Avoidable severe visual sequelae are prevalent among highly myopic eyes. We analyzed the postoperative incidence of myopic traction maculopathy (MTM) progression and long-term postoperative structural and functional findings after macular surgery for myopic foveoretinal detachment (FRD).
A retrospective, consecutive, comparative, interventional, one-surgeon, multicenter control case series was conducted on 35 highly myopic eyes of 31 patients who underwent fovea sparing internal limiting membrane removal technique for myopic FRD between October 2016 and April 2020. Long-term postoperative SD-OCT and functional follow-up evaluations with microperimetry, chromatic campimetry and multifocal electroretinography were performed. The main outcome was the incidence of surgical success and progression of myopic FRD.
The mean evolution time of myopic FRD was 6.2 ± 3.5 months. The mean follow‑up time was 23.9 ± 12.1 months. The mean time for the myopic FRD resolution was 5 ± 2.1 weeks. Using a paired-samples permutation test, we found that surgery was associated with a significant improvement in visual acuity: BCVA (in logMAR) decreased from 0.87 ± 0.15 pre-surgery to 0.48 ± 0.52 logMAR, with P = 0.00075.
Thirty-two eyes (91.4%) showed resolved myopic FRD. Three eyes (8.5%) showed progression: Two (5.7%) developed a full-thickness macular hole, and one (2.8%) developed a macular hole retinal detachment.
Postoperative test results revealed retinal sensitivity abnormalities in 10-2 and 30-2 visual-field examinations in 18 of 19 eyes (94.7%) examined; 16 of 17 eyes (94.1%) tested showed an abnormal response on microperimetry with a stable foveocentral fixation pattern, and 20 of 21 eyes (95.2%) tested showed a profound reduction in N1- and P1-wave amplitudes.
Results showed a high incidence of microstructural regression (91.4%) with low incidence of MTM structural progression after surgery (8.5%). Long-term structural and functional evaluations revealed an abnormal macula.
Foveoretinal detachment, Microperimetry, Myopic traction maculopathy, Multifocal Electroretinography, Multimodal functional evaluation, Visual field testing, Macular surgery
High myopia is a major cause of legal blindness in industrialized countries [1]. In the United States, it affects nearly 2% of the general population aged between 12 and 54 years [2]. Pathological myopia is the fifth-leading cause of low vision or blindness in Japan and the second-leading cause among people aged over 40 years in China [3]. High myopia is defined as a refractive error with a spherical equivalent > -6.0 diopters or an axial length > 26.5 mm, while pathological myopia is currently defined as the presence of progressive posterior pole chorioretinal, and vitreoretinal tissue damage associated with posterior scleral stretching and posterior staphyloma (PS) development. Pathological macular changes in high myopic eyes are characterized by retinal atrophy, ruptures in Bruch's membrane, and sclerotic thinning [4].
The progressive increase in axial length from alterations of the scleral connective tissue, together with the presence of epiretinal membranes (ERMs), and vascular rigidity give rise to early tractional changes resulting in myopic foveoschisis (MF), followed by an advanced and progressive form of myopic foveoretinal detachment (FRD) [5]. Scleral thinning and localized ectasia due to a reduction in the thickness of individual collagen fibers have been observed in postmortem myopic eyes [6].
Myopic traction maculopathy (MTM) is a relatively new term for tissue tractional mechanical changes found in highly myopic eyes. The term MTM was coined by Panozzo and Mercanti [7], who used optical coherence tomography (OCT) to describe foveomacular changes, such as ERM or vitreomacular traction, foveomacular internal or external schisis-like thickening, FRD, lamellar or partial-thickness macular holes (MHs), myopic full-thickness MH with or without retinal detachment, and PS. In addition, enhanced depth imaging OCT has revealed choroidal thinning in the macular region as an age-related degenerative change described in high myopia [8].
Myopic foveoschisis, which is the early stage in MTM, is present in approximately 9-34% of patients with pathological myopia. It is consistent with a slow, progressive, vitreomacular, tractional schisis-like thickening of the retina, and was recently described as the tractional elongation of the Henle nerve fiber layer rather than a splitting of the retina in eyes with high myopia and PS [5]. This phenomenon has a prevalence of 66% among female patients [7,9]. MF was first identified by Takano and Kishi in 1999 based on OCT cross-sectional views and is found in 34% of highly myopic eyes with PS [6-13].
Highly myopic eyes with macular or foveal retinoschisis and FRD naturally progress to form MH [12,14]. Although MF as the early stage of MTM may remain stable over a long period of time, it slowly progresses to form FRD or MH with or without macular hole retinal detachment (MHRD) as a part of its natural history.
Tractional forces play an important role in the pathogenesis of MTM, especially when combined with PS [15]. The specific cause of foveoschisis is not fully understood. In one proposed mechanism for its pathogenesis, the axial traction generated by the progressive elongation of the eyeball produces the subsequent stretching force on the posterior retina [10,11]. The premacular vitreous cortex with tangential traction may be secondary to the rigidity of the internal limiting membrane (ILM) and retinal vessels [11].
There are multiple published classification and grading systems for MTM. Shimada, et al. [12] classified and defined MTM according to extent and location relative to the fovea using OCT. The META-PM study group proposed an international photographic classification and grading system for MTM using fundus photographs, and its application is increasingly being considered [15]. The ATN classification and grading system quantifies MTM based on atrophic pathological changes (A), tractional vitreoretinal pathological macular changes (T), and neovascularization pathological submacular changes (N). It has been validated [16], and some reports have described its use for surgical decision-making [17]. However, published data on long-term functional results of myopic FRD surgery is sparse. For this reason, we selected surgical cases that met criteria designed to minimize possible confounding variables. Thus, we selected cases who were treated successfully with vitrectomy and an uncomplicated fovea sparing ILM peeling technique. This study aimed to analyze the long-term structural and functional outcomes after fovea sparing ILM Peeling technique for myopic FRD, and the postoperative incidence of MTM progression.
The retina department at the Instituto de Oftalmologia Hospital, Retina Specialists at the American British Cowdray Hospital, and Juarez Hospital in Mexico City provided authorization and released the patients' electronic clinical records to generate the database used in this study. This retrospective study was approved by the three institutional review committees (no approval or reference number is provided for retrospective studies by the institutions in Mexico City). Written informed consent was obtained from all patients in accordance with the institutional guidelines. Data are available from the imagenology and psychophysics laboratory at the retina department of the three institutions.
