Tooth loss is a risk factor for dementia. This study aimed to compare the occlusal imbalances in cognitively impaired elderly patients to those with normal cognitive function.
Twenty-five cognitively impaired patients and 17 control subjects with normal cognition (aged ≥ 65 years; 78.12 ± 7.56) were included in this study. These two groups were categorized into two subgroups by their use of removable partial dentures. The Mini-Mental State Examination was used to evaluate cognitive function, medical and dental examinations were conducted, and digital analysis of occlusion was performed.
All control subjects had ≥ 24 teeth and 22 cognitively impaired subjects had ≤ 20 teeth. The correlation between the number of teeth and cognitive function revealed significant differences between the two groups (P < 0.05). The occlusal imbalances exhibited significant differences in correlation with cognitive function (P < 0.05).
A correlation was observed between tooth loss and occlusal imbalances with cognitive function.
T-Scan, Dementia, Cognitive ability, Occlusal parameters, Elderly, Tooth loss, Cognition
DQoL: Dementia Quality of Life Instrument; MMSE: Mini-Mental State Examination; RPD: Removable Partial Denture
Dementia, as defined by the World Health Organization, is a syndrome that affects memory, thinking, behavior, and the ability to perform daily activities. Approximately 47.5 million people are affected by dementia worldwide, and this number is projected to double or triple by 2050 [1]. The two most common types of dementia are Alzheimer's disease and vascular dementia, with the former being the leading cause of dementia in the elderly population [2]. Risk factors for dementia include ageing, illiteracy, lower education level, lower socioeconomic status, head trauma, genetic factors, cardiovascular risk factors, obesity, smoking, hypertension, diabetes mellitus, inactive lifestyles, and loss of teeth [3-6]. Furthermore, decreases in cognitive function are caused by changes in the regions of the brain involved in learning, memory, and emotional behavior [7], all of which are known to be related to masticatory function [5,6,8]. Animal studies have demonstrated that loss of natural dentition has a negative effect on learning and memory [9,10], suggesting that maintaining good oral health may be one of the key methods to preventing dementia and other cognitive disorders. Food intake and digestion are the primary roles of mastication [11], and studies have indicated that proper mastication promotes and preserves cognitive function [12,13], possibly due to the constant input of sensory signals to the central nervous system by the masticatory muscles. Proper mastication is influenced by a multitude of factors including the person's ability to chew. This ability of an individual to chew food is affected by the structures responsible for this action such as the teeth, muscles, occlusal force, etc. The influx of sensory signals during mastication stimulates the cognitive and memory centers of the brain [14,15]. It was reported that mastication increases cortical blood flow and activates various somatosensory, supplementary motor, and insular cortical areas, as well as the striatum, thalamus, and cerebellum. In addition, it was found that decreased chewing function in mice led to degeneration of the neurons in their hippocampi, which in turn led to impaired memory function [16,17]. Measuring an individual's masticatory ability can be somewhat difficult. Different tools for analysis of occlusal parameters are available, such as articulating papers, Shimstock foils, impression waxes, silicone impressions, etc. However, the outputs of said tools are hard to quantify. Therefore, the T-Scan Digital Occlusal Analysis System was used in this study, which can measure the relative occlusal force distribution, timing of occlusion, and occlusal force intensity. Moreover, in comparison to T-Scan, the other tools are highly susceptible to inaccuracies, and they have low repeatability which can result in distortion and false positive readings. T-Scan, on the other hand, provides a dynamic occlusal measurement that reveals the levels and timing of force on individual teeth, thereby indicating the occlusal stability of the overall bite [18]. The purpose of the present study was to compare and correlate the occlusal imbalances in elderly patients with cognitive impairment to those with normal cognitive function.
This study was conducted in accordance with the regulations of and with the approval of the Institutional Review Board at Gachon University, Incheon, South Korea (IRB no. 1044396-20510-HR-050-20). Informed consent was obtained from each subject or from relatives or legal representatives. The study was conducted from May 2017 to August 2017 (November 2015 and July 2016) at the Department of Exercise, Rehabilitation and Welfare of Gachon University Medical Campus, Incheon, South Korea.
