Anxiety has a great influence on the painful experience related to Temporomandibular Disorder (TMD), but the association between clusters of anxiety phenotypes and the subjective perception of signs and symptoms was few explored in the scientific literature. The aim of this study was to analyze the impact of anxiety level on the pain perception experience and fatigue of masticatory muscles in subjects with chronic TMD according to clusters of anxiety phenotypes.
26 patients with a diagnosis of TMD (DC/TMD) were assessed: Anxiety level (BAI), emotional, sensory and affective aspects of the pain experience (SF-MPQ), pain catastrophizing, presence of referred pain and perception of TMD signs and symptoms (ProTMDMulti). The fatigue (masseter/temporalis) was also analyzed by surface electromyography, and the TMD patients were compared with 13 controls paired by age and gender.
Patients with moderate/severe anxiety showed higher scores for all pain indexes and pain catastrophization, besides a higher association with DC/TMD diagnoses, self-perception of TMD-related signs and symptoms, and higher muscle fatigue mastication (p < 0.05) when compared with minimum/low anxiety. Temporalis muscle showed higher fatigue compared with masseter.
The level of anxiety directly impacts the perception of painful experience and other signs and symptoms of TMD as well as the fatigue response of masticatory muscles. Clusters based on anxiety phenotypes show different clinical manifestations of painful TMD, such results emphasize the need to specific strategies to identify these subgroups in order to increase clinical assertiveness in pain management.
Anxiety, Muscle fatigue, Orofacial pain, Temporomandibular joint disorders
Temporomandibular Disorders (TMD) are defined as a musculoskeletal pain syndrome that affects the masticatory muscles, temporomandibular joint and/or other trigeminal or extratrigeminal areas, in which are associated multisystemic alterations, behavioral changes, emotional status and social interactions, besides an association with the central sensitization phenomena and an imbalance of the descending mechanisms of pain control [1,2].
The pain modulation process is associated with mechanisms of descendent inhibition, through the release of neurotransmitters such as serotonin, dopamine and norepinephrine, which control endogenous analgesia. Emotional factors such as pain catastrophizing and anxiety may influence the expression of this pain control process, increasing nociceptive sensitization and pain perception [3,4].
Patients with TMD and/or other musculoskeletal pain syndromes frequently show inappetence, fatigue, signs and symptoms of anxiety and stress, sleep disturbances, labor difficulties and loss of general quality of life [5,6]. Recent studies have shown that psychological factors such as pain catastrophizing, stress, anxiety, lack of assertiveness in seeking help, and delay in treatment may be associated with maintenance of TMD pain [7,8]. The presence of mental health disorders, such as stress and anxiety, is quite significant in patients with TMD (16-40%), higher when compared with general population (16%) [9-11]. The anxiety assessment is extremely important, especially in patients with TMD signs and symptoms for more than two years, since it indicates the presence of associated emotional comorbidities [11].
Regarding the physical aspects of TMD, the complaint of tiredness in the masticatory muscles is frequent, being associated with the fatigue and pain. Muscle fatigue can be understood as the lack of ability to sustain a muscle contraction for a period or by the decrease in contraction force during prolonged muscle activity. Muscle fatigue tests can provide an indication of the performance of masticatory muscles, and patients with chronic painful TMD tend to have more fatigue than control subjects, which contributes to the maintenance of pain and anxious states related with pain [3,5,12,13].
Considering this clinical association between painful TMD and anxiety states, the central hypothesis of this study is that patients with higher anxiety levels perceive pain and manifest TMD signs and symptoms in a more exacerbated way than patients with low anxiety levels. Therefore, the aim of this study was to analyze the impact of anxiety level on the pain perception experience and fatigue of masticatory muscles in subjects with chronic TMD according to clusters of anxiety phenotypes.
