To evaluate the proportion and characteristics of patients diagnosed with neovascular age-related macular degeneration (AMD) who do not complete the loading dose of bevacizumab, given as first line agent.
Using the electronic medical records of all patients affiliated to the largest health maintenance organization in Israel who received intravitreal injections of bevacizumab between September 2008 and October 2014, we isolated patients aged of 60 years or more treated for neovascular age-related macular degeneration. We considered patients with less than three injections and those having completed the initial course within 100 days as two separate groups. We then compared patients living at the end of follow-up in terms of demographics and baseline conditions.
22.3% of all patients started with bevacizumab did not fulfill the loading dose within 100 days. Mortality was higher in patients not achieving induction (32.5% vs. 20.2%, OR = 2.39, CI: 2.04 - 2.80, p < 0.001). When considering patients living at the end of the follow-up, 13.7% did not receive the loading dose. We found a larger proportion of rural residents in patients who failed induction than in those who received three injections or more (OR = 1.54, 95% CI: 1.23 - 1.92, p < 0.001). Patients, living at the end of follow-up, who failed to complete the loading dose were relatively younger than patients with three or more injections (79.6 vs. 80.7 vs. years, p < 0.001). No other demographic variable and no specific medical condition was found to be associated with failure to complete induction.
In this nationwide retrospective study, we report that a large number of patients do not comply with treatment guidelines. Since the area of residence was identified as the main risk factor for failing to receive the loading dose, we think distance to anti-VEGF delivering facilities should be seriously taken into account when defining global policies relating to retinal care.
Age-related macular degeneration, Anti-VEGF, Bevacizumab, Compliance, Intravitreal injections, Loading dose, Treatment regimen
For more than a decade, anti-vascular endothelial growth factor (VEGF) therapy is the standard treatment for neovascular age-related macular degeneration (AMD) [1]. Ranibizumab [2-14], bevacizumab [2,4,8,9,11,12,15] and more recently aflibercept [16] have all been extensively studied in large, multicenter, double-masked, prospective studies. For those three agents, a loading dose is recommended, consisting of three-monthly intravitreal injections [1,17,18].
In the public health system in Israel, patients diagnosed with neovascular AMD are offered bevacizumab as a first line agent, in accordance with the conclusions of major studies comparing treatment outcomes when starting with one or the other of those molecules [2,4,8,9,12,16,19]. The first three monthly injections are considered as standard of care and, according to clinical guidelines, should be delivered to any patient diagnosed with neovascular AMD [1,17,18]. Attempts to shorten or extent the interval between the first injections have raised efficiency and safety concerns [20,21]. Repeated ocular injections undoubltly represent a burden for the patients [22].
It is known from other conditions that invasive treatment, planned to be iterative, is associated with compliance issues [23-27]. The compliance of neovascular AMD patients to therapy in real life has been poorly studied [28,29].
In this study, we aim to evaluate the proportion and characteristics of patients diagnosed with neovascular AMD who do not complete the bevacizumab loading dose.
This retrospective, population-based analysis accessed data from the electronic medical records of all individuals affiliated with Clalit Health Services who received intravitreal injections of bevacizumab for treatment of AMD between September 2008 and October 2014.
Clalit Health Services maintains a chronic disease registry database that includes information collected from a variety of sources: primary care physician reports, medication-use files, hospitalization records, and out-patient clinic records. The methods of registry acquisition and maintenance were described elsewhere [30].
For all individuals included in the analysis, we extracted information from the registry regarding the following conditions: anxiety, depression, alcohol abuse, transient ischemic attack, cerebrovascular accident, congestive heart failure and myocardial infarction.
Additional information extracted from patients' files included age, gender, place of residency (living in urban (> 10,000 inhabitants) or rural (< 10,000 inhabitants) areas, marriage status, and social security economic status (indicating members that are exempt from paying social security tax because of a low-socioeconomic status). The date of death was automatically communicated from the Israeli Interior Ministry via the unique national identity number. The cause of death was not recorded.