A total of 35 eyes of 31 consecutive patients who had undergone vitrectomy with successful and uncomplicated macular surgery with the fovea sparing ILM surgical technique for symptomatic myopic FRD, and 22 eyes that fulfilled the diagnosis of myopic FRD that had undergone classical ILM removal were selected and retrospectively analyzed at the Retina Service of the three participating Institutions from October 2016 to April 2020. Study group: A three-port pars plana vitrectomy was performed in these symptomatic and highly myopic eyes with evidence of a progressive decrease in BCVA. All the selected eyes had an axial length > 26.5 mm, with no evidence of patchy foveal-affected chorioretinal atrophy, diffuse macular chorioretinal atrophy, or quiescent or active myopic choroidal neovascularization according to the ATN classification [16]. The diagnosis of myopic FRD traction maculopathy was confirmed by SD‑OCT findings consistent with central submacular presence of subretinal fluid, internal or external schisis-like foveomacular thickening, presence or absence of ERM and residue of hyaloidal cortical remnants, and no evidence of partial or full-thickness MH on the SD-OCT examination. Only patients with a follow-up period of at least 4 months were statistically analyzed. All eyes were followed-up in a standardized fashion at the three institutions every month for more than 6 months and then examined every 6 months until the last follow-up visit. Follow-up durations ranged from 4 to 43 months, with a mean of 23.86 months (12.10 months standard deviation).
Control group: N = 22 eyes that underwent classical ILM removal technique were used as controls in order to evaluate the effectiveness of the modified fovea sparing ILM removal tailored by the author. Individuals were matched on age, sex, study period, and follow-up period (Table 1). The inclusion/exclusion criteria, three referral institutions and the surgeon were the same across groups.
Table 1: Myopic FRD patients' general and demographic data. View Table 1
All patients underwent a general ophthalmic standardized evaluation and preoperative examinations, including a regular Amsler test, BCVA assessment, biomicroscopy slit-lamp examination, fundus examination with panfundoscopic contact lens, and indirect ophthalmoscopy. Neither preoperative multifocal electroretinography (mfERG) examinations nor microperimetry examinations were performed due to the remarkable presence of submacular fluid, symptomatic myopic FRD with significant vision loss, and lack of preoperative central clinical stable fixation patterns.
Cross-sectional images of the macular region were acquired along the horizontal plane through the foveal center using SD-OCT (RTVue-XR platform SD-OCT, Optovue, Inc.; Fremont, CA, USA), and the axial lengths were measured using partial coherence laser interferometry (Zeiss IOL Master 700; Carl Zeiss Meditec, AG; Oberkochen, Germany).
The presence of PS in both groups was confirmed by B-scan ultrasonography (A and B Ultrasound Unit. Quantel Medical. Du Bois Loli; Auvergne, France) and indirect ophthalmoscopy.
A postoperative microstructural evaluation (mean final evaluation at 23.9 ± 12.1) was performed using SD-OCT (Spectralis OCT, Heidelberg Engineering; Heidelberg, Germany) and the swept-source DRI OCT Triton device (Topcon Medical Systems, Inc., Oakland, USA), while postoperative multimodal functional evaluations were conducted with BCVA and conversion in logarithm of the minimum angle of resolution (logMAR) units, 10-2 and 30-2 automated chromatic central field examination (Visual Field Perimeter, Model MonPackONE, Vision Monitor by Metrovision; France), macular microperimetry (MP-3 MAIA Confocal Microperimeter by Metrovision; France), and mfERG testing (Electrophysiology Vision Monitor Analizer, Model MonPackONE by Metrovision; France).
The functional evaluation included the final BCVA in logMAR units, macular retinal sensitivity (MRS), foveal retinal sensitivity (FRS), and retinal sensitivity analysis mapping assessed by microperimetry. The latter was performed by using the standard MAIA examination protocol covering a 10° diameter area with 37 measurements points and a light stimulus projected directly over the macula surface, with a size stimulus of Goldman III, background luminance of 4 asb and maximum luminance of 1000 asb, and a 36-dB dynamic range. Fixation stability and fixation location pattern parameters were assessed by tracking eye movements 25 times/second and plotting the resulting distribution over the scanning laser ophthalmoscope image. Each movement was represented by a point, and the overall site described the preferred retina locus.
Computerized mfERG was used to detect focal (regional) outer macular abnormalities as indexed by the amplitude and implicit time of the N1 wave, and the implicit time of the P1 wave. Elevation electroretinography 3-D maps were assessed in the affected eye and compared to the normal contralateral eye or to the corresponding age and population control normative dataset of the laboratory institution. The 61-hexagon 30º standardized technique was performed to test the macular electrical multifocal outer layer sensitivity, point to point, at the < 2-degree to > 15-degree central rings (< 2, 2-5, 5-10, 10-15, > 15 central rings) at the last follow-up evaluation visit.
A standard 25-gauge three-port pars plana vitrectomy was performed by one of the authors (MAQR) in all eyes under local anesthesia plus sedation. In addition to core vitrectomy, triamcinolone acetonide-assisted (Kenalog 40 mg/mL; Bristol-Myers, New York, NY) removal of the cortical vitreous from the surface of the retina was performed using a silicone-tipped cannula and active suction, paying special attention to achieve a free and mobile posterior hyaloid membrane and leave the superficial foveal tissue (foveal roof) untouched. The surgeon's personal technique was standardized: surgical macular evaluation and revision were performed in all cases by using trypan blue 0.15% ophthalmic solution (Membrane Blue; Dutch Ophthalmic USA) as an adjuvant dye to stain cortical vitreous remnants or ERMs. As a second-step macular surgery, 0.15 mL of a 0.25 mg/mL (0.025%) diluted isomolar solution (pH 7.4) of Brilliant Blue G (BBG) dye was used to selectively stain the ILM and manipulate it carefully to accomplish an adequate fovea-sparing surgical ILM removal, without peeling the dyed foveocentral ILM; in most cases, the ILM was found to be fragmented and easy to peel off, leaving the fovea untouched, with its corresponding foveocentral ILM, as mentioned above. Only eyes in which this technique was completed and uncomplicated were included in this study. This procedure was performed using a 25-gauge vitrectomy cut and suction instrument (Alcon Constellation Vision System, Alcon Labs; Fort Worth, Texas, USA) and 25-gauge 0.44 ILM forceps (Grieshaber Revolution DSP ILM forceps; Alcon Labs; Fort Worth, Texas, USA) along with a 25-gauge Finnesse ILM flex loop microinstrument (Grieshaber, Alcon labs, Fort Worth, Texas, USA) to facilitate ILM flap manipulation. A non-expandable bubble with 15% of a perfluoropropane gas mixture was used as a long-acting tamponade. In 12 phakic eyes, phacoemulsification followed by intraocular lens implantation was performed, and the lens status was not considered as a variable in the postoperative analysis. In the control group, the classic technique of ILM peeling technique consisting of staining and removal of the ILM from macular vascular arcade to vascular arcade was performed, making sure not to leave remnants of ILM on the foveal surface, only the eyes without transurgical complications with this technique were included.
The primary outcome was fully resolved myopic FRD using a modified ILM removal technique that aims to avoid irreparable damage associated with late-stage MTM. The examined variables were absence/presence of progression to MH/MHRD, and macula status. The secondary outcomes were the long-term final postoperative BCVA and its associations with SD-OCT, campimetric, mfERG, and microperimetry findings.