A total of 26 patients composed the sample, 15 women and 11 men, ranging in age from 21 to 54 years (mean = 36 ± 4.2) from a specialized service in TMD and Orofacial Pain, with diagnosis of TMD according to criteria of the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) and with complete dentition [14]. Subjects with a history of craniofacial traumas or tumors, with dental absences, neurological and/or psychiatric disorders, patients taking anxiolytic medications, anticonvulsants and/or antidepressants were excluded from the study. 13 control subjects (50% of the total TMD sample) paired by age and gender were compared with the TMD sample only regarding the data of electromyographic activity, which were available in the database of the equipment analysis software.
Were included patients with painful TMD (muscle and/or joint), with presence of pain in the orofacial region for more than three months and with stable functional dental occlusion. Were excluded subjects with dental absences, use of removable prostheses, use of fixed prostheses with more than two elements, patients who were been treated with occlusal splints, presence of occlusal discrepancies (crossbite, open bite, accentuated horizontal and vertical overjet), patients with neurological or psychiatric disorders, patients with presence or history of autoimmune diseases, patients who make use of pain medication (antidepressants, anxiolytics, anticonvulsants), patients undergoing orthodontic, speech therapist or dental treatment for TMD, or who have received any of these in the last 6 months.
This study was approved by the Research Ethics Committee of the School of Dentistry of Ribeirão Preto-University of São Paulo (53561316.0.0000.5419). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. The control subjects also signed the consent form for participation in the research.
In addition to the clinical evaluation for the TMD diagnosis, other questionnaires were applied to the sample for a more comprehensive delineation of the participant's pain experience. They responded to the ProTMDMulti questionnaire (Protocol for Multi-professional Centers for the Determination of Signs and Symptoms of Temporomandibular Disorders), which assess the self-perception regarding ten signs and symptoms commonly related to TMD in 4 daily situations: chewing, waking, talking and resting), and for each question the participant should assign a score from zero to ten, in which zero means absence and ten the worst possible severity of the signs or symptom, thus enabling a maximum score of 400, the higher score is associated with a worse perceived severity [15].
It was also applied the SF-MPQ (Short-Form McGill Pain Questionnaire) in its translated and adapted version to Brazilian Portuguese [16]. This questionnaire refers to perceived pain at the time of its application. It consists of five indexes: Sensory Pain Rating Index (S-PRI), Affective Pain Rating Index (A-PRI), Total Pain Rating Index (T-PRI), Global Pain Experience Rating (measured with a Visual Analogue Scale-VAS) and Present Pain Intensity (PPI). The S-PRI consists of 11 descriptors of the sensory pain experience and the A-PRI by 4 affective descriptors, and for each descriptor it is possible to measure on a likert scale of 0-3 the intensity of the pain at the assessment moment, being 0 (without pain), 1 (mild), 2 (moderate) and 3 (severe). The Global Pain Experience Rating (VAS) is related with the pain intensity, as described above. And in the PPI are six words that describe a painful experience: No pain, mild, discomforting, distressing, horrible and excruciating; The volunteers were instructed to choose the word that best describes their experience of pain.
Other aspects related to pain experience have also been investigated: Pain catastrophizing (Pain-Related Catastrophizing Thoughts Scale) and presence of referred pain on masticatory muscles during the palpation test, based on the DC/TMD protocol. It is important to emphasize that the control subjects did not respond to the other questionnaires and protocols used in this study, since they are directed to the presence of pain, as these individuals did not have pain, the application was unfeasible.
The Beck's Anxiety Inventory (BAI) was used to determine the level of anxiety, with the objective of identifying signs and symptoms perceived weekly associated with anxiety. This questionnaire consists of 21 multiple-choice questions, each of which has four possible answers, which are: No (zero score), low (score 1), moderate (score 2), and severe (score 4). BAI analysis is performed by summing the score of each response, characterizing anxiety states. The possible score ranges are: From zero to seven points there is indication of minimum level of anxiety, from eight to 15 points mild anxiety, from 16 to 25 points moderate anxiety and from 26 to 63 points severe anxiety.