In those nationwide records, we isolated patients aged of 60 years or more treated for neovascular age-related macular degeneration, excluding patients whenever a doubt subsisted on the nature of the indication. 47 patients were excluded because it was not possible to eliminate diabetic macular oedema as the indication for injections; 29 since high myopia could not be ruled out as the cause of choroidal neovascularization; 18 as the reason for treatment may have been a concomitant diagnosis of retinal vein occlusion; in 4 patients, inflammatory conditions were identified as the possible etiology of choroidal neovascularization. We then separated patients with less than three injections from those having completed the initial course. We excluded patients who received only three injections over more than 100 days. At that point, we considered two groups: patients after three or more injections (the three initial injections delivered within 100 days) and patients who received less than three injections.
For each group, we excluded patients having passed away during the follow-up period, after characterizing them. We compared both groups of patients living at the end of follow-up in terms of baseline demographics, baseline conditions known to affect compliance [19,31-34], number of injections and overall frequency of injections. We also analyzed the occurrence, after initiation of anti-VEGF therapy of conditions indicating a deteriorated general health and therefore lesser ability to pursue regular retinal treatments [19].
Ethics approval was obtained from the Ethics Committee of the Clalit Health Services.
Student's t-test was used to analyze continuous variables, and the chi-squared test for proportions. The threshold for significance was p < 0.05. Odds ratio were calculated, when relevant, with a confidence interval of 95%.
On 5638 patients (mean age at first injection ± SD: 80.3 ± 8.9 years, 2489 males) having received unilateral or bilateral injections of bevacizumab only, (sum of all injections: 42128), 1003 (17.8%) received less than three injections.
Among the patients who did not receive all three initial injections, 47.2% had received only one injection, 52.8% two. Of the patients who received two injections at all, the interval between both injections was longer than 80 days in 114 patients (11.4% of all patients having received less than three injections). We identified 252 patients who received three injections only, within a longer period than 100 days. This means that 22.3% (1255/5638) of all patients who started bevacizumab therapy did not fulfill the loading dose within 100 days.
We excluded from further analysis patients with three injections over more than 100 days. At the end of the observation period (73 months), 306 of the patients who had received less than three injections within 100 days had passed away (mortality: 30.5%), while in the same period 884 patients deceased after receiving three injections or more (mortality: 20.2%) (OR = 2.24, CI: 1.91 - 2.61, p < 0.001).
Of all the patients living at the end of follow-up (n = 4196), 16.6% (n = 697) did not fulfill induction within 100 days (patients who received only three injections over more than 100 days were not taken into account furthermore) (Figure 1).
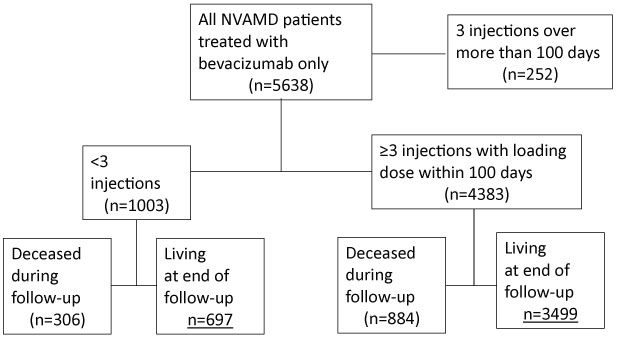 Figure 1: Study flowchart. Of all patients having received bevacizumab for neovascular AMD (NVAMD), we generated two groups, based on the number of injections. For each of those group, mortality at the end of follow-up was calculated. We then compared both groups of survivors. View Figure 1
Figure 1: Study flowchart. Of all patients having received bevacizumab for neovascular AMD (NVAMD), we generated two groups, based on the number of injections. For each of those group, mortality at the end of follow-up was calculated. We then compared both groups of survivors. View Figure 1
Surviving patients having completed the loading dose received a mean (± SD) of 9.68 (± 9.14) bevacizumab injections over a mean period of 18.3 (± 18.6) months (mean ± SD interval between injections: 55.6 ± 50.6 days). Patients, living at the end of follow-up, who failed to complete the loading dose were younger than patients with three or more injections (79.8 vs. 80.7 vs. years, p < 0.001).
