. View Figure 2
Echocardiography proved to be normal with no evidence of a structural or embolic Cardiac source and Cardiac monitoring demonstrated Sinus Rhythm without any significant Atrial Arrhythmias. Haematological and Biochemical parameters were within normal limits. Carotid Duplex Arterial imaging demonstrated patent bilateral Common Carotid Arteries with a moderate Left Internal Carotid Artery [ICA] Stenosis quantified through velocity measurements at 50-59%. This was initially thought to be a coincidental finding as Posterior Circulation Infarcts could not be normally explained with Carotid Stenosis; however it was decided to qualify these findings further with CT Angiography.
CT Angiography demonstrated a large ruptured plaque of heterogeneous morphology in the Left ICA associated with a propagating Thrombus (Figure 3). These findings were associated with a dominant Left PCOM feeding the Left Posterior Cerebral circulation and thereby explaining the fact that the plaque present in the Left ICA was able to seed the Left Middle Cerebral and the Left Posterior Cerebral circulation and in fact; the origin of the multi-territory Stroke as demonstrated on the MRI scan was not Cardio-Embolic but in fact related to his underlying Carotid disease. The patient underwent a successful Left Carotid Endarterectomy and has made an excellent functional recovery. He remains on high dose Statin and Anti-Platelet therapy. The decision to investigate the presumed moderate Carotid Stenosis demonstrated on Duplex imaging with CT Angiography was central to the diagnosis and further management.
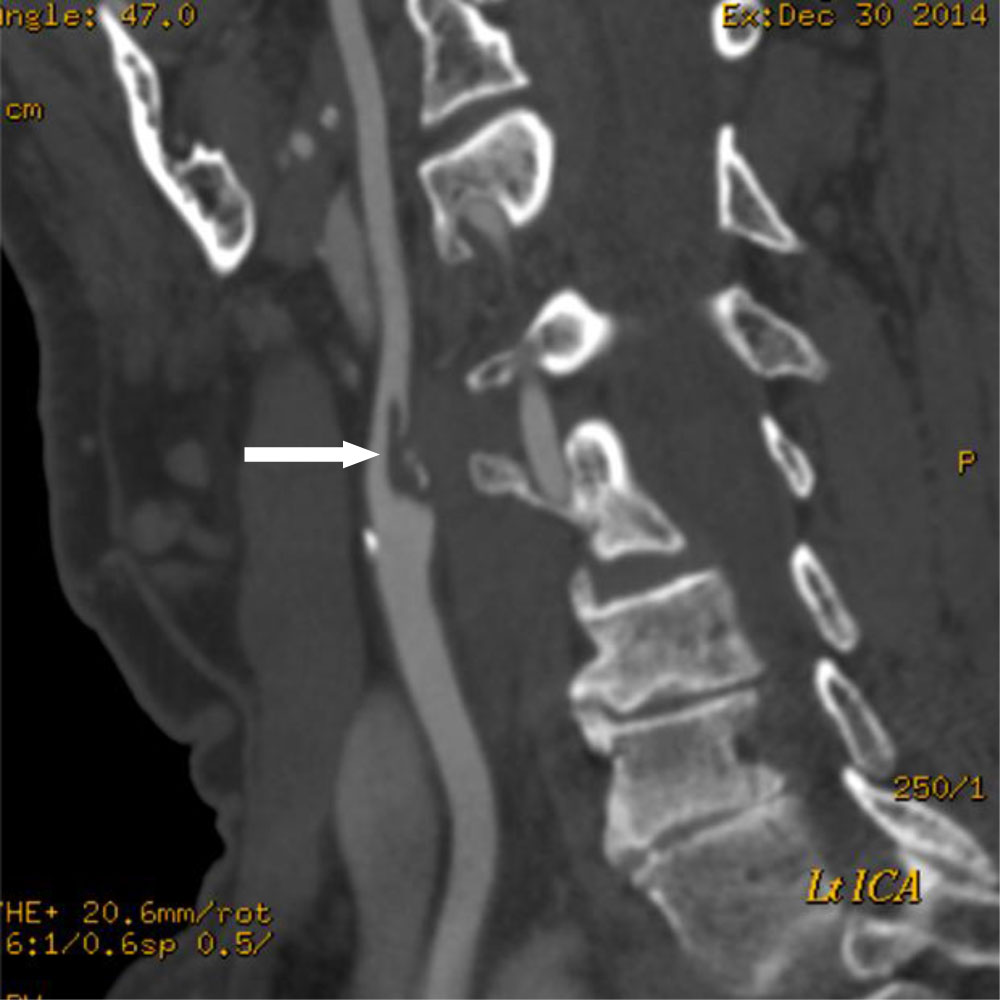 Figure 3: CT Carotid Angiography demonstrating a large ruptured plaque in the Left Internal Carotid Artery (white arrow). View Figure 3
Figure 3: CT Carotid Angiography demonstrating a large ruptured plaque in the Left Internal Carotid Artery (white arrow). View Figure 3
The importance of this case is to highlight unusual presentations of common conditions. Stroke has multiple aetiologies including Atherosclerotic Large Vessel Extra-Cranial disease and Cardio-Embolic disease accounting for nearly 50% of all Strokes. The Carotid vascular tree generally supplies the Middle and Anterior Cerebral circulation and the Vertebro-Basilar system supplies the Posterior Cerebral circulation. Where Imaging suggests multi-territory [unilateral and bilateral] infarcts especially involving Anterior and Posterior circulation, the diagnostic balance shifts in favour of a Cardio-Embolic source as it is a commonly held view that Carotid disease related Strokes should not involve the Posterior circulation territories. While this view is accurate in the majority of cases, a high threshold of suspicion must be exercised. In a small but significant proportion of the adult population, there is a Foetal variant PCOM and in these individuals, it is the PCOM [arising from the MCA and thereby Anterior circulation] that provides the majority of blood supply to the Posterior Cerebral areas.
Foetal variant PCOM is the commonest anatomical variant of the Posterior circulation of the Circle of Willis. It is related to hypoplasia or absence of the P1 segment of the PCA. It occurs in up to 29% of the adult population and is more commonly found unilaterally [1]. CT Angiography has been shown to be both a sensitive and specific tool in identifying Foetal variant PCOM [3]. It must be noted that the Foetal variant PCOM does not per se increase the incidence of PCA territory ischaemic Stroke [4]. However, in patients with Anterior and Posterior Circulation territory ischaemic Stroke with ipsilateral Carotid disease, consideration must always be given to further imaging to determine if the Foetal variant PCOM exists [2].
Our case demonstrates symptomatic Carotid Artery Disease resulting in both MCA and PCA territory strokes due to a Foetal variant PCOM. Reliance on Carotid Duplex imaging alone does not allow for Intra Cerebral Vasculature to be determined and there is a risk that patients with the above presentation with mild to moderate ipsilateral Carotid Stenosis may be offered best medical treatment instead of Surgery based on the presumption that the Stroke may be Cardio-embolic in nature. Given the benefits of Carotid Endarterectomy in symptomatic stenosis [5] and the incidence of Foetal variant PCOM; we highlight the fact that patients presenting with isolated PCA territory stroke or mixed PCA and MCA territory strokes and ipsilateral ICA stenosis, should have a low threshold to be assessed with CT or MR Brain Angiography to determine if variants in Cerebral Circulation exist.