Metastases to the foot bones are uncommon and they mimic inflammatory conditions. Acrometastases may be the first manifestation of an unknown primary malignant disease. We report a case in which the first sign of lung adenocarcinoma was a pathological fracture due to metastasis to a proximal toe phalanx. A 68-year-old man was evaluated for pain in his fifth toe of the left foot after a trauma. Biopsy and immunohistochemistry reactions confirmed the metastatic lesion. Unfavorable clinical course and imaging exams showed advanced disease. A review of the literature indicates that acrometastases should be well-thought-out in aging patients complaining of foot pain and presenting osteolytic lesions.
Acrometastasis, Metastasis to foot, Lung adenocarcinoma
Measurements of length: centimeter (cm)
CK7: Cytokeratin 7; CK20: Cytokeratin 20; TTF-1: Thyroid Transcription Factor
Acrometastases (from the Greek akros, meaning extreme) are secondary malignant neoplasms that affect the bones of hands or feet [1]. Metastatic involvement of the bones of the foot is unusual [2]. Although the metastatic disease of the foot is rare, it is important to have it considered because it may be the first clinical manifestation of an occult tumor [1,2]. Secondly, acrometastases can mimic benign conditions and mislead the treatment [3]. And finally, it indicates an unfavorable prognosis and poor survival rate [1-3].
About 30% of all individuals with cancer develop metastasis to the skeleton and only 0.007% to 0.3% to the bones of hands and feet [4]. However, in the last decades, cancer has been undergoing an epidemiological transition into becoming a chronic disease what increases the chances of metastases [4].
We present a rare case of a lung adenocarcinoma metastatic lesion to a toe diagnosed and treated in a high complexity Brazilian hospital.
A 68-year-old man has a history of marked pain in the fifth toe of the left foot after minor trauma. He has smoked one pack of cigarettes per day for 55 years. On examination, he has moderate local swelling and bruising. A closed fracture is diagnosed and treated. Four months later, the patient complains of erythema, warmth, edema, and pain in the broken toe. The physical exam shows skin and soft tissue necrosis. Osteomyelitis is suspected and the patient is referred to hospital care. A radiograph shows an osteolytic lesion in the proximal phalange of the fifth toe. No periosteal reactions are present (Figure 1). A bone biopsy specimen is obtained and microscopic examination shows large, hyperchromatic, pleomorphic epithelial cells arranged in solid and tubular growth-pattern consistent with metastatic adenocarcinoma (Figure 2). The neoplastic cells marked with CK7+ and CK20+ and TTF-1+ (Figure 3) appointing to an occult lung adenocarcinoma. On following diagnostic workup, a chest radiograph shows a 3-cm round lesion in the right lower lobe (Figure 4A) and an axial chest CT scan confirms the highly suspicious for malignancy spiculated borders nodule in the right lung (Figure 4B) and pre-tracheal lymph node enlargement (Figure 4C). Over the next 2 months, he appears agitated and has seizures with episodes of transient loss of consciousness. Brain MRI shows two solid, 1- to 3-cm mass lesions, without enhancement of surrounding edema, located at the gray-white junction in the left frontal and occipital lobes consistent with metastasis (Figure 4D).