The data were analyzed using SPSS v.28 for Windows and R v.4.0.4 for Windows software.
Pre-post change in BCVA logMAR values was evaluated using a two-tailed paired-samples permutation test (20,000 permutations), a statistical approach that has an advantage over a t-test when distributions are skewed. This analysis was performed in jmuOutlier for R [18] for the Study and the Control groups separately and enabled inferences about the presence and magnitude of change in preoperative to postoperative visual acuity.
Comparisons with the Control sample were carried out as follows. For categorical outcomes (progression to MH/MHRD, macula status post-op), association testing with the Group status was performed using Pearson's X2 test; empirical P-values were obtained via a Monte Carlo simulation (20,000 replicates). For continuous outcomes, we adopted a two-pronged strategy. First, we performed a permutation test on the BCVA logMAR difference values (Post minus Pre), directly testing the group differences in the magnitude of change over time. To further quantify this effect, we also calculated and compared the effect size estimates using Hedges' g with correction for sample non-independence, as implemented in effsize for R [19].
The patients' general and demographic data are listed in Table 1.
The mean preoperative evolution time of FRD was 6.2 ± 3.5 months. The mean postoperative time for the myopic FRD resolution was 4.9 ± 2.1 weeks. To determine whether surgery outcomes correlated with the macular alterations observed on the OCT, the postoperative BCVA was measured and compared between 20 eyes (57.1%) with normal and 15 eyes (42.9%) with abnormal OCT results. A one-sided permutation test found only tentative statistical evidence (P = 0.07885) for the difference in the BCVA between those who had an abnormal and those with normal OCT. A summary of preoperative and postoperative structural findings is presented in Table 2.
Table 2: Study group: Summary of preoperative and postoperative structural findings (n = 35 eyes). View Table 2
The mean preoperative BCVA was 0.87 ± 0.15 logMAR, and the mean postoperative BCVA was 0.48 ± 0.52 logMAR. A paired-sample permutation test established that this difference was statistically significant (P = 0.00075), indicating that the surgery resulted significant improvement in the final postoperative BCVA.
In contrast, our analyses of the Control group of eyes did not establish a significant shift in BCVA logMAR values post-surgery (from 0.89 ± 0.15 logMAR to 0.87 ± 0.71; P = 0.8634). A formal comparison of the magnitude of change between the two groups was carried out using change scores as the outcome. Using a two-sample permutation test, we found that magnitude of change indeed differed significantly between the two group (P = 0.04975): this difference was also evident in the difference in formal effect size estimates obtained for the Study group (Hedges' g = 1.02, 95% CI from 0.27 to 1.01) and that of the Control group (g = 0.05, 95% CI from -0.40 to 0.48), corresponding to a large and very small effect, respectively.
Further postoperative multimodal functional evaluation was performed on a subset of eyes. Microperimetry analysis was completed for 17 of 35 (48.5%) of Study group eyes, the 10-2 and 30-2 visual field tests were completed for 19 of 35 eyes (54.2%) of Study group eyes, and mfERG was completed for 21 of 35 (60%) of Study group eyes.
The 10-2 and 30-2 visual field test results indicated a significant decrease in macular sensitivity with a preserved color discrimination on chromatic evaluation, and the mfERG results indicated variability in the degree of abnormality in the outer retinal and photoreceptors in 20 of 21 eyes (95.2%). Chromatic campimetry, selectively performed to detect photoreceptor damage, indicated no selective damage in some specific cone systems; only significant decrease in macular sensitivity was observed. A summary of postoperative multimodal functional evaluation is listed in Table 3.
Table 3: Study group: Postoperative multimodal functional evaluation (n = 35 eyes). View Table 3
Post-operative BCVA in logMAR in the study group was not associated with post-operative mfERG (P = 0.14075), microperimetry (P = 0.1182), or time to FRD resolution (evaluated using Spearman's nonparametric correlation coefficient rho = 0.03, P = 0.8552).
A X2 test with Monte Carlo simulations established a statistically significant association between Group and progression to MH/MHRD (X2 = 8.50, P = 0.007): post-operative incidence of MH/MHRD was significantly higher in the Control group of eyes (9 out of 22 or 41%) compared to that in the Study group (3 out of 35 or 8.6%).
A 49-year-old symptomatic woman complained of metamorphopsia and progressive visual loss in her right eye over 7 months. Her preoperative visual acuity of the right eye was 20/160 (0.90 logMAR), with a refractive defect of -21 + 3.00 × 70, and applanation ocular tension of 10 mmHg. The right eye had an axial length of 29.76 mm with PS, and the fundus photograph showed myopic FRD. Preoperative SD-OCT findings were consistent with ERM proliferation, schisis-like macular thickening, and a remarkable amount of central subretinal macular fluid (SRF) (Figure 1a). Macular surgery was performed using the modified fovea sparing ILM peeling technique. Because of the refractory FRD and increasing foveal symptomatology, the eye underwent a second procedure, employing macular surgical revision by using a BBG dye as an adjuvant to identify any ILM remnants, air-fluid exchange, and a non-expandable 15% perfluoropropane gas mixture. After a 35-month follow-up, the foveomacular region remained attached, with a final BCVA of 20/40 (0.30 logMAR) and an extrafoveal nasal, residual, and very shallow SRF (Figure 1b and Figure 1c) was detected. Furthermore, some recognizable SD-OCT biomarkers, such as an irregular foveal contour and internal and external neuroretina lines without total restoration of the central subfoveal ellipsoid band and the ELM line were observed (Figure 1b, Figure 1c and Figure 1d). The color fundus image showed the presence of myopic changes over the posterior pole with well delineated areas of chorioretinal atrophy peripapillary and extrafoveally located (Figure 1e). The autofluorescence image depicts only very mild RPE foveal changes (Figure 1f). Microperimetry showed reduced mean retinal sensitivity, severely reduced foveal sensitivity with a normal fixation stability, and a location pattern with an abnormally depressed retinal sensitivity analysis map (Figures 1g and Figure 1h). The functional evaluation depicted a reduced mean macular sensitivity of 9.5 dB and 9.2 dB respectively in the 10-2 and 30-2 on macular visual field testing (Figures 1i and Figure 1j). The postoperative functional evaluation with mfERG showed an N1 wave amplitude elevation elicited with a reduction of 72.41%, 58.64%, 42.03%, 36.81%, and 30.92% from the < 2-degree to > 15-degree central rings, respectively, and an abnormally prolonged P1 implicit time (Figure 1k), and rather an abnormal mfERG 3-D elevation map (Figure 1l).
