This report describes a case of APMPPE after an Influenza vaccine in an adult and followed by a facial palsy.
A 25-year-old man was admitted to the ophthalmology department because of painless blurred vision on the right eye over two weeks. The patient worked as a soldier and the symptoms started three weeks after having a seasonal anti-flu immunization. The medical chart review and the ancillary investigation disclosed the cause of the visual impairment.
The patient was treated with prednisolone 100 mg intravenous. After three months the patient had also a facial palsy. Therefore, we did a cerebral Magnetic Resonance Imaging (MRI). There were no pathological findings.
Previous case reports already suggested a possible relationship between various immunizations and APMPPE onset. More studies are required to link APMPPE occurrence and vaccination and disclose the relationship and the risk.
Gass first described acute posterior multifocal placoid pigment epithelium (APMPPE) fluorescein angiography findings with bilateral central vision loss in 1968. The etiology of APMPPE is till now unknown. However, it could be secondary to a delayed-type of hypersensitivity-induced occlusive vasculitis [1]. There is a strong association with HLA-B7 and HLA-DR2 genetic haplotypes [2,3]. There is also an association with infection and autoimmune disease [4]. Cerebral vasculitis is a strongly associated. And CNS imaging should be done in patients with associated neurological symptoms [3].
The pathogenesis of the disease is controversial. A prevailing theory suggests that a primary affectation of the choriocapillaris leads to secondary injury of the RPE and outer retina. As a result, occurs an atrophy of the choriocapillaris, RPE, and photoreceptors. So actually, the choroidopathy may be a more appropriate name than epitheliopathy [5].
The usual clinical presentation is subacute bilateral visual impairment. Visual acuity can range from 20/40 to count-fingers neurological symptoms, such as sensorineural hearing loss and headache [3,6].
Anterior uveitis is rare. Vitritis is usually very mild [7]. Fundoscopic examination shows multiple bilateral creamy yellow-white placoid lesions. These lesions are at the level of RPE, typically found posterior to the equator [3,7].
The active lesions show in Fluorescein Angiogram (FA) early hypofluorescence corresponding to the placoid lesions then followed by irregular hyperfluorecent staining at the late frame.
The explanation for the hypofluorescence at the early FA frame may be due to poor perfusion of the choriocapillaris. The late hyperfluorescence may be because of vascular leakage. The hyperfluorescence resolves in subacute or healed lesions [3,8].
APMPPE is a self-limiting disease, about ¼ the patient had a visual acuity of 20/50 or worse [3,5].
A 25-year-old man was admitted to the ophthalmology department because of painless blurred vision on the right eye over two weeks.
He was otherwise healthy, and he had no complaints on the left eye. He works with the army. He had no foreign mission for the past months. The symptoms started three weeks after having a seasonal anti-flu immunization.
Visual acuity (BCVA) was 0.8 (0.1 Log MAR) in the right eye and 1.2 (-0.1 Log MAR) in the left eye. The anterior segment of both eyes revealed no signs of inflammatory reaction. There were also no vitreous cells. Dilated fundus examination revealed multiple bilateral creamy yellow-white placoid lesions on both eyes (Figure 1). The visual field shows a central scotoma only on the right eye (Figure 2).