 Figure 1: Radiograph of the left foot. A diminished density is seen in the proximal phalange of the fifth toe. It displays an osteolytic appearance. No signs of consolidation after a 4-month-old fracture. View Figure 1
Figure 1: Radiograph of the left foot. A diminished density is seen in the proximal phalange of the fifth toe. It displays an osteolytic appearance. No signs of consolidation after a 4-month-old fracture. View Figure 1
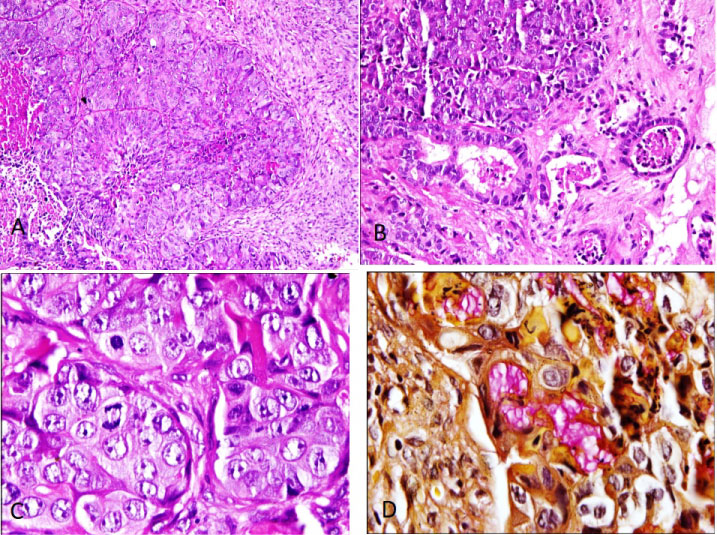 Figure 2: Acrometastasis to foot. A) Nests of malignant epithial cells, comedo necrosis and desmoplasic stroma; B) Tubular formations are present; C) High grade nucleis and mitotic activity are feature; D) Mucus is highlighted by mucicarmin stain. View Figure 2
Figure 2: Acrometastasis to foot. A) Nests of malignant epithial cells, comedo necrosis and desmoplasic stroma; B) Tubular formations are present; C) High grade nucleis and mitotic activity are feature; D) Mucus is highlighted by mucicarmin stain. View Figure 2
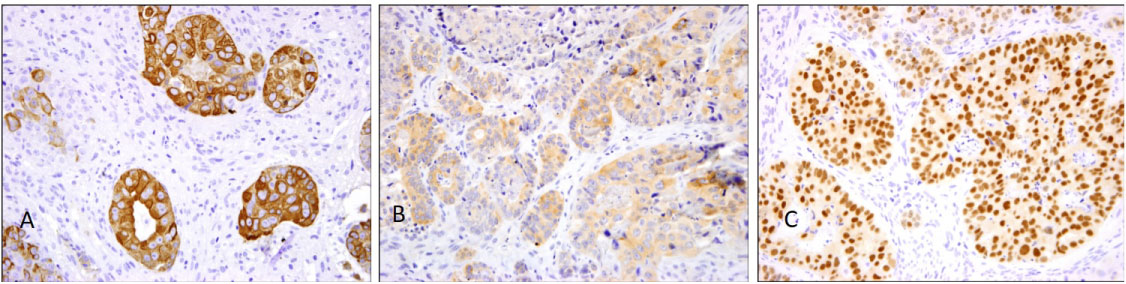 Figure 3: Lung adenocarcinoma immunohistochemestry profile. A) Neoplastic cells mark for CK7strongly and diffusely; B) CK20 stainnig is weaker; C) Nuclear positivity for TTF-1. View Figure 3
Figure 3: Lung adenocarcinoma immunohistochemestry profile. A) Neoplastic cells mark for CK7strongly and diffusely; B) CK20 stainnig is weaker; C) Nuclear positivity for TTF-1. View Figure 3
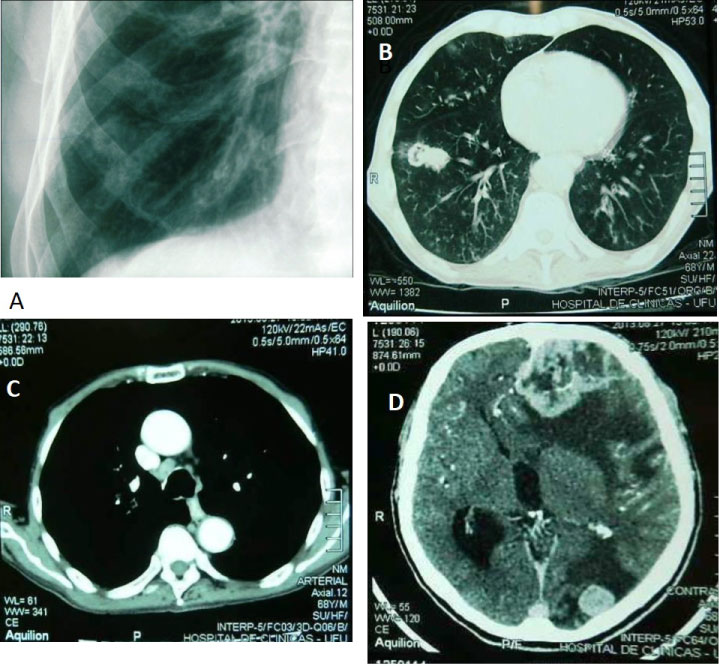 Figure 4: Imaging exams. A) A chest radiograph features a nodular mass in the right lower lobe; B) A chest CT scan reveals a nodule with spiculated borders in the right lung; C) Pre-tracheal lymph node enlargement suspicious for secondary involvement; D) Brain MRI shows two solid lesions located at the gray-white junction in the left frontal and occipital lobes. View Figure 4
Figure 4: Imaging exams. A) A chest radiograph features a nodular mass in the right lower lobe; B) A chest CT scan reveals a nodule with spiculated borders in the right lung; C) Pre-tracheal lymph node enlargement suspicious for secondary involvement; D) Brain MRI shows two solid lesions located at the gray-white junction in the left frontal and occipital lobes. View Figure 4
In a brief historical summary, the first case of acrometastasis involving the bones of the hand by a breast carcinoma was reported in 1906 [2]. However, the first metastasis to foot bone was published in a series of cases of bone tumors in 1920 [5,6]. In 1982, a literature review identified 72 cases of peripheral metastases to the foot bones but only 38 cases were histologically diagnosed [6,7]. In over 40 years of work, there have not been records on acrometastasis in this pathology laboratory.