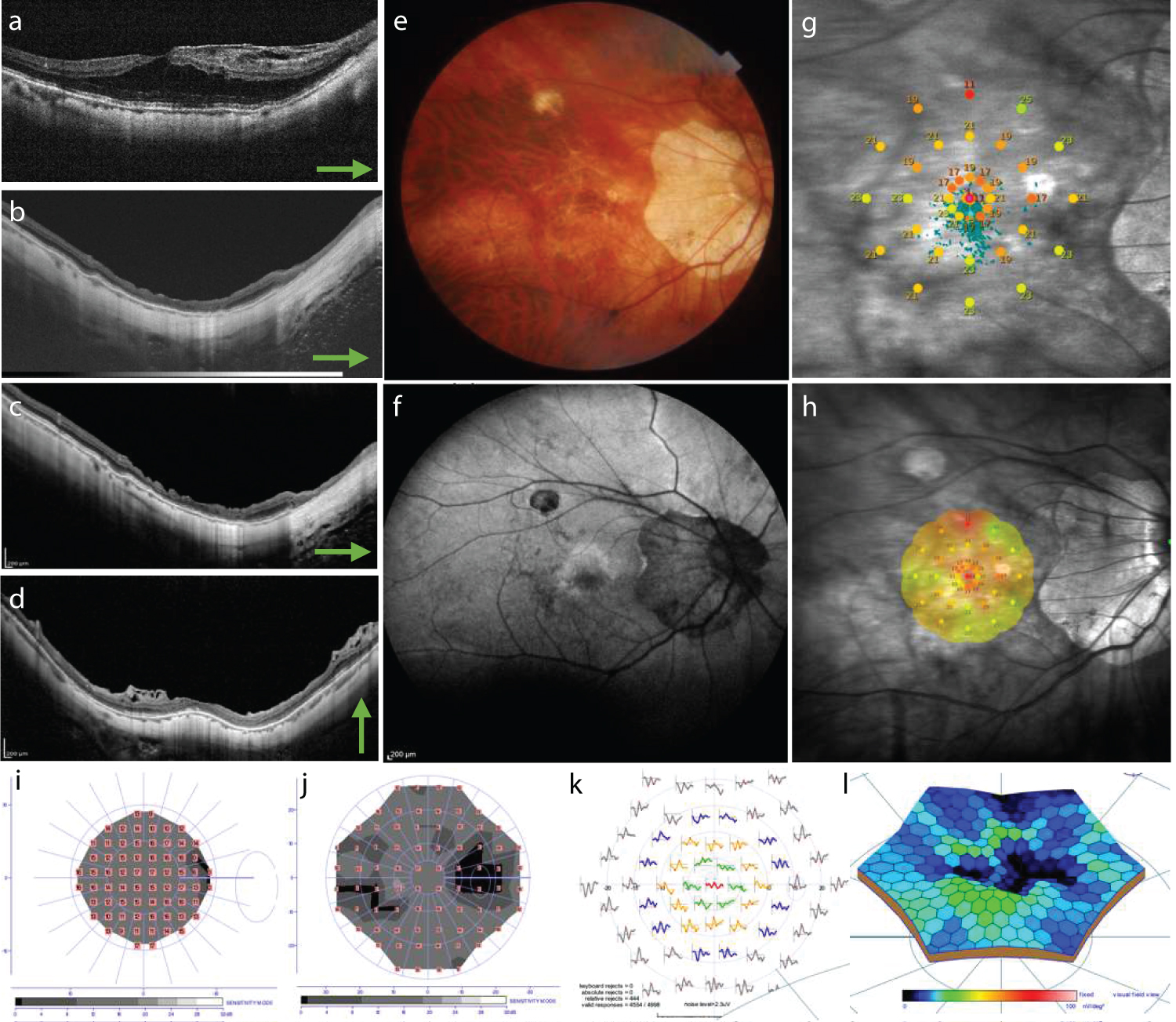 Figure 1: Clinical case 1. (a) Preoperative myopic foveoretinal detachment (FRD) is shown with moderate amount of subretinal fluid (SRF), schisis-like retinal thickening, and evidence of epiretinal membrane proliferation; (b,c) After a 35-month follow-up, the foveomacular region remained attached, with a final best-corrected visual acuity of 20/40 (0.30 logMAR) and an extrafoveal nasal, residual, and very shallow subretinal fluid; (d) Furthermore, some recognizable spectral-domain optical coherence tomography (SD-OCT) biomarkers, such as an irregular foveal contour, and internal and external neuroretina lines without total restoration of the central subfoveal ellipsoid were observed at the internal segment/outer segment line and external limiting membrane; (e) This image depicts a highly myopic eye with an axial length of 29.76 mm, and posterior staphyloma. Some regions of non-foveal chorioretinal atrophy and very irregular but well-defined peripapillary chorioretinal atrophy were observed without clinical evidence of the faint residual macular epiretinal membrane on microstructural spectral-domain optical coherence tomography; (f) Some areas of very faint central and peripapillary autofluorescence indicative of retinal pigment epithelial (RPE) involutional atrophy were observed; (g,h) Microperimetry showed a reduced mean retinal sensitivity, deeply reduced foveal sensitivity with a normal fixation stability, and a location pattern with an abnormally depressed retinal sensitivity analysis map; (i,j) 10-2 and 30-2 central color visual fields depict subnormal retinal sensitivity without any color discrimination elicited; the 10-2 and 30-2 visual field test results revealed mean deficits in the retinal sensitivity of 9.5 dB and 9.2 dB, respectively; (k,l) The multifocal electroretinography (mfERG) recordings were deeply abnormal. The N1 wave amplitude of the mfERG showed a reduction of 72.41%, 58.64%, 42.03%, 36.81%, and 30.92% from the < 2-degree to > 15-degree central rings with a reduced macular and foveal sensitivity, and the PI implicit time was shorter in the < 2-degree central ring and slightly longer in the remaining central rings; An abnormally prolonged P1 implicit time (k) and a rather abnormal mfERG elevation 3-D elevation map was noted (l).
View Figure 1
Figure 1: Clinical case 1. (a) Preoperative myopic foveoretinal detachment (FRD) is shown with moderate amount of subretinal fluid (SRF), schisis-like retinal thickening, and evidence of epiretinal membrane proliferation; (b,c) After a 35-month follow-up, the foveomacular region remained attached, with a final best-corrected visual acuity of 20/40 (0.30 logMAR) and an extrafoveal nasal, residual, and very shallow subretinal fluid; (d) Furthermore, some recognizable spectral-domain optical coherence tomography (SD-OCT) biomarkers, such as an irregular foveal contour, and internal and external neuroretina lines without total restoration of the central subfoveal ellipsoid were observed at the internal segment/outer segment line and external limiting membrane; (e) This image depicts a highly myopic eye with an axial length of 29.76 mm, and posterior staphyloma. Some regions of non-foveal chorioretinal atrophy and very irregular but well-defined peripapillary chorioretinal atrophy were observed without clinical evidence of the faint residual macular epiretinal membrane on microstructural spectral-domain optical coherence tomography; (f) Some areas of very faint central and peripapillary autofluorescence indicative of retinal pigment epithelial (RPE) involutional atrophy were observed; (g,h) Microperimetry showed a reduced mean retinal sensitivity, deeply reduced foveal sensitivity with a normal fixation stability, and a location pattern with an abnormally depressed retinal sensitivity analysis map; (i,j) 10-2 and 30-2 central color visual fields depict subnormal retinal sensitivity without any color discrimination elicited; the 10-2 and 30-2 visual field test results revealed mean deficits in the retinal sensitivity of 9.5 dB and 9.2 dB, respectively; (k,l) The multifocal electroretinography (mfERG) recordings were deeply abnormal. The N1 wave amplitude of the mfERG showed a reduction of 72.41%, 58.64%, 42.03%, 36.81%, and 30.92% from the < 2-degree to > 15-degree central rings with a reduced macular and foveal sensitivity, and the PI implicit time was shorter in the < 2-degree central ring and slightly longer in the remaining central rings; An abnormally prolonged P1 implicit time (k) and a rather abnormal mfERG elevation 3-D elevation map was noted (l).