In order to complement the analysis of TMD clinical manifestations associated with anxiety levels, subjects underwent the surface Electromyography (EMG) examination during seated tests (to assess baseline EMG activity) and in maximal voluntary contraction, sustained for 10 seconds, in the position of maximum habitual intercuspation, to analyze the fatigue state of the masticatory muscles. The frequency variation (%) of the EMG activity, provided by the equipment program itself, named Long Clench, was analyzed. For this test, the electromyograph Myotrace 400, with capacity for 8 channels (Noraxon®, Scottsdale, Arizona, USA) was used. Silver chloride disposable surface bipolar electrodes (Hall Industria e Comércio LTDA, São Paulo, São Paulo, Brazil) were fixed to the skin on anterior masseter and temporalis muscles positioned parallel to the bundles of muscle fibers and a reference electrode was fixed at approximately 10 mm above the glabella.
After collecting the data, 4 subgroups (clusters) were set according to the anxiety levels obtained from the BAI questionnaire: Minimum anxiety (scores from zero to 7), low (8 to 15), moderate (16 to 25) and severe (26 to 63). From this, the groups were analyzed comparatively to the scores obtained in the other evaluations using ANOVA One Way (Bonferroni Posttest) for the following variables: Emotional, sensory and affective aspects of the pain experience, pain catastrophizing and referred pain on masticatory muscles. The significance level adopted was 5% (p < 0.05) (Bioestat 5.0, Instituto Mamirauá, Brazil).
The group with severe anxiety showed higher scores for all SF-MPQ pain indexes when compared with other groups (p < 0.05). In addition, pain catastrophizing was also different among anxiety groups, i.e. patients with moderate and severe anxiety had a higher pain catastrophizing rate, with statistical significance (p < 0.05) (Table 1).
Table 1: Sample and gender for each anxiety level subgroup, mean and standard deviation of the SF-MPQ indexes, pain catastrophization, total Pro TMDMulti score, percentages of diagnoses according to the DC/TMD and presence of pain with referral. Anova One Way (post-Bonferroni test, p < 0.05). View Table 1
Regarding the painful TMD, the group with severe anxiety had a higher perception of signs and symptoms (180) according to the total ProTMDMulti score, followed by the group with moderate anxiety (83), low (29) and minimal (22), following a pattern decreasing. Regarding the diagnosis of TMD (DC/TMD), the groups with severe and moderate anxiety showed more conditions of association (painful and articular) in comparison to the other groups, which presented higher percentage of painful conditions alone. In addition, patients with higher levels of anxiety also showed more painful sites with referred pain (Table 1).
The results of surface electromyography demonstrated higher fatigue of the masseter and anterior temporalis muscles in patients with painful TMD in comparison to controls, and in the groups with higher levels of anxiety (severe and moderate), muscle fatigue was higher than in the other groups (Figure 1). In the comparison of the two muscles, the anterior temporalis showed higher fatigue when compared to the masseter, independent of the right or left side (p < 0.05).