Many hypotheses have been proposed in the pathogenesis of acrometastases. However, there is no consensus regarding the exact mechanism [2,5]. Increased blood flow and trauma are mentioned as important risk factors [8]. For instance, statistical data show a higher frequency of metastases to the bones of the dominant hand compared to the non-dominant hand [2,5,9]. The latter receives less blood flow and is less prone to trauma. The metastatic site can be predicted by the location of the primary neoplasm. Thus, bronchogenic carcinomas would tend to metastasize to the hand bones, and breast carcinomas would have a similar preference for hands and feet, and gastrointestinal tumors would rather metastasize to the foot bones [5]. In other words, supradiaphragmatic malignant tumors tend to affect the hand bones as infradiaphragmatic malignancies do to the bones of the foot. Genitourinary cancers (renal, bladder, prostate, and testicular carcinomas) hardly ever produce acrometastases [5]. Local temperature, hormonal effects, and immune response also appear to participate in the metastatic cascade and the adhesion of tumor emboli to certain sites [2,5]. We believe in multifactorial pathogenesis and that some tumors show organ tropism. In our case, neoplastic emboli from a lung adenocarcinoma could have fallen into the systemic circulation through: 1) The wall of the pulmonary capillaries and/or 2) Through the lymphatic vessels that led them to the systemic venous system.
Once acrometastasis is developed in a foot bone, its erosive and destructive growth leads to local manifestations such as pain and edema and drainage [10,11]. Diagnosis of acrometastasis is challenging and generally constitutes an advanced disease with poor prognosis [12]. The clinical picture can lead to misdiagnosis of traumatic fracture, osteomyelitis, septic arthritis, gout, ischemic necrosis, and diabetic foot and lead to inadequate treatment and delayed diagnosis of occult cancer. In our case, bone fracture masked any signs of metastasis at the visit four months ago.
When an acrometastasis is suspected, a comprehensive staging is needed to define the primary tumor, its extension, and prognosis [13]. Concurrent multidisciplinary care reliefs the pain and improves mobility [14].
In conclusion, we describe a case of extensive lung adenocarcinoma with acrometastatic disease to the foot bones. Our patient also developed metastatic lesions in the mediastinal lymph node and brain. Our case highlights the need to consider an acrometastasis in an adequate clinical scenario and the importance of a biopsy. Material collection for pathological study should be performed promptly and further immunohistochemistry techniques can accurately define the site of the primary lesion.
Candeloro, I collected data, reviewed the literature, conducted the immunohistochemical reactions and wrote the manuscript; Dornelas, BC designed the project, collected data, reviewed the literature, wrote and revised the manuscript. All authors have read and approved the final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing interests.
The authors declare that they have no funding.