View Figure 1
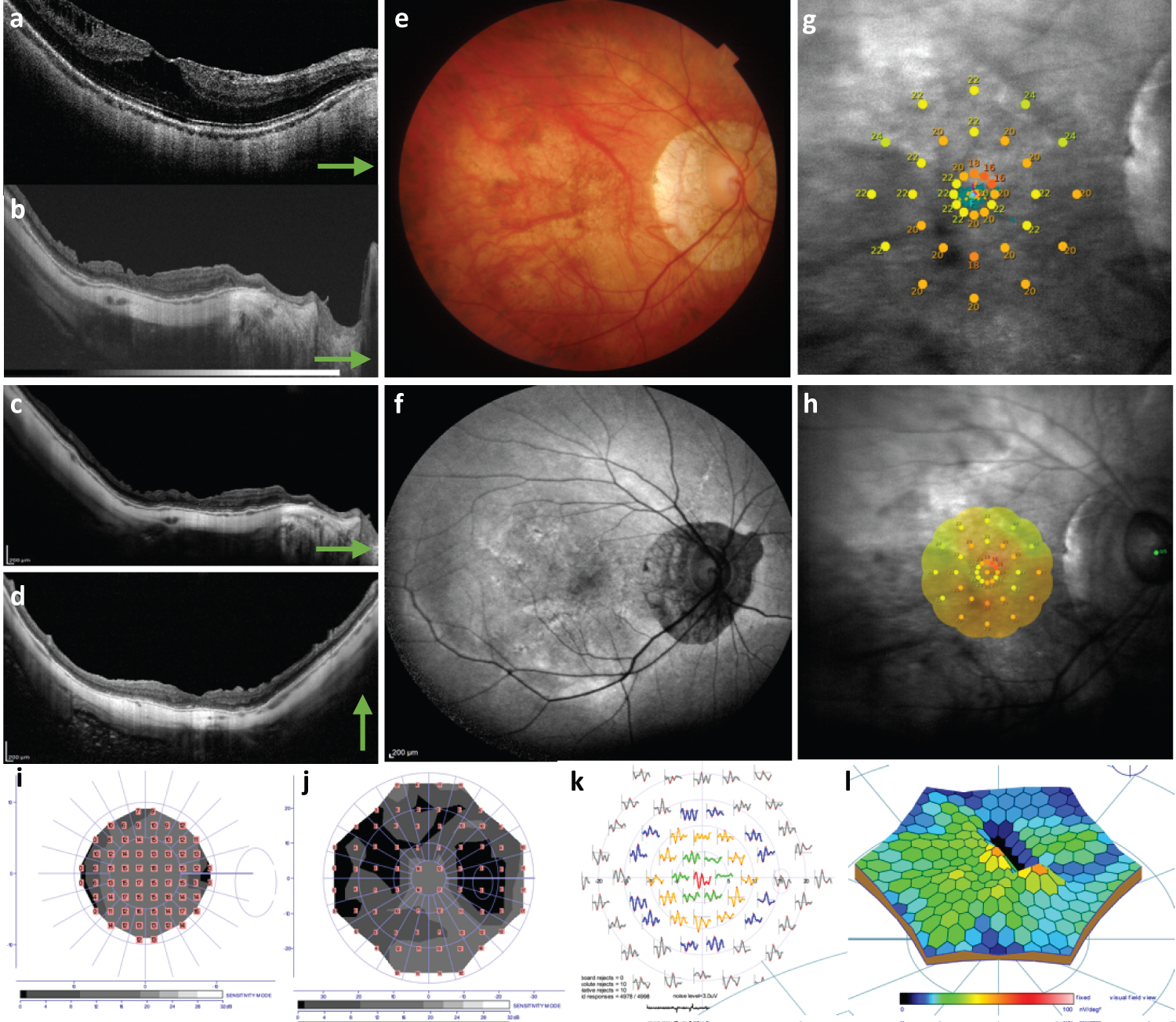 Figure 2: Clinical case 2. (a) Horizontal b-scan through the center of the fovea depicting a preoperative myopic FRD with remarkable amount of SRF, schisis-like-thickening, and superficial traction due to mild ERM proliferation; (b-d) After a 29-month longitudinal follow-up, the operated eye showed a postoperative best-corrected visual acuity of 20/25 (0.10 logMAR), no evidence of recurrent myopic foveomacular retinal detachment or progression to macular hole in the swept-source, and on spectral-domain optical coherence tomography only some superficial dimpling was seen; (e) A highly myopic eye with an axial length of 28.92 mm and posterior staphyloma is depicted; a tesellatus fundus and well-defined peripapillary chorioretinal atrophy were observed with some diffuse RPE thinning and no evidence of any epiretinal membrane (ERM) or foveal elevation was observed in the long-term postoperative analysis on clinical examination; (f) The autofluorescence clinical photo shows only fine and very mild pigment mottling and faint localized central autofluorescence; (g,h) On microperimetry the fixation stability pattern was found to be stable, and the fixation location pattern was documented as foveocentral. The retinal sensitivity analysis map showed abnormal macular integrity with mild reduced sensitivity, mainly at the foveal center, with reduced sensitivity over the thin macula. Fixation stability and fixation location patterns were stable and central; (i,j) Color visual field testing showed mean deficits in the retinal sensitivity of 9.9 dB and 12.4 dB, respectively without any detected chromatic abnormalities; (k) No specific correlation was found between the diffuse reduced macular sensitivity locus and the corresponding macular thickness on the SD-OCT horizontal B-scan in this case. The mfERG showed a reduction of 73.78%, 32.33%, 21.74%, and 28.84% from 2-5 degree to > 15-degree; no reduction in the < 2-degree central ring was observed; (l) Subnormal mfERG 3-D elevation map was seen in this case.