Residing in rural areas was associated with a significantly higher likelihood of not completing the loading dose (OR = 1.54, CI: 1.23-1.92, p < 0.001) (Table 1). Gender, marital status and baseline conditions such as congestive heart failure (CHF), status post cerebrovascular accident (CVA)/transient ischemic attack (TIA), status post myocardial infarction (MI), anxiety and depression were not significantly associated with a risk of failing to achieve induction.
Table 1: Baseline differences between patients who did not receive the loading dose of bevacizumab and those who did. View Table 1
In the group failing to achieve induction, we did not detect a higher incidence, between the first injection and end of follow-up, of TIA/CVA, MI or CHF (Table 2).
Table 2: Incidence of major cardiac and cerebrovascular events after initiation of bevacizumab treatment, difference between patients achieving induction or not. View Table 2
Among patients started with bevacizumab therapy, given as first line treatment for neovascular AMD, we found that 22.3% of them failed to receive the loading dose within 100 days and that 17.8% received less than three injections.
Mortality was higher in patients not fulfilling induction. It could be assumed that those deceased patients had an initial poorer general health than patients able to comply to the anti-VEGF guidelines. Another worrying explanation could be that some patients are proner to develop fatal complications of bevacizumab intraocular injections and would decease after only one or two injections. When considering all patients living at the end of the follow-up, 16.6% had not received the loading dose within 100 days. We found a larger proportion of rural residents in patients who failed induction than in those who received three injections or more.
Regarding other conditions possibly lowering compliance, we did not observe any significant difference between the two groups. We neither find a significant difference between both groups in the occurrence of major cerebrovascular or cardiac events after the first injection. So, we can assume that patients, living at the end of follow-up, whether receiving or not the loading dose, share a similar health profile.
To our knowledge, this is the first-time adherence to anti-VEGF therapy is assessed on such a large scale, under real-life conditions.
As a retrospective study that draws clinical data from an HMO database, this study has inherent weaknesses. However, it can be admitted that the HMO database was complete regarding the diagnoses and therapies: registration of ophthalmologic conditions is based on multiple visits, registration of chronic diseases is considered to be sufficiently solid [30], the HMO reimburses bevacizumab intraocular injections, given as first line therapy (so there is no interest for the patients to receive bevacizumab therapy outside the HMO). Fatal events would have been registered even for patients passing away after leaving the HMO. The design of our study does not enable us to establish more precisely the reasons underlying failure to adhere to guidelines. Another weakness of this research is that the electronic medical records on which it is based do not differentiate between unilateral and bilateral intravitreal injections. Information on visual acuity is also lacking. Patients receiving bevacizumab injections in a poorly seeing eye while the fellow eye enables preserved overall vision might show lower compliance than patients treated in their relatively good eye. Our data do not provide us insight of such a resolution. Another weakness of our data is that the cause of death is not available. Another design would be necessary to investigate more specifically the group of patients, excluded from our analysis, who received three injections over a longer period than 100 days.
In this nationwide retrospective study, we report that a large number of patients do not comply to treatment guidelines. Failure to receive the loading dose is alarming in itself [35]. In terms of functional repercussions, as well as global social cost, the natural history of neovascular AMD is grim [36]. Moreover, failure to receive the initial three bevacizumab injections should certainly be considered as an indicator of more widespread non-adhesion to clinical guidelines [37].
The importance of adhering to long term follow-up and iterative injections should be explained to patients newly diagnosed with neovascular AMD and the consequences of not doing so should be clearly stated. Improving communication between the retina specialist and his patient is crucial but it does not dispense the health system to be evaluated on a macroscopic level. We identified the area of residence as the major risk for failing to receive the loading dose. In comparison to other countries, Israel is small and access to clinics delivering bevacizumab relatively easy. Our results suggest that distance from home to facilities providing intraocular anti-VEGF injections should be taken into account when assessing the global efficiency of retinal care. Prospective studies on which the current protocols for treating neovascular AMD rely are not designed to evaluate compliance in real life.
In view of the repercussions of suboptimal treatment of neovascular AMD, we advocate registering anti-VEGF administration on a national and transnational scale and using the data to formulate general health guidelines that would ensure equitable access to retinal care.