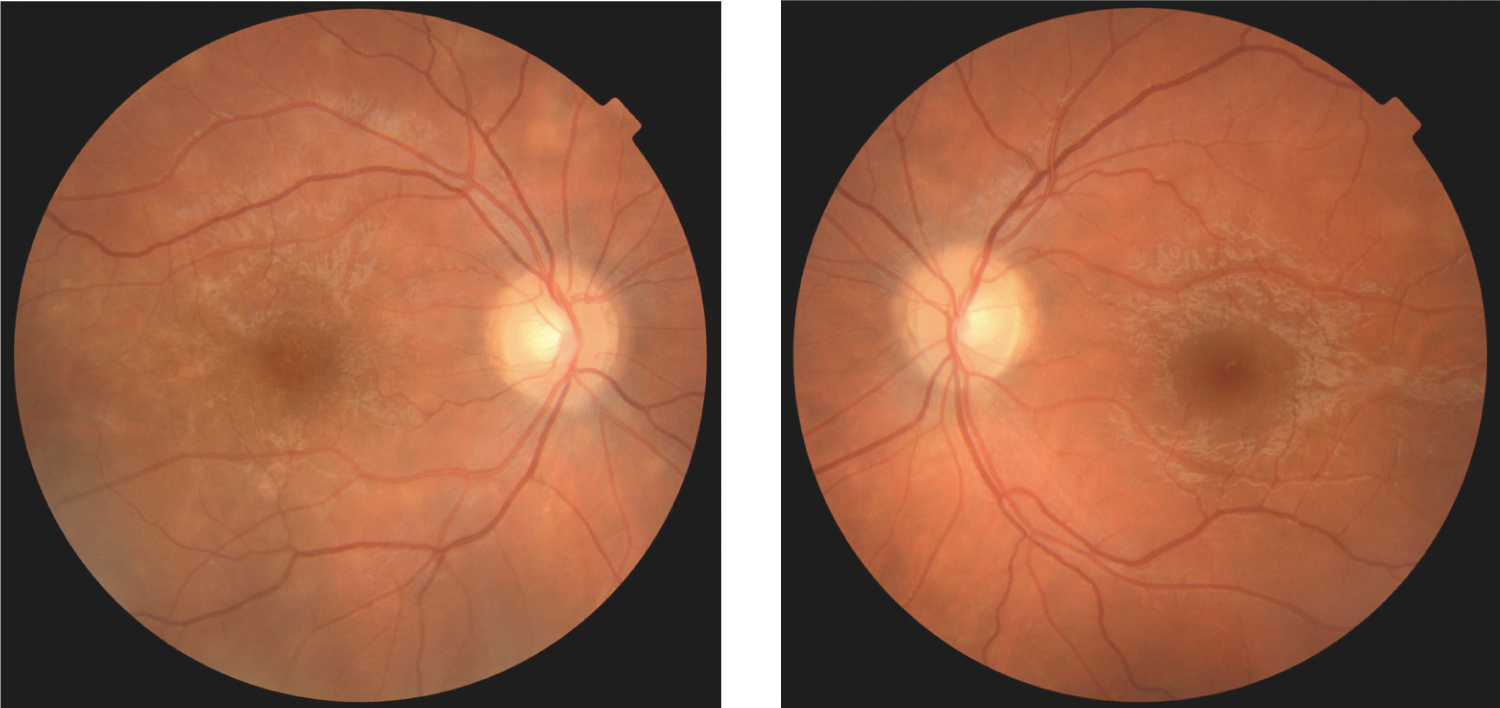 Figure 1: Fundus photo show multiple bilateral creamy yellow-white placoid lesions on both eyes.
View Figure 1
Figure 1: Fundus photo show multiple bilateral creamy yellow-white placoid lesions on both eyes.
View Figure 1
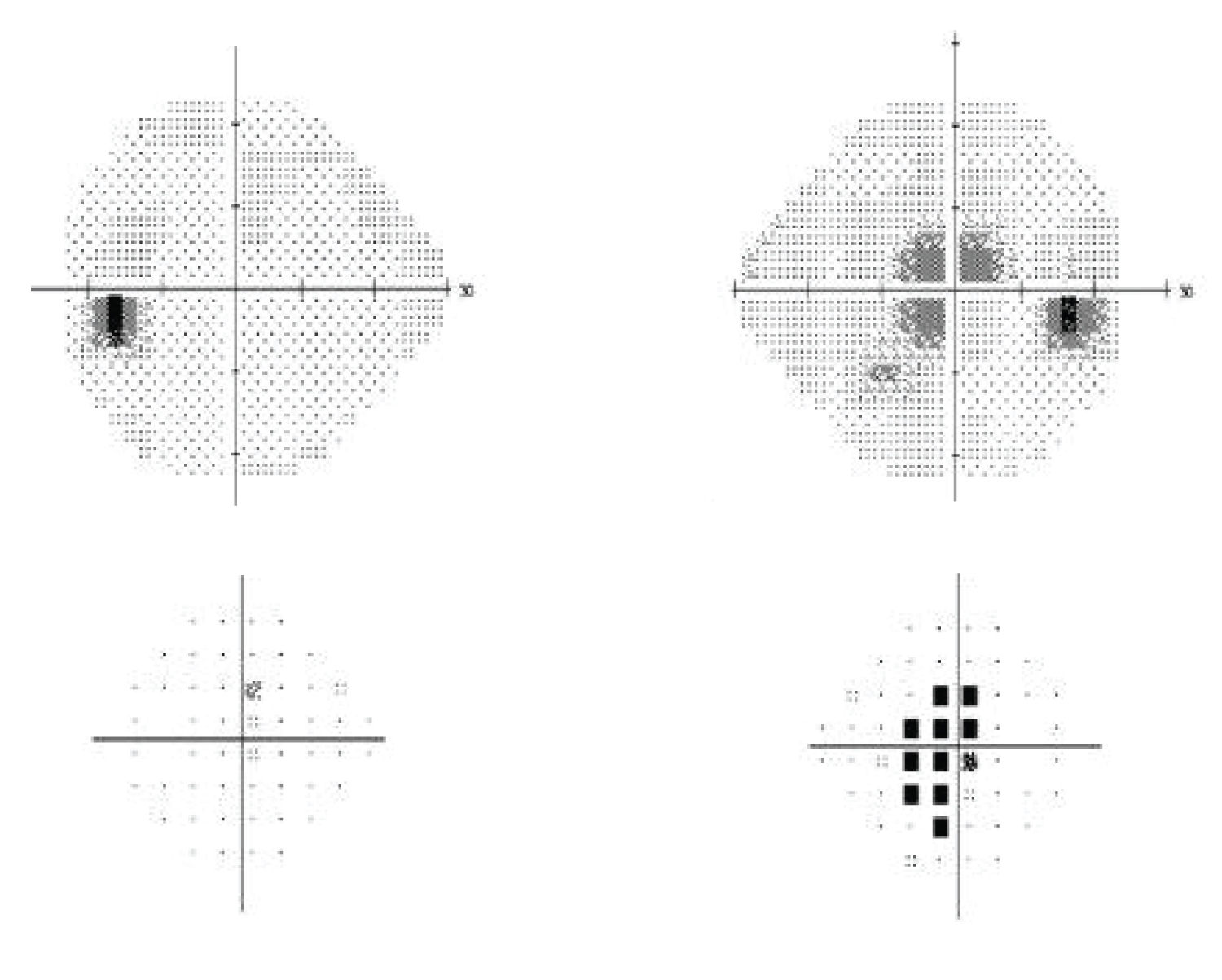 Figure 2: Visual field of the right eye revealed central scotoma (to the right), Visual field of the left eye with no scotoma (to the left).
View Figure 2
Figure 2: Visual field of the right eye revealed central scotoma (to the right), Visual field of the left eye with no scotoma (to the left).
View Figure 2
The Fluorescein angiogram (FA) shows on both eyes early hypofluorescence corresponding to the placoid lesions then followed by irregular hyperfluorescent staining at the late frame (Figure 3).