View Figure 2
Figure 2: Clinical case 2. (a) Horizontal b-scan through the center of the fovea depicting a preoperative myopic FRD with remarkable amount of SRF, schisis-like-thickening, and superficial traction due to mild ERM proliferation; (b-d) After a 29-month longitudinal follow-up, the operated eye showed a postoperative best-corrected visual acuity of 20/25 (0.10 logMAR), no evidence of recurrent myopic foveomacular retinal detachment or progression to macular hole in the swept-source, and on spectral-domain optical coherence tomography only some superficial dimpling was seen; (e) A highly myopic eye with an axial length of 28.92 mm and posterior staphyloma is depicted; a tesellatus fundus and well-defined peripapillary chorioretinal atrophy were observed with some diffuse RPE thinning and no evidence of any epiretinal membrane (ERM) or foveal elevation was observed in the long-term postoperative analysis on clinical examination; (f) The autofluorescence clinical photo shows only fine and very mild pigment mottling and faint localized central autofluorescence; (g,h) On microperimetry the fixation stability pattern was found to be stable, and the fixation location pattern was documented as foveocentral. The retinal sensitivity analysis map showed abnormal macular integrity with mild reduced sensitivity, mainly at the foveal center, with reduced sensitivity over the thin macula. Fixation stability and fixation location patterns were stable and central; (i,j) Color visual field testing showed mean deficits in the retinal sensitivity of 9.9 dB and 12.4 dB, respectively without any detected chromatic abnormalities; (k) No specific correlation was found between the diffuse reduced macular sensitivity locus and the corresponding macular thickness on the SD-OCT horizontal B-scan in this case. The mfERG showed a reduction of 73.78%, 32.33%, 21.74%, and 28.84% from 2-5 degree to > 15-degree; no reduction in the < 2-degree central ring was observed; (l) Subnormal mfERG 3-D elevation map was seen in this case.
View Figure 2
A 65-year-old symptomatic woman presented with aggravating metamorphopsia, a progressive drop in central vision, and high myopia. She had PS in both eyes; the right eye had an axial length of 28.92 mm and was subjected to macular surgery because of a 12-month history of symptomatic myopic FRD (Figure 2a). The preoperative BCVA was 20/100 (0.70 logMAR). This eye underwent a three-port 25-G pars plana vitrectomy and non-foveal ILM peeling by the foveal sparing technique. Fluid-air gas exchange was performed with 15% C3F8 tamponade. After a 29-month longitudinal follow-up, the operated eye showed a postoperative BCVA of 20/25 (0.10 logMAR), no evidence of recurrent myopic FRD, and no progression to MH in the swept-source and SD-OCT (Figure 2b, Figure 2c and Figure 2d). Fundus color photo showing a highly myopic eye with well-defined peripapillary chorioretinal atrophy (Figure 2e). Autofluorescence image depicts a well-delineated peripapillary RPE atrophy and very mild pigment mottling changes over the macula consistent with DONFL defects (Figure 2f). Microperimetry showed reduced macular sensitivity, a mild reduction in FRS with stable foveocentral fixation patterns, and an abnormal retinal sensitivity analysis map (Figure 2g and Figure 2h). The 10-2 and 30-2 visual field tests showed a decreased mean macular sensitivity of 9.9 and 12.4, respectively without any elicited alteration on chromatic campimetry (Figure 2i and Figure 2j). N1 wave amplitude of the mfERG showed a reduction of 73.78%, 32.33%, 21.74%, and 28.84% from 2-5 degree to > 15-degree; no reduction in the < 2-degree central ring was observed in this case. The PI implicit time was shorter in the < 2-degree central ring and slightly longer in the remaining central rings. The nV amplitude decreased significantly, with subnormal implicit times for the P1 waves in all central rings in the affected eyes compared to the normal control eye (Figure 2k); a deeply abnormal mfERG three-dimensional elevation map was seen in this case (Figures 2l).
In this study, we evaluated the effectiveness of a modified fovea sparing ILM removal technique in a sample of 35 highly myopic eyes of 31 patients, and presented anatomical results complemented with functional evaluations of the macula and the evaluation of vision. Using postoperative visual acuity and progression to MH/MHRD as outcomes, we found that this modified technique results in a significant improvement of visual acuity and a lower rate of progression to MH/MHRD, compared to the Control group of eyes.
In a large case series [7], Panozzo and Mercanti concluded that surgical resolution of traction during the early stages of FRD would allow re-flattening of the macula center, thus preventing the development of a full-thickness MH and emphasizing the high prevalence of an ERM in highly myopic eyes with MF and FRD. In our study, 32 eyes (91.4%) showed a fully resolved myopic FRD at the end of follow-up. Three eyes (8.5%) showed progression during follow-up, of which 2 (5.7%) developed a full-thickness MH and 1 (2.9%) developed an MHRD. Only one eye showed evidence of very mild extrafoveal ERM reproliferation despite the ILM having been removed in a modified manner. In contrast, only 13 eyes (59%) in the Control group showed a fully resolved myopic FRD at the end of the follow-up.
Shimada, et al. [14] performed a prospective observational study of 8 eyes with MTM, assessed over an average follow-up period of 44 months, and reported that 6 (80%) showed progressive macular thickening with evidence of foveomacular retinoschisis and myopic FRD. Although its natural progression to MH formation has been well described, its multiple pathogenesis has not, particularly as an early stage of MTM. Thus, we speculated that early structural detection of this condition in symptomatic eyes might improve its surgical results, as described by other authors [17].
Most patients with early-stage MTM, such as MF, may be relatively asymptomatic when presenting to retinal and macular specialists. This early stage may persist for many years, with slow and asymptomatic chronic progression before central vision is significantly affected [13]. We agree with Takano, et al. [10] and Shimada, et al. [20] that MF occurs at the earliest stage or is a direct precursor lesion for the development of myopic FRD and is defined as an impending myopic MH traction maculopathy [17].
Uchida, et al. [11] showed that 8 of 10 (80%) eyes at the MF stage progress to myopic FRD, followed by the development of a partial or full-thickness myopic MH during the follow-up. Hayashi, et al. [21] assessed 806 eyes of 429 patients who were followed up for 5 to 32 years and observed the progression of myopic foveomacular retinoschisis (MF) to myopic FRD and to partial-thickness MH in 41% and 20.7% of the eyes, respectively. Focal irregularities and thickness in the external retina have been described as initial findings, followed by formation of an outer lamellar defect associated with a small focal myopic FRD. Since column-like structures exert traction, the lamellar defect elevates the upper edge of the retina, leading to enlargement of the myopic FRD [20,21]. The incidence of myopic FRD in patients with PS is estimated at around 9% [22].