Forty-two patients (aged > 65 years; 78.12 ± 7.56; 27 females and 15 males) were enrolled in this study. All patients were asked to take the Korean version of the Folstein test or the Mini-Mental State Examination (MMSE) as seen in Figure 1 [19], which is a tool used to assess an individual's level of cognitive function. This 30-point questionnaire is used in both clinical and research settings. It is also used to estimate the severity and progression of cognitive impairment in order to follow the course of cognitive changes in an individual over time. It is comprised of tests for orientation, registration, short term memory, language use, comprehension, and basic motor skills. Scores range from 0-30. Patients who score 20-25 points are said to have mild cognitive impairment; Patients scoring 10-19 points are considered to be in the moderate stage, while patients scoring ≤ 9 points are considered to be in the severe stage [20]. After assessing the subjects' level of cognitive ability, they were divided into two groups: Those with MMSE scores of ≥ 25 were classified as normal and were assigned to the control group (n = 17), and those who scored < 25 were classified as having mild cognitive impairment and were assigned to the experimental group (n = 25). No patients scored < 20; Therefore, all subjects included in the experimental group were classified as having mild cognitive impairment. Any subject with disorders that could interfere with the psychometric assessments (severe blindness, terminal illness etc.) and patients who were completely edentulous were excluded from the study. The subjects from both groups were then subcategorized into those who wore Removable Partial Dentures (RPD) and those who did not. Between the control and experimental groups, four subgroups were formed: Two in the experimental group and two in the control group.
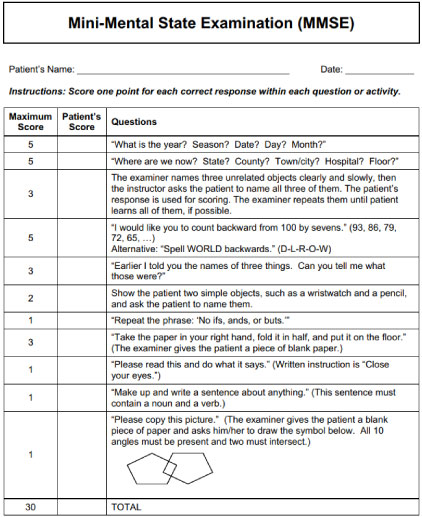 Figure 1: Mini-mental state examination. View Figure 1
Figure 1: Mini-mental state examination. View Figure 1
After the subjects were divided into the experimental and control groups, medical examinations were conducted to determine if they had systemic diseases that could have rendered the results inconclusive. Two dentists also conducted dental examinations to assess the use of RPDs, the number of remaining natural teeth, and the condition of the remaining teeth. The dentists also assessed the location of the RPDs and used Kennedy's classification to differentiate the patients.
The T-Scan III (Version 7, Tekscan Inc. S. Boston, MA, USA) was then used to assess the occlusal parameters of the patients. The T-scan sensor was inserted intraorally by resting the sensor support within the facial central incisor embrasure of the maxillary teeth. The patient was then asked to firmly bite down into the sensor and to firmly hold their teeth together for 1-3 s until maximum intercuspation is reached. The subject was then asked to repeat the procedure for improved accuracy. The recording indicated the force details of the occlusal contact time sequence from first contact to maximum intercuspation, and simultaneously indicated the history of the right to left arch force imbalance of the contact closure sequence (Figure 2). The results of the analysis were gathered and recorded for each of the patients.
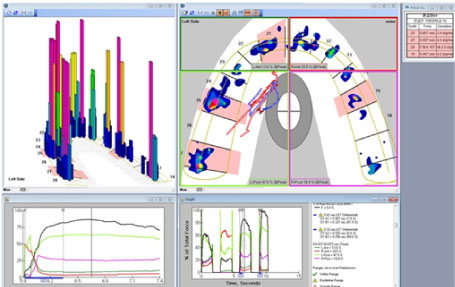 Figure 2: Sample output of the results from the digital occlusal analysis. View Figure 2
Figure 2: Sample output of the results from the digital occlusal analysis. View Figure 2
The presence of depression and quality of life of the subjects were also assessed by the psychologists at Gachon University using the Dementia Quality of Life Instrument (DQoL).