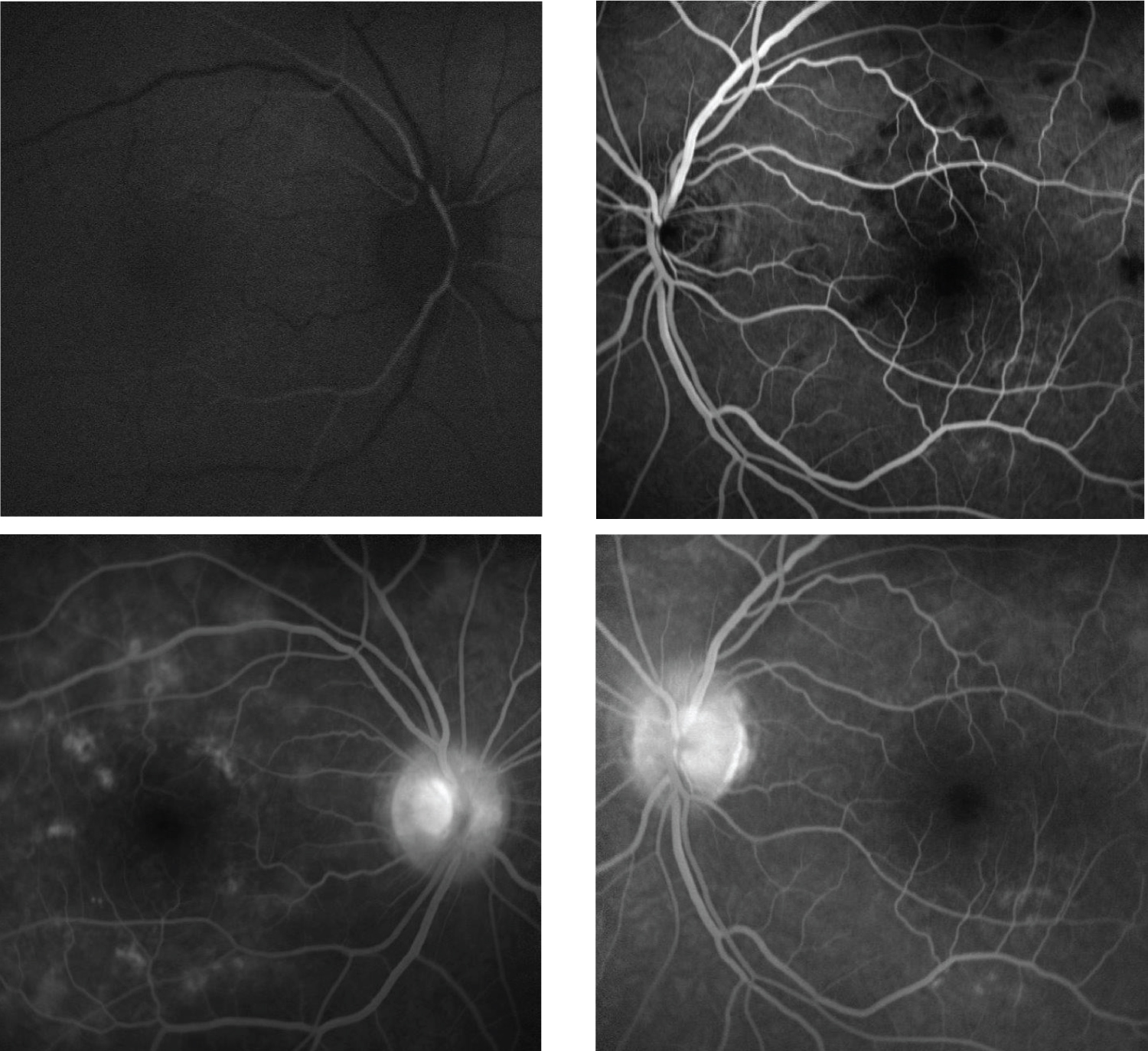 Figure 3: FA at the acute phase shows on both eyes early hypofluorescence (the upper pictures) corresponding to the placoid lesions then followed by irregular hyperfluorescent staining at the late frame (the lower pictures).
View Figure 3
Figure 3: FA at the acute phase shows on both eyes early hypofluorescence (the upper pictures) corresponding to the placoid lesions then followed by irregular hyperfluorescent staining at the late frame (the lower pictures).
View Figure 3
The Indocyanine green angiography (ICGA) shows non-perfusion of the choriocapillaris corresponding to the placoid lesions on both eyes (Figure 4).