Several surgical techniques have been described for myopic FRD due to MTM. Previous reports have shown that MF can be only treated by vitrectomy, posterior vitreous cortical remnant removal, and gas tamponade with or without ILM peeling [13,23-25]. Most eyes undergoing these techniques are symptomatic with metamorphopsia and show some degree of progressive vision loss. The reported surgical techniques include vitrectomy and long-acting gases with non-ILM removal in primary cases and vitrectomy and classical or modified-ILM removal techniques in refractory cases. Currently, modified techniques such as the fovea-sparing ILM peeling technique with long-term gas tamponade are available for both refractory and primary cases, resulting in foveal reattachment and significant visual improvement [26]. These observations suggest that ILM removal may be beneficial, although presenting some risks inherent to ILM removal, such as superficial retinal damage, thinning of the inner retinal layer, DONFL defects with the appearance of retinal dimples (superficial retinal dimpling), and partial- or full-thickness MH development. To reduce these risks in eyes with myopic FRD, Shimada, et al. used a modified technique called the fovea-sparing ILM removal technique and found that no eyes developed a full-thickness MH, whereas 16.7% of the eyes treated by total classical or non‑sparing ILM removal developed a full-thickness MH [27].
Several authors [13,17,20,23,26] suggested that a myopic FRD is associated with poor prognosis leading to MH formation and, subsequently, to MHRD. Our case series of 35 eyes with symptomatic myopic FRD showed significantly improved postoperative final logMAR vision recovery after being subjected to the fovea-sparing ILM peeling technique along with long-acting gas tamponade. The fact that we did not observe a near 100% visual recovery might be attributable to the outer retinal functional damage due to the chronic presence of macular fluid, as demonstrated by mfERG and microperimetry. In addition, though we did not find associations between postoperative visual improvement and postoperative SD-OCT biomarkers, we speculate that in a larger study with more power, such an association would be found and would provide further support for the success of the surgical technique utilized in our study group.
The development of a full-thickness MH may be spontaneous as part of the natural progression of FRD or secondary to the classical macular surgery for ILM removal, as mentioned by some authors [6,10,25]. Gaucher, et al. [23] stated that the pathogenesis of the myopic MH might be different from that of idiopathic MH. The tangential traction and vitreoretinal traction are the main mechanisms of idiopathic MH [28] while mechanical factors such as scleral stretching, posterior pole elongation with vitreomacular traction exerted via rigid retinal vessels, lack of ILM flexibility, cortical remnants, and persistent vitreomacular traction are the implicated mechanisms in the pathogenesis in highly myopic eyes with PS [5]. Myopic eyes with total posterior vitreous detachment are not protected against the traction exerted by cortical remnants adhering to the macula, and the formation of an MH is always preceded by a myopic FRD in areas where the foveola becomes extremely thin. The tangential traction exerted by a tense ILM, or persistent posterior vitreous remnants might explain the formation of a myopic MH. In a set of independent studies, Shimada, et al. [27], Quiroz, et al. [17], and Shiraki, et al. [29] presented findings for a group of 67 symptomatic highly myopic eyes that underwent macular surgery. No eyes were found to develop a partial or full-thickness MH after macular surgery when using the fovea-sparing ILM removal and gas tamponade, while 57.1% of these eyes showed a normal postoperative SD‑OCT pattern. The authors reported that improved BCVA was observed in eyes treated with gas vitrectomy and the fovea sparing ILM peeling technique. Shiraki, et al. reported that 6 eyes (8%) that underwent the classical ILM removal technique developed MH [29], while Shimada, et al. reported that 5 eyes (16.7%) that underwent the classical ILM removal method developed a full‑thickness myopic MH [30]. Poor preoperative visual acuity and thinner choroidal thickness were identified as risk factors for postoperative MH formation [29].
We speculated that, in the long term, these patients would show profound functional macular sequelae due to the progressive nature of this degenerative disease [2,3], despite the removal of the tractional component. However, removal of the ILM prevents the reproliferation of ERMs and prevents the progression of myopic FRD to MH, thus halting the natural course of MTM; however, this still has possible risks. Potentially severe functional complications such as loss of macular sensitivity, loss of foveal sensitivity with excentric or non-stable foveocentral fixation patterns, non-foveocentral fixation location patterns (preferred retinal loci), and profound alterations in the amplitude of the N1 mfERG waves might develop, irrespective of whether the ILM has been removed in a fovea‑sparing fashion [27].
A previous study reported the importance of macular functional evaluation and abnormal functional findings in extreme macular surgery related to refractory idiopathic MH surgery [31]. Although only 4 eyes underwent extreme surgery using the neuroretinal auto-transplantation technique in that study, and despite the reassuring anatomical outcomes, the authors emphasized the importance of functionally evaluating the macula in eyes that have been subjected to surgery to assess whether a procedure has promising functional outcomes [31].
In our report, photoreceptor dysfunction was considered to be the result of chronic serous separation from the RPE, even though foveal surgical reattachment occurred within the first year. The mfERG showed photoreceptor and outer retinal abnormalities; we compared the mfERG results, point to point, with those of concurrent automated selective chromatic central visual fields. We found that abnormal mfERGs in the same visual field regions that were abnormal on the automatic perimetry provided a high degree of certainty regarding the retinal origin of the defect. Automated fundus-tracking visual-field examination (microperimetry) can overcome the effects of eye movements and retinal fixation changes and obtain precise retina-related sensitivity data. In our study, complete resolution of the myopic FRD detachment was observed in 91.2% of the eyes, with substantial functional recovery but with many functional sequalae at the subclinical level. This was reflected in the psychophysical evaluation, our quantification of the differential retinal threshold of macular sensitivity on microperimetry, and visual field testing under different light (both background and stimuli) conditions that revealed serious macular sensitivity abnormalities in 94.7% of the eyes. Recently, lower macular sensitivity has been reported in highly myopic eyes without detachment, advising the use of this functional technique for longitudinal surveillance of the retina to predict myopic pathology before the loss of vision [32]. Our patients could not be examined with any method of measuring preoperative macular sensitivity, and the long-term postoperative functional evaluation showed macular sensitivity that was lower than that of highly myopic eyes without FRD (39), indicating that macular sensitivity was altered deeply and irreversibly.
Recently, Wai, et al. [33] reported a relationship between visual function and deep retinal perfusion density as measured by microperimetry and OCTA respectively, suggesting that these parameters may serve as early indicators of structural and functional abnormalities in highly myopic eyes with myopic macular degeneration (MMD). Published neurological and functional magnetic resonance imaging studies have previously identified functional alterations across multiple cortical layers in brains of patients with highly myopic eyes [34]. In the future, we plan to investigate the structural and functional postoperative findings in surgically resolved myopic FRD to test whether this macular pathology further leads to the aggravation of cortical surface thickness and related functional connectivity in MMD patients.
Additionally, in our report we found two patients who developed diffuse chorioretinal atrophy (DCRA) and diffuse retinal thinning (DRT) that we consider as a part of the natural history and not due to the surgical intervention. DCRA contributes to a deficient retinal reattachment, DRT, poor visual recovery and also to functional macular sensitivity alterations [35,36]. Fang et al. reported a 10.5% incidence of macular atrophy after vitrectomy, which was higher in eyes with MHRD than in eyes with foveoschisis or foveomacular detachment, but not in eyes that had an MH [37]. Recently, Wai, et al. [33] reported a vasculature-macular sensitivity function relationship between visual function and deep vascular retinal perfusion density as measured by microperimetry and OCTA respectively.