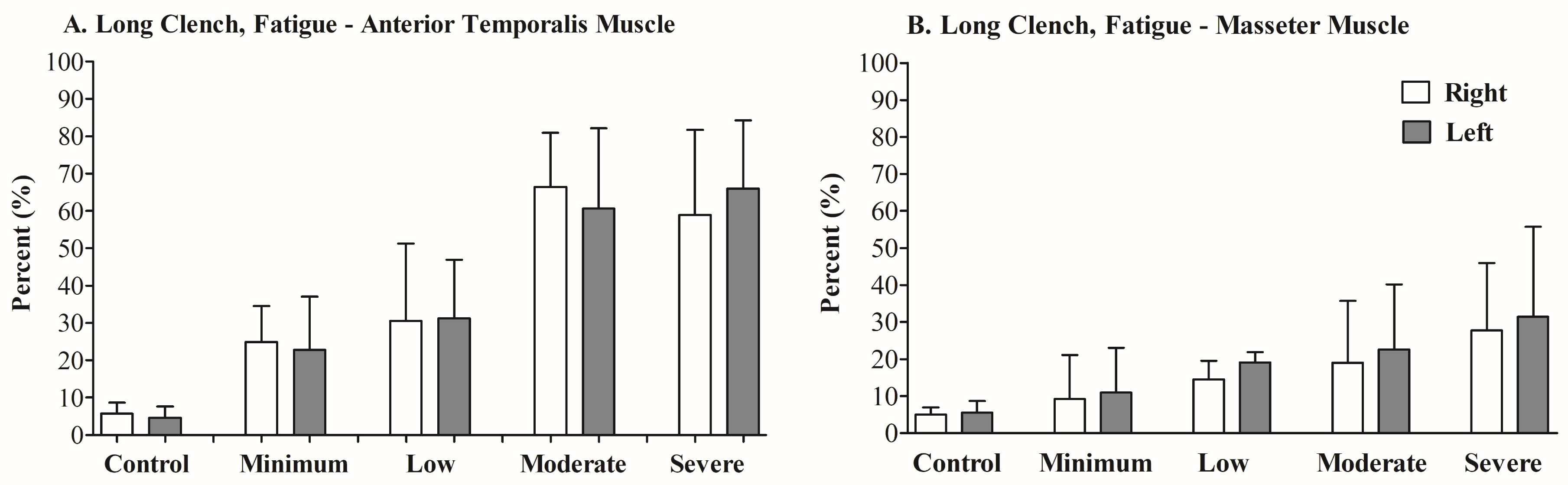 Figure 1: Long clench, fatigue of the anterior temporalis and masseter muscles (right and left sides) for the analyzed groups (control and anxiety levels-minimal, low, moderate and severe). Percentage of frequency variation (Hz) indicative of fatigue (%).
View Figure 1
Figure 1: Long clench, fatigue of the anterior temporalis and masseter muscles (right and left sides) for the analyzed groups (control and anxiety levels-minimal, low, moderate and severe). Percentage of frequency variation (Hz) indicative of fatigue (%).
View Figure 1
The results showed that the patients with higher anxiety perceive the pain with increased intensity, since they present higher scores in all SF-MPQ indices in comparison with less anxious patients. The presence of painful TMD leads to greater predisposition to anxiety [3,5] and more anxious individuals are more likely to perceive pain in TMD clinical situations [3]. Pain is understood as an experience strongly influenced by emotional factors, it is relevant to assume that nociception may often not be compatible with the perception of pain in these anxious patients, that is, the experience of pain and consequently their report can be amplified in function of the anxiety level, corroborating with the results of this study [1,2]. This does not mean that these patients presented more severe TMD clinical symptoms, but the pain felt, and the coping of this pain are different in these more anxious subjects.
A recent study found that among TMD patients, women had higher levels of stress and anxiety. In the present study, it was found similar results, TMD women are more anxious e show higher pain scores when compared with men. Women with poor social support or diagnosis of myofascial pain also demonstrate more significant levels of anxiety. The presence of anxiety should be considered as an additional factor in musculoskeletal pain, especially in the treatment plan for patients diagnosed with TMD [3].
Other components such as depression, somatization and the presence of painful comorbidities are also important in the clinical manifestation of TMD, since they directly affect the perception of symptoms, especially pain [17]. The identification of responders and non-responders clusters to TMD therapies based on emotional aspects may be of great utility in the clinic in order to achieve more satisfactory results and clinical assertiveness, for example, in a recent study which demonstrated that low-level laser therapy is not effective for TMD pain relief in patients with severe anxiety level and is more appropriate for patients with reduced or moderate anxiety [18].