The Mann-Whitney U-test was used to correlate the patients' cognitive ability with the number of remaining natural teeth, left and right occlusal asymmetry, anteroposterior occlusal asymmetry, depression, and quality of life with the use of IBMM SPSS Statistics for Windows version 22 (Armonk, NY). The level of significance was assumed to be P < 0.05 for all tests.
The epidemiological and clinical characteristics of the subjects in the control and experimental groups are summarized in Table 1. The mean age of the subjects in the cognitively normal (control) and cognitively impaired (experimental) groups was 78.3 ± 3.25 and 81.6 ± 2.98, respectively. There was no significant difference in age between the groups. The other clinical characteristics did not exhibit significant correlations with cognitive function.
Table 1: Epidemiological and clinical characteristics of the two main groups. View Table 1
Table 2 summarizes the variables measured in this study for all subjects. Firstly, in the subjects who were not RPD wearers, the average number of remaining natural teeth (dental status) were 24.92 ± 3.70 in the control group and 14.83 ± 4.48 in the experimental group, which rendered a statistically significant difference (P = 0.01). The mean left and right occlusal asymmetry was 14% in the control group and 39.66% in the experimental group, and the difference was statistically significant (P = 0.03). The mean anteroposterior occlusal asymmetry was 73.99% in the control group and 58.60% in the experimental group. However, the difference was not significant (P = 0.143). The mean MMSE score was 3.17 ± 2.89 in the control group and 1.83 ± 2.66 in the experimental group, but the difference was not significant (P = 0.143). Lastly, the mean DQoL scores for the control and experimental groups were 9.42 ± 9.13 and 3.5 ± 4.19, respectively. Again, the difference was not significant (P = 0.089). In the subjects who were RPD wearers, the average number of remaining natural teeth (dental status) were 22.40 ± 2.07 in the control group, and 8.9 ± 3.43 in the experimental group, and the difference was statistically significant (P = 0.02). The mean left and right occlusal asymmetry were 28.52% in the control group and 22.38% in the experimental group, but the difference was not significant (P = 0.443). The mean anteroposterior occlusal asymmetry was 10.02% in the control group and 57.79% in the experimental group, and the difference was significant (P = 0.019). The mean MMSE score was 1.40 ± 2.07 in the control group and 1.77 ± 2.09 in the experimental group; However, the difference was not significant (P = 0.84). Lastly, the mean DQoL scores for the control and experimental groups were 8.40 ± 12.36 and 6.08 ± 7.83, respectively, but the difference was not significant (P = 0.80). These results are presented in Figure 3 and Figure 4.
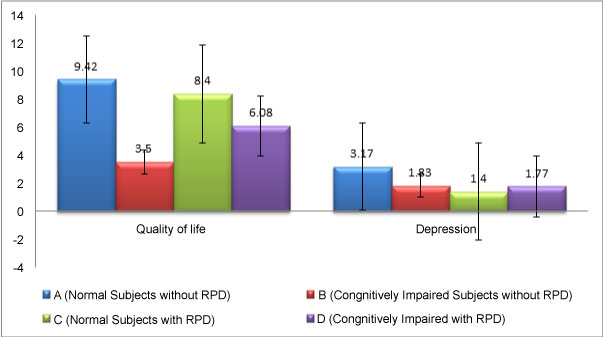 Figure 3: Cognitive ability, number of teeth, and occlusal asymmetries. View Figure 3
Figure 3: Cognitive ability, number of teeth, and occlusal asymmetries. View Figure 3
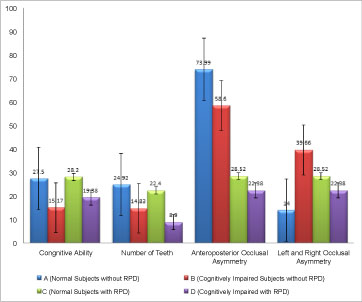 Figure 4: Quality of life and depression. View Figure 4
Figure 4: Quality of life and depression. View Figure 4
Table 2: Occlusal parameters of each group. View Table 2
Dysfunction in the masticatory system affects cognitive function, particularly among the elderly [21] and one of the risk factors for cognitive impairment, specifically Alzheimer's disease, is loss of natural dentition [5]. Loss of teeth due to oral pathology, trauma, and heredity contributes to occlusal imbalance in the stomatognathic system, which further leads to masticatory dysfunction [22]. Additionally, occlusal imbalance also reduces the individual's ability to masticate. Specifically, the loss of teeth and occlusal imbalance creates changes in the physiology of the hippocampus that can be pathological and lead to deficits in learning and memory [23]. In our study, we determined the correlation between the number of remaining natural teeth and cognitive function, both in denture-wearing and non-denture-wearing groups. This division is due to the fact that comparison between individuals using dentures and