This report has several limitations that warrant consideration. First, the OCT biomarkers utilized in this study are not standardized; to date, only one international consensus panel tried to define the normal anatomical SD-OCT landmarks, highlighting just a few SD-OCT alterations as being well-correlated with the functional results [38]. Nevertheless, our study suggests that an abnormal foveal contour, IS/OS band (subfoveal ellipsoid zone) disruption, ELM line disruption, disruption of the interdigitation zone or segmented RPE line, and en-face SD-OCT retinal analysis abnormalities (e.g., DONFL defects) might be tomographic predictors of vision. In our report, the DONFL appearance defect findings could be considered a consequence of ILM removal; first described by Alkabes, et al. [39] as a subclinical finding. We could not find any electrophysiological or microperimetry evidence of secondary damage due to the ILM removal, and we speculate that the dimples observed represent only mild structural abnormalities in en-face and SD-OCT imaging without visual significance; however, this must be demonstrated in prospective studies. The effects of DONFL on macular function as measured by microperimetry and mfERG is still controversial, and the effect on the tomographic microstructures in this entity, their reaction to the surgical procedures in terms of recovery, and the possible correlation with the postoperative final BCVA are not well understood currently [40]. Second, the study utilized a personalized, modified surgical technique; although intraoperative variables are less predictive than preoperative BCVA with respect to anatomical and visual outcomes [27], we recognize that a prospective standardized and randomized study is required to determine whether the modified technique results in better outcomes. Third, the preoperative BCVA and Amsler tests were the only preoperative functional assessments we used. Because patients presented to the clinic with profound vision loss and loss of central vision caused by the myopic FRD, we considered that preoperative mfERG and microperimetry testing would have identified only isoelectric traces without preoperative clinical relevance or valuable functional contribution; however, these tests were performed during the final postoperative visit as part of the functional postoperative evaluation protocol in eyes that had undergone macular surgery. Fourth, while the aim of the study was to observe long-term changes in macular structure and function, the study was originally designed without a control group. Additional analyses of data from the synthetic control group of eyes utilized in this study provided strong evidence in favor of the modified technique but cannot unequivocally indicate whether observed structural or functional changes were dependent upon the surgical intervention or the time factor alone. Nonetheless, we showed that this uncomplicated surgery solves the macular tractional mechanical problem and consequently stops the natural evolution of this condition to more advanced tractional or combined tractional and rhegmatogenous stages, which are difficult to repair even with several surgical procedures and could lead to irreparable structural and functional sequelae, even severe visual loss from MHRD. The results of this study enable us to speculate that the use of this new and modified surgical technique minimizes the surgical contributions to the development of FRD, allowing it to progress naturally upon the resolution of tractional forces.
The innovative aspects of this study included the modification of the surgical technique of assisted revision via proper staining of the macula for preservation of the foveal flap, coupled with a scheduled and timely structural follow-up of the patients with high myopia. Our findings suggest that symptomatic myopic FRD traction maculopathy should be treated as soon as possible to minimize photoreceptor and RPE damage due to the presence of stagnant SRF and photoreceptor layer separation from the RPE as a source of essential and necessary photoreceptor nutrient and by involutional or secondary atrophy [37]. Myopic FRD should be properly repaired before the emergence of structural damage associated with hard-to-repair full-thickness MH or MHRD. At present, we cannot determine whether the functional alterations observed in this report are due to the prolonged exposure of photoreceptors to SRF or are secondary to mechanisms by which ILM removal causes functional alterations at the subclinical level [41]. Successful early foveomacular anatomical reattachment with fully myopic FRD resolution due to timely removal of premacular tractional tissue can only result in subclinical damage as demonstrated in this study. Recently, Peng, et al. [42] speculated that resolution of myopic FRD after foveal-sparing ILM removal technique is driven by the upregulated local cytokine production. However, highly myopic eyes are at a high risk of developing profound and irreversible loss of vision if they are allowed to progress to partial-, full-thickness MH or MHRD. Therefore, careful prospective and sequential longitudinal tomographic evaluation in the highly myopic population is critical to detect this condition in the early stages and identify the appropriate early surgical strategy by using different macular surgical approaches to optimize visual outcomes. Sequential postoperative structural and functional multimodal evaluation and imaging techniques for the follow-up evaluation of MTM are continuously being developed to offer a more precise clinical diagnosis and prognostic insights to quantify its visual impact. Further prospective randomized clinical trials are needed to better establish the pathogenesis of myopic FRD traction maculopathy and determine the most appropriate surgical procedures to resolve this severe condition.
• Myopic FRD during the early state and as part of MTM is a progressive and potentially blinding condition.
• When myopic FRD is detected on time, it should be treated surgically with care to avoid delay as it is difficult to treat the more advanced MTM stages.
• This condition showed a high incidence of regression and low incidence of MTM progression after using the fovea sparing ILM removal technique. Despite successful anatomical reattachment of the macula, long-term structural and functional evaluations revealed a microstructurally and functionally abnormal macula.
We express our deep appreciation to the technical staff of the Retina Service of the three participating institutions located in Mexico City, Mexico.
None.
The authors declare they have no conflict of interest.
Photos, composite figures, datasets, and laboratory studies supporting the findings of this study may be released upon written application to the Photographic laboratory and Clinical Archives department at Instituto de Oftalmología Fundacíon Conde de Valenciana (Non-profit Organization), Chimalpopoca 14, Colonia Obrera, Mexico City 06800, Mexico and from the Corresponding Author upon request.
Not applicable.
All authors contributed to the study conception and design. Surgeries were performed by Miguel A. Quiroz-Reyes. Material preparation, data collection, and analysis were performed by Miguel A. Quiroz-Reyes, Boris Moreno-Andrade, Erick A Quiroz-Gonzalez, Miguel A. Quiroz-Gonzalez, Hae Jin-Kim, Alejandra Nieto-Jordan, Jorge Morales-Navarro, Margarita Montano, Virgilio Lima-Gomez, and Federico Graue-Wiechers. The first and main draft of the manuscript was written by Miguel A Quiroz-Reyes, and all authors commented on previous versions of the manuscript. All authors have read and approved the final manuscript.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This retrospective study received full ethical approval from the Research Ethics Committees, and was approved by the Institutional Review Committees and the Teaching Departments of the three institutions enrolled (no reference number is provided for retrospective studies by these institutions). Written informed consent in accordance with the institutional guidelines was obtained from all the patients.
Informed consent was obtained from all individual participants included in the study.
The authors affirm that the participants provided informed consent for publication of all images in Figure 1 and Figure 2, as well as images in Online Resources if any.