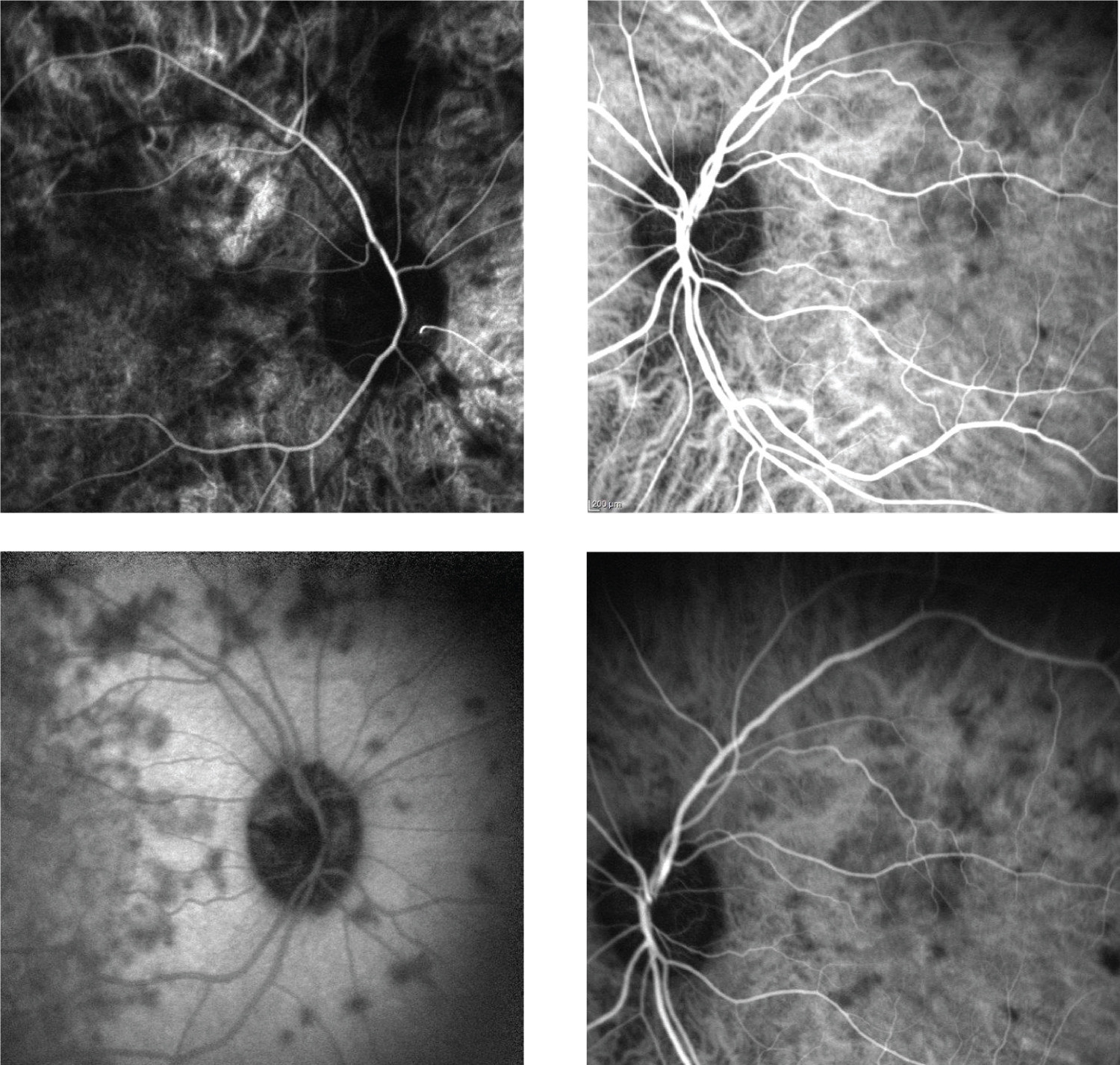 Figure 4: (ICGA) at the acute phase shows non-perfusion of the choriocapillaris corresponding to the placoid lesions on both eyes.
View Figure 4
Figure 4: (ICGA) at the acute phase shows non-perfusion of the choriocapillaris corresponding to the placoid lesions on both eyes.
View Figure 4
We found in the systemic assessment no infection or systemic inflammatory marker. Systemic therapy with 1 mg/kg Prednisolon for 3 days then tapering the therapy revealed an increase of the visual acuity of the right eye to 1.0 (0.0 Log MAR).
After five months comes the patient with a facial palsy that has been occurring over 2 weeks on the left side. The facial palsy was treated successfully with Prednisolone. There was a complete regression of the fundus signs. However, a residual spot of non-perfusion of the choriocapillaris was still shown on the ICGA (Figure 5).
