Soft tissue sarcomas of the breast are very rare tumors and account for less than 1% of all primary malignant breast tumors. We are reporting a case of primary myxofibrosarcoma of the breast in a 55-year-old woman treated at King Abdulla Medical City and we conducted a literature review on primary soft tissue sarcomas of the breast.
Primary soft tissue sarcomas of the breast are extremely rare neoplasms [1]. One of the largest published retrospective reviews of a single cancer center experience reported 78 primary and non-metastatic breast sarcomas. The pathologic sub-classifications of these cases were malignant cystosarcoma phyllodes in 32 patients, with the remainder being stromal sarcoma, angiosarcoma, fibrosarcoma, carcinosarcoma and liposarcoma [2]. In another large clinicopathologic series from Mayo Clinic 25 cases of primary sarcoma of the breast were reported, histopathological diagnoses were fibrosarcoma (6), angiosarcoma (6), pleomorphic sarcoma (6), leiomyosarcoma (2), myxofibrosarcoma (3), hemangiopericytoma (1) and osteosarcoma (1) [3]. More recent series reported 19 cases of primary breast malignant fibrous histiocytoma (MFH) or myxofibrosarcoma; storiform-pleomorphic subtype was most common (10), myxofibrosarcoma (6) and giant cell subtype (1) [4]. Several other case reports have been published on pathological diagnostic dilemma of a primary myxoid breast sarcoma [5-7]. Most of these tumors have an epithelial component and therefore are classified as phyllodes tumors. Although, these tumors constitute a specific clinicopathologic entity and therefore should be differentiated from the two other main entities in differential diagnosis, which are cystosarcoma phyllodes and metaplastic carcinomas.
We are reporting a diagnostic challenge of a case of primary breast myxofibrosarcoma and review literature on the best available evidence on diagnosis and management of primary soft tissue sarcomas of the breast.
We report a 55-year-old woman who presented with a 10-cm right breast mass. Ultrasonography (US) of the breast showed a large mainly upper outer quadrant irregular hypoechoic mass with increase internal vascularity and calcification. It measured 10 × 9 × 7 cm and no suspicious enlarged right axillary lymph node. Breast Mammography showed large irregular partially circumscribed lobulated dense mass occupy mainly upper outer quadrant, measuring 10 × 10 × 10 cm, with associated suspicious amorphous microcalcification and mild distortion and no skin thickening or nipple retraction (Figure 1). The patient initially underwent ultrasound (US) guided biopsy and pathology revealed the neoplasm composed of both epithelial and stromal components. The epithelial component was composed of benign hyperplastic ducts exhibiting pericanalicular patterns with focal leaves like pattern. These ducts were surrounded with hypercellular focally myxoid stroma, with no cytological atypia or necrosis and rare mitotic figures. Features were suggestive of benign phyllodes tumor of the breast. Based on the initial pathology of benign phyllodes tumor of the breast, the patient was offered mastectomy vs. conservative breast treatment and she opted to go with conservative approach. She underwent right wide local excision of the breast mass. Pathology of lumpectomy consisted of two lumps seen attached by fibrofatty tissue the larger measured 10 × 8 × 7 cm and the smaller measured 5 × 4.5 × 2 cm. Representative sections of both masses showed morphology consistent with malignant phyllodes tumor with lobulated fibroepithelial proliferation, increased stromal cellularity of occasionally frankly sarcomatous component and broad "leaf-like" papillae inserting into slit-like spaces. Periductal stromal condensation was seen. A moderate to marked atypia with frequent mitoses and stromal overgrowth were also seen. The borders were focally infiltrative with tumor; however, the tumor was completely excised. The epithelial cells were benign with scant peripheral breast tissue showing fibrocystic changes (Figure 2).