Likewise, the more anxious patients showed higher pain catastrophization, evidencing a significant difference with the other groups that showed lower levels of anxiety. Other studies have also shown that subjects with TMD present greater pain catastrophization, somatization and other psychological impairments when compared to healthy subjects [19,20]. However, within the group of patients seeking treatment for TMD signs and symptoms, there are subgroups that vary depending on the presence of comorbidities, level of perception and chronic pain, positive or negative emotional aspects, previous experiences, among many other variables that can contribute to the treatment response.
The perception of TMD signs and symptoms was also higher in patients with higher levels of anxiety, in addition to the presence of more trigger-points with referred pain. These aspects may be related to a higher hypervigilance of the orofacial region, which generates a greater demand of complaints of these patients. This is also related to the personality of patients with chronic pain, who tend to be more pessimistic and with fearful behavior, skepticism, hypervigilance, valuation of poor life experiences and low motivation [21].
Despite these evidences, the psychological profile is not directly related to the localization of pain in patients with painful TMD, i.e. pain in the muscular regions or in the region of the temporomandibular joint, however more anxious patients tend to present more isolated or combined muscular pain with joint pain than just articular pain [22], agreeing with the results of this study that also verified the higher occurrence of muscle pain in patients with mild anxiety and muscle/joint pain in those with moderate and severe anxiety.
The presence of elevated levels of anxiety has been shown to be a long-term predictive variable for the development of chronic pain [23,24]. Pain-related anxiety, that is, that arising from the persistence of pain sensation, contributes very negatively to management strategies, as it causes patients to seek immediate alternatives that do not aim at behavior change and/or cognitive awareness about pain experience, such as analgesic drugs, which alleviate short-term pain but do not have great effectiveness for chronic pain and do not lead to resolution [24]. In this perspective, the management of the anxiety level is of paramount importance for patients with chronic pain, since they interfere both in the subjective perception of pain and in the response to the treatment strategies.
This study demonstrated that more anxious patient's shows higher fatigue of the masseter and anterior temporalis muscles in the electromyographic evaluation. Other studies have shown that, in general, patients with painful TMD tend to have higher fatigue rates compared to control [12,25]. Wózniak, et al. have shown that increased masseter and temporalis fatigue is correlated with the intensity of TMD signs and symptoms, and patients with more chronic and complex clinical conditions tend to show higher fatigue of these muscles, which may contribute to the first onset and pain maintenance [13]. Among the group of patients with painful TMD, women showed more fatigue of the masticatory muscles. These results may be related to the presence of parafunctional habits, or perhaps to the higher perception of pain that generates a lower maintenance capacity of the sustained contraction, or to the functional adaptations of the stomatognathic system structures because the presence of TMD, which generate higher fatigue of these muscles.
Therefore, anxiety can be understood as a factor that subdivides the groups of patients with TMD in relation to their clinical manifestation in the following aspects: Intensity and Quality of Pain (SF-MPQ), pain catastrophizing, subjective perception of signs and symptoms, the complexity of the TMD diagnosis, the presence of referred pain and the fatigue of the masticatory muscles. In this sense, this triad composed by anxiety, pain and muscular fatigue seems to be directly proportional to the manifestation of TMD. Such reflections contribute to a better understanding of the phenotype of chronic TMD patients and to the development of more assertive treatment strategies that take into account specific characteristics of each subgroup with an enlarged view.
More anxious patients perceive pain from temporomandibular disorders in a more exacerbated way: With higher intensity, higher pain catastrophizing, more referred pain and with higher perception of other TMD signs and symptoms. In addition, more anxious patients show more fatigue of the masseter and anterior temporalis muscles, which may be a result of increased muscle tension, the presence of parafunctional habits that may be related to anxiety and/or lower capacity to maintain a contraction sustained by the presence of pain. Therefore, the level of anxiety directly impacts the perception of painful experience and other signs and symptoms of TMD as well as the fatigue response of masticatory muscles. Clusters based on anxiety phenotypes show different clinical manifestations of painful TMD, such results emphasize the need to specific strategies to identify these subgroups in order to increase clinical assertiveness in pain management.
The authors declare no conflict of interests.