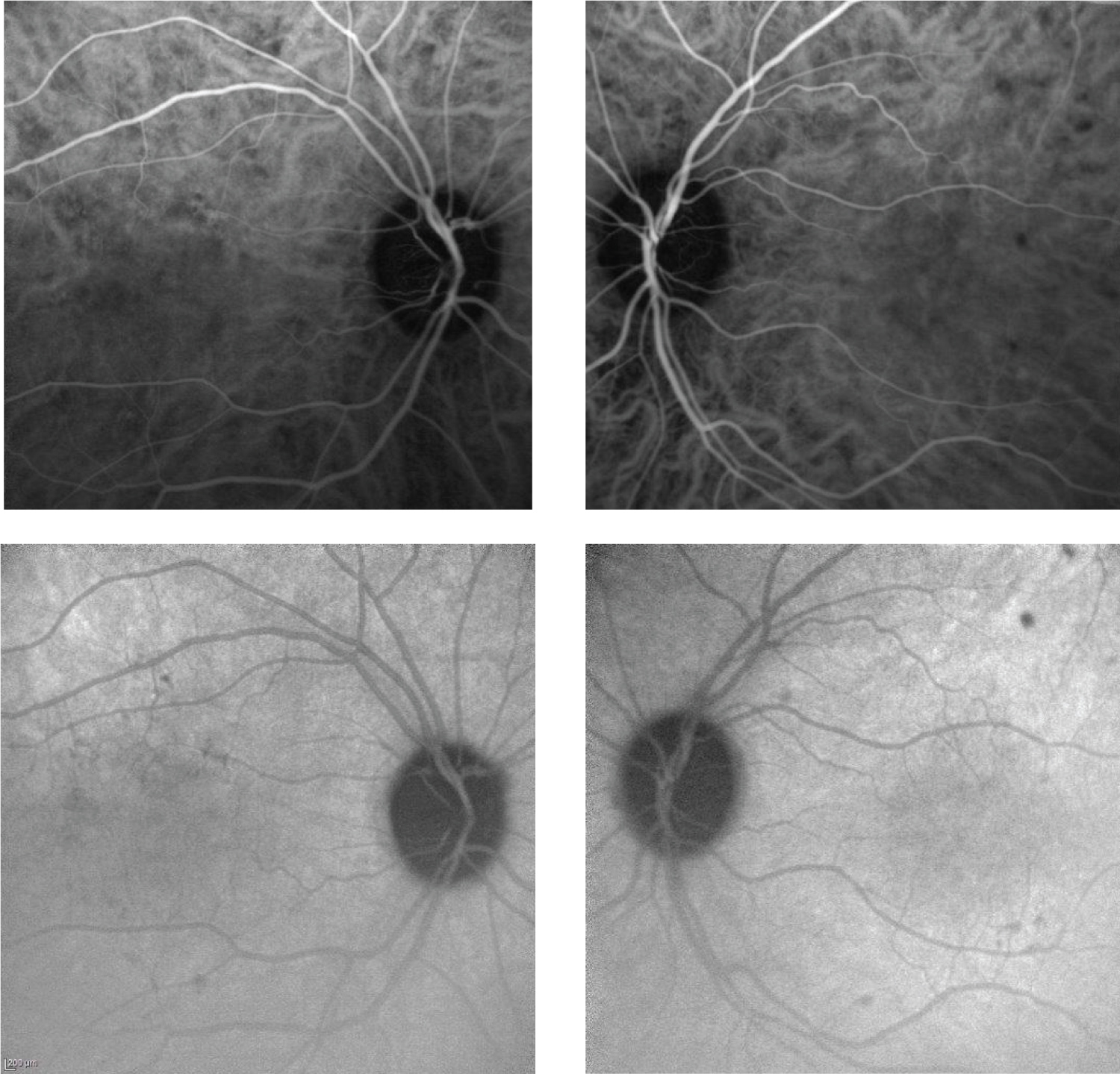 Figure 5: ICGA shows residual spots of non-perfusion of the choriocapillaris after 5 Months.
View Figure 5
Figure 5: ICGA shows residual spots of non-perfusion of the choriocapillaris after 5 Months.
View Figure 5
Because of the facial palsy, a cerebral MRT was performed. There were no pathological findings.
Previous case reports already suggested a possible relationship between various immunizations and APMPPE onset. This is the first reported case of APMPPE followed by facial palsy after anti-flu immunization. More studies are required to link APMPPE occurrence and vaccination and disclose the relationship and the risk.