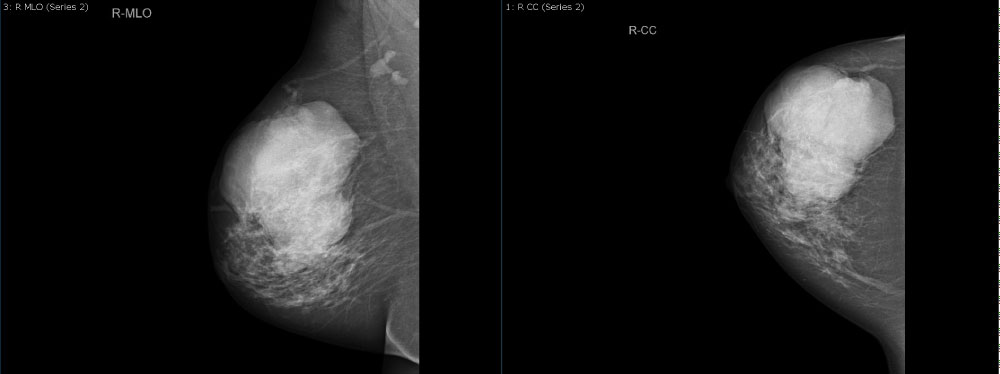 Figure 1: Mammography of the right breast showed large irregular partially circumscribed lobulated dense mass occupying the upper outer quadrant with associated suspicious amorphous microcalcification and mild distortion. View Figure 1
Figure 1: Mammography of the right breast showed large irregular partially circumscribed lobulated dense mass occupying the upper outer quadrant with associated suspicious amorphous microcalcification and mild distortion. View Figure 1
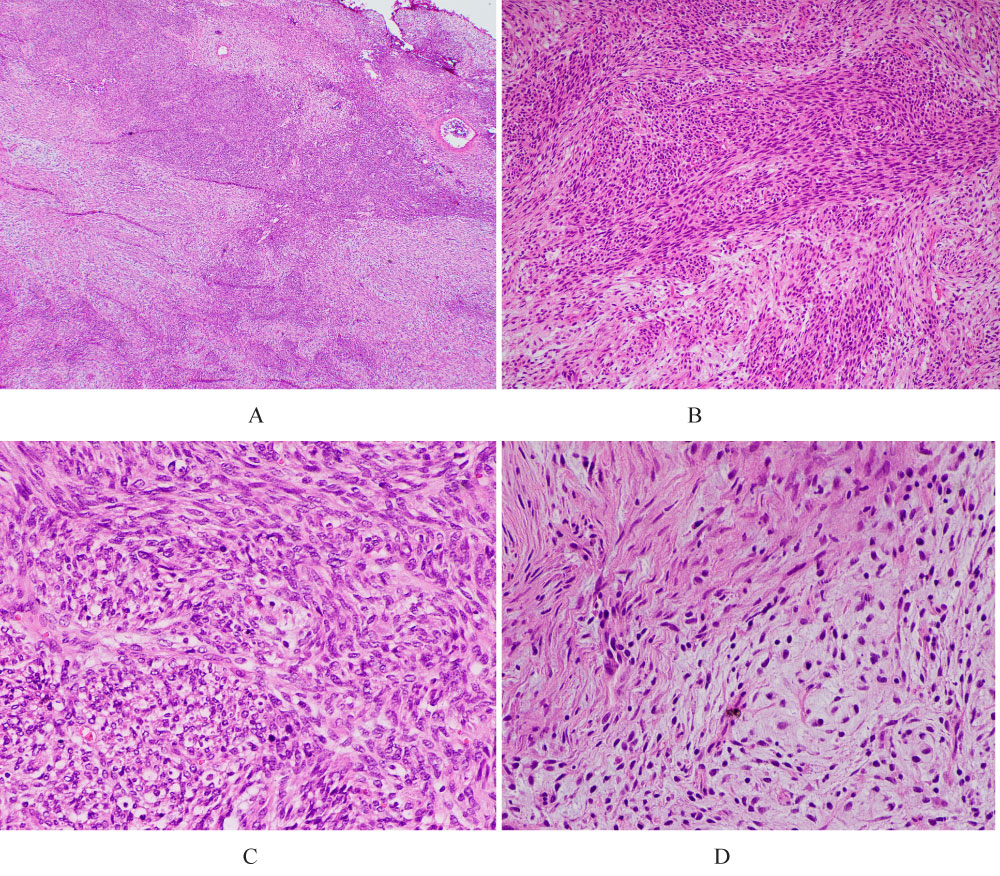 Figure 2: Photomicrograph of low and high power of the tumor with hematoxylin-eosin staining (H&E):
Figure 2: Photomicrograph of low and high power of the tumor with hematoxylin-eosin staining (H&E):
A) H&E low-power picture shows highly cellular spindle cell neoplasm with different areas of variable cellularity.
B) H&E medium-power picture showing fascicles of spindle cells neoplasm with myxoid areas.
C) H&E high-power picture showing mild-moderate nuclear atypia with mitosis and apoptotic cells.
D) H&E high-power picture showing the spindle cells with myxoid stroma. View Figure 2
One month later, she underwent completion of simple mastectomy with no evidence of residual disease and patient declined adjuvant radiotherapy.
Two months later, she presented with swelling at the lateral part of her right chest wall. Core biopsy was done from the mass and pathology revealed evidence of spindle cell neoplasm consistent with recurrence.
She went for complete surgical excision of the new developed right chest wall mass. A diagnosis of myxofibrosarcoma of the breast was confirmed by histologic examination. The immunohistochemical stains showed the following: SMA positive in the spindle cell component, CD99 paranuclear positive reaction, CD34 highlighted rich capillary network in myxoid areas, and BCL-2, CK, Desmin, ALK-1, and P-63 were negatives and Ki-67 was low of < 1%. Further sections were reexamined from the previous mastectomy and confirmed by histologic examination that the tumor had two components: The largest was malignant phyllodes tumor as described earlier and the smallest tumor was consistent with intermediate grade myxofibrosarcoma, which suggest a heterogenous sarcomatous element in a malignant phyllodes tumor.
Patient underwent adjuvant radiotherapy to the chest wall of 66 Gy in 33 fractions over 6.5 weeks with conformal radiation technique.
Primary breast sarcoma, excluding phyllodes tumor of breast is an extremely rare and constituting less than 1% of all primary breast malignancies. Primary breast sarcomas always present as breast lumps which are clinically and radiological can mimic breast fibroadenomas. These tumors are usually carry a high risk of recurrence and worse prognosis than primary adenocarcinoma of the breast. Core or excisional biopsy of the breast can differentiate this histology from other primary breast neoplasms. Due to the extreme rarity as a primary breast neoplasm, it requires to rule out more common breast primary neoplasms such as sarcomatoid carcinoma and cystosarcoma phyllodes of the breast.
The published literatures on this disease are limited to small retrospective case reviews and case reports. There is no definitive consensus regarding optimal diagnosis and management of this entity of primary breast malignancy. Staging is based on the 7th edition of American Joint Committee on Cancer (AJCC) for soft tissue sarcoma (STS), which incorporates histologic grade, tumor size, node status, and distant metastases. Data from the Surveillance, Epidemiology, and End Results (SEER) program and performed analysis showed; tumor size, lymph node involvement, distant metastasis and histologic grade were associated with poor survival outcomes [8].
The optimal treatment is not well defined for primary sarcoma of the breast, and current recommendations are extrapolated from other STS data [9]. Complete surgical resection with negative margins is strongly recommended. The optimal surgical approach can be achieved with breast conservative surgery (BCS) versus simple mastectomy. In most cases, it is possible to achieve negative wide margins with BCS. The incidence of lymph nodes metastasis in soft tissue sarcomas are extremely rare, therefore lymph nodes dissection is not recommended as standard of practice unless clinically or radiologically suspicious. The role of chemotherapy in non-metastatic disease is not well documented. Adjuvant radiotherapy should be recommended to improve local control in cases in which the tumors are large (≥ 5 cm) or in tumors with positive surgical margins as extrapolated from data on other STS [2,10]. Some retrospective data support the use of dose escalation of adjuvant radiotherapy of at least 60 GY to tumor bed, which significantly improve the disease specific survival [2].
A primary myxofibrosarcoma of the breast is a subtype of soft tissue sarcoma. The key features of this tumor are spindle cell proliferation with a moderate degree of nuclear pleomorphism, myxoid stroma and curvilinear blood vessels. Primary breast sarcomas constitute a specific clinicopathologic entity that carry different prognosis and, therefore should be differentiated from cystosarcoma phyllodes and metaplastic carcinomas. Central pathology review and multidisciplinary approach should be considered in management of such cases.