those who are not, may render the results inconclusive. Our results indicated that there was a close correlation between loss of natural teeth and cognitive function in elderly subjects within the chosen community. A total of 24 subjects had < 20 teeth and 80% of those subjects exhibited cognitive impairment. This finding is in agreement with the aforementioned study [23], stating that a lower number of teeth, particularly in the ones approaching edentulism, was significantly correlated with impaired cognitive function. The previous report also stated that the decline in the number of teeth contributed to the decline in the masticatory function of individuals, which further decreased the cognitive abilities of the individuals by inducing pathologic changes in the learning and memory centers of the brain. However, in our study, we observed no significant differences in the cognitive abilities of patients wearing dentures compared to those who were not wearing dentures. Similar results were observed in a study conducted by Lexomboon, et al. [5]; The report concluded that whether elderly people chew with natural teeth or dentures may not contribute significantly to cognitive impairment, provided no chewing difficulties are present. In the current study, it was also found that imbalances in the distribution of occlusal forces were significantly related to the cognitive ability of the subjects. Differences in the occlusal force distribution in the anteroposterior dimensions are due to the involvement of the posterior teeth in the grinding of food. Occlusal force is affected by factors such as gender, age, contact area, and increased contact between teeth [20,24]. Therefore, the posterior teeth naturally exhibit greater force distribution than the anterior teeth. However, discrepancies in occlusal force distribution in the sagittal dimension on the left and right sides might contribute; Some patients may be right-side chewers or left-side chewers. Chewing preferences may bring about asymmetries in force distribution in the sagittal dimension, and may be influenced by functional dominance, temporomandibular disorders, muscle activity, use of dentures, etc. [25,26]. Left-side chewing activates the supplementary motor area of the brain, while right-side chewing activates the inferior frontal gyrus and inferior parietal lobule [27]. Theoretically, this suggests that a decrease in the activation of the frontal gyrus and inferior parietal lobe areas could lead to memory loss. A study by Lee, et al. [26] reported that mastication ability does not differ between dominant and non-dominant sides, and it was suggested that brain dominance correlates with chewing preference but does not affect the efficiency of mastication. The present results indicated that, regardless of the use of dentures, subjects with fewer remaining teeth obtained a lower score on the MMSE, rendering them cognitively impaired. Previous studies reported that systemic diseases, such as diabetes and renal disorders, significantly correlate with an individual's cognitive ability [28]. However, in our study, we did not find significant correlations between systemic diseases and cognition. Previous studies [29,30] have also reported that loss of teeth is more prevalent in women than in men. We have observed similar results in our study wherein 70% of the 24 subjects with < 20 teeth remaining were women. We also observed that there were more women than men who were cognitively impaired; A total of 17 out of 25 (68%) of our cognitively impaired subjects were women. However, this difference was not significant.
The results of our study indicate a clear correlation between tooth loss, occlusal force distribution asymmetries, and cognitive function. The clinical relevance of our results is evident. Oral health awareness is very important for the general population. The ability to maintain good oral health can lead to improved mental and physical health. Attention and priority should be given to an individual's oral health in order to maintain or even improve mastication, which could lead to stabilization or even improvement